
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 6
Occult liver abscess presenting as septic shock following common bile duct stent removal: A rare post-ERCP complication
Anmol Saini; Nitin Rustogi; Sandeep Lamoria; Preeti Rajpoot; Vaishali Bhardwaj*
Department of Gastroenterology, ABVIMS and DR RML Hospital, New Delhi, India.
*Corresponding Author : Vaishali Bhardwaj
Department of Gastroenterology, ABVIMS and DR
RML Hospital, New Delhi, India.
Email: drvaishali22.db@gmail.com;
drvaishali22@ymail.com
Received : Apr 13, 2026
Accepted : May 22, 2026
Published : May 29, 2026
Archived : www.jjgastro.com
Copyright : © Bhardwaj V (2026).
Abstract
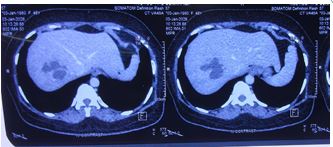
Endoscopic Retrograde Cholangiopancreatography (ERCP) with biliary stenting is routinely performed for choledocholithiasis, and stent removal is generally considered safe. Severe infectious complications following biliary stent removal are rarely described. We report the case of a 46-year-old female who developed acute febrile illness, rapidly progressive jaundice, septic shock, and hypoxemic respiratory failure within hours of elective Common Bile Duct (CBD) stent removal. Initial ultrasonography did not reveal biliary obstruction or hepatic pathology, and blood cultures remained sterile. Despite early antimicrobial therapy and supportive care, the patient developed worsening liver biochemistry and hemodynamic instability requiring vasopressor support and non-invasive ventilation. Computed Tomography Pulmonary Angiography (CTPA) incidentally detected a hepatic lesion subsequently confirmed as a liver abscess. Imaging demonstrated a uniloculated segment VII liver abscess measuring 3.8×5.2×3.6 cm (approximately 40 cc). The patient was successfully managed with broad-spectrum antimicrobial therapy and intensive supportive care without percutaneous drainage, achieving complete clinical and biochemical recovery.
Citation: Saini A, Rustogi N, Lamoria S, Rajpoot P, Bhardwaj V. Occult liver abscess presenting as septic shock following common bile duct stent removal: A rare post-ERCP complication. J Gastroenterol Res Pract. 2026; 6(3): 1253.
Introduction
ERCP remains a cornerstone in the management of pancreaticobiliary disorders, particularly choledocholithiasis. Although generally safe, complications such as pancreatitis, bleeding, perforation, and cholangitis are well recognized [1,2]. Pyogenic Liver Abscess (PLA) is an uncommon but serious complication associated with biliary pathology and instrumentation [3,4]. Liver abscess following biliary stent removal is exceedingly rare and poorly described in the literature.
Case presentation
A 46-year-old female with no comorbidities underwent elective CBD stent removal following prior ERCP for choledocholithiasis and open cholecystectomy. Baseline laboratory investigations were normal (total/direct bilirubin 0.35/0.05 mg/dL; AST/ALT/ALP 31/26/130 IU/L). The procedure was uneventful.
Post-procedural course
Approximately 8 hours after stent removal, the patient developed fever with chills, followed by progressive jaundice and dyspnea. Rapid deterioration occurred with hypotension and hypoxemia, necessitating vasopressor support and ICU admission. Non-invasive ventilation was required for 24 hours.
Investigations
Repeat laboratory studies showed total/direct bilirubin 14/8.2 mg/dL and ALT/AST/ALP 348/251/320 IU/L. Peak leukocyte count was 17,760/mm³. CRP was 20.6 mg/L and serum procalcitonin was positive. Blood cultures remained sterile. Initial ultrasonography was normal. CTPA excluded pulmonary embolism but incidentally revealed a hepatic lesion. Repeat ultrasonography confirmed a uniloculated segment VII liver abscess measuring 3.8×5.2×3.6 cm (~40 cc).
Management
Initial therapy included ceftriaxone and ofloxacin. With progression to septic shock, antibiotics were escalated to meropenem and vancomycin, and metronidazole was added after abscess detection. Conservative management was pursued without drainage. Total antibiotic duration was 16 days.
Outcome
The patient improved clinically with resolution of fever and stabilization of hemodynamics. Repeat ultrasonography before discharge showed reduction of abscess volume from 40 cc to 22 cc. The patient was discharged in stable condition after 21 days of hospitalization.
Discussion
Pyogenic liver abscess most commonly arises from biliary tract disease, portal venous seeding, or systemic bacteremia [3]. ERCP-related abscess formation is rare but recognized, particularly in the presence of biliary obstruction, sphincterotomy, or indwelling stents [4]. The present case is notable because abscess formation occurred following stent removal in a previously asymptomatic patient with normal baseline liver function tests.
Several pathophysiological mechanisms may explain this phenomenon. Biliary stents are prone to biofilm formation, which may harbor pathogenic bacteria [7,8]. Mechanical manipulation during stent removal may dislodge colonized material into the biliary tree, facilitating ascending infection. Instrumentation may transiently disrupt mucosal integrity and promote bacterial translocation into the portal circulation. Even without overt obstruction, transient papillary edema or micro stasis may predispose to infection.
The rapid onset of septic shock within eight hours suggests either acute bacterial dissemination or a robust systemic inflammatory response. Blood cultures remained sterile, which does not exclude localized hepatobiliary infection. Elevated procalcitonin and leukocytosis supported a bacterial etiology despite negative cultures.
A key learning point is the limitation of early ultrasonography. Small or evolving abscesses may not be visualized initially. Computed tomography is more sensitive for detecting hepatic collections and should be considered when suspicion persists despite negative ultrasound findings [5,6].
Management traditionally includes antimicrobial therapy combined with image-guided drainage for larger collections. However, selected uniloculated abscesses smaller than 5 cm may respond to antibiotics alone [9]. In this case, conservative therapy resulted in radiologic regression and complete clinical recovery, supporting individualized management strategies.
This case underscores the need for high clinical suspicion for occult hepatobiliary infection following biliary interventions, even when early investigations are non-revealing.
Conclusion
Septic shock following CBD stent removal is rare but may signify occult liver abscess. Persistent clinical suspicion and timely cross-sectional imaging are crucial for diagnosis and favorable outcomes.
References
- Chandrasekhara V, Khashab MA, Muthusamy VR, et al. Adverse events associated with ERCP. Gastrointest Endosc. 2017; 85: 32–47.
- Andriulli A, Loperfido S, Napolitano G, et al. Incidence rates of post-ERCP complications. Am J Gastroenterol. 2007; 102: 1781 1788.
- Longworth S, Han J. Pyogenic liver abscess. Clin Liver Dis. 2015; 6: 51–54.
- Wu CK, Hsu CY, Chen YC, et al. Increased risk of pyogenic liver abscess after sphincterotomy. Infect Drug Resist. 2021; 14: 2121–2131.
- Halvorsen RA, Korobkin M, Foster WL, et al. CT appearance of hepatic abscesses. AJR Am J Roentgenol. 1984; 142: 941–946.
- Lardière-Deguelte S, Ragot E, Amroun K, et al. Hepatic abscess: diagnosis and management. J Visc Surg. 2015; 152: 231–243.
- Vaishnavi C, Samanta J, Kochhar R. Biofilm formation in biliary stents. World J Gastroenterol. 2018; 24: 112–123.
- Elsebaey MA, Enaba ME, Elashry H, et al. Forgotten biliary stents: complications and outcomes. Medicina (Kaunas). 2024; 60: 1258.
- Hope WW, Vrochides DV, Newcomb WL, et al. Optimal treatment of hepatic abscess. Am Surg. 2008; 74: 178–182.