
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 6
Dysplasia rates in sessile serrated lesions in symptomatic and screening populations
Morris Joseph G, MB, BCh, BAO, LRCPI/SI*; Al Manji Zainab, FRCPath; Sheahan Kieran, FRCPath; Gibbons David, FCAP
Department of Histopathology, St. Vincent’s University Hospital, Elm Park, Dublin 4, Ireland.
*Corresponding Author : Joseph Morris
Department of Histopathology, St. Vincent’s University
Hospital, Elm Park, Dublin 4, Ireland.
Tel: (01) 221 4000;
Email: jmorrisresearch@outlook.com
Received : Mar 27, 2026
Accepted : Apr 14, 2026
Published : Apr 21, 2026
Archived : www.jjgastro.com
Copyright : © Morris JG (2026).
Abstract
Introduction: The World Health Organisation (WHO) describes 5 subtypes of serrated colorectal lesions, with Sessile Serrated Lesions (SSLs) being distinguished by distortion of crypt architecture. Approximately 4-8% of these lesions are dysplastic and represent malignant precursor lesions with rapid progression to Colorectal Cancer (CRC), often with loss of MLH-1 expression. Subtyping dysplasia is challenging and no gold standard criteria exist. We describe rates and subtypes of dysplasia in our institution and evaluate interobserver variability in the diagnosis of dysplasia.
Methods: We identified all SSLs diagnosed in our department over a 2-year period and noted rates of dysplasia. In cases where dysplasia was not subtyped, we reviewed the slides and assigned a subtype. In the second part of the study two histopathologists reviewed dysplastic cases independently, as well as 50 controls slides, after reviewing diagnostic criteria, to assess inter-observer agreement for the prevalence and subtype of dysplasia.
Results: 1805 SSLs were identified with a dysplasia rate of 5%. 26/53 showed adenomatous dysplasia, 21/53 serrated and 6/53 mixed. There was modest agreement between pathologists, with a Cohen’s kappa coefficient (k) of 0.566.
Conclusion: Dysplasia is important to recognise given the potential rapid progression to CRC in these lesions. There are no gold standard diagnostic criteria but we were able to demonstrate modest agreement in the diagnosis and subtyping of dysplasia between pathologists in our dataset.
Keywords: Dysplasia; SSL; Sessile serrated lesion; Sessile serrated adenoma; MLH1; Interobserver variability; Colorectal carcinoma; Adenoma.
Abbreviations: WHO: World Health Organisation; SSL: Sessile Serrated Lesion; SSL-D: Sessile Serrated Lesion with Dysplasia; CRC: Colorectal Carcinoma; NOS: Not Otherwise Specified; IHC: Immunohistochemistry; TSA: Traditional Serrated Adenoma; MMR: Mismatch Repair.
Citation: Morris JG, Zainab AM, Kieran S, David G. Dysplasia rates in sessile serrated lesions in symptomatic and screening populations. J Gastroenterol Res Pract. 2026; 6(3): 1251.
Introduction
The World Health Organisation (WHO), Digestive System Tumours (5th Ed.) describes 5 subtypes of serrated colorectal lesions characterised by a serrated (sawtooth or stellate) architecture of the epithelium [1].
SSLs can be distinguished from other serrated lesions by distortion of normal crypt architecture, including horizontal growth along the muscularis mucosae and dilation of the crypt base with serrations extending to the base. The presence of ≥1 unequivocal architecturally distorted serrated crypt is diagnostic of an SSL histologically (Figure 1) [1].
These lesions account for approximately 15% of all endoscopically removed colorectal polyps that are encountered by a histopathologist in day-to-day practice, with dysplasia being present in approximately 4-8% of SSLs (SSL-D) [2-4].
Dysplasia is important to recognise as it may be a transitional step in the progression towards Colorectal Carcinoma (CRC). SSLs may be precursor lesions in 30% of CRCs, with SSL-D having a risk of rapid progression to CRC [3,5].
Subtyping dysplasia can be challenging. The subtype, and potentially grade, of dysplasia may predict malignant behaviour [3,6,7]. Serrated and adenomatous dysplasia are recognised and C Liu et al divided dysplasia into four main patterns; serrated, adenomatous, minimal deviation and Not Otherwise Specified (NOS), in an attempt to describe the spectrum of dysplastic changes seen [1,3,7-9]. SSL-D polyps are considered ‘advanced polyps’ in screening programmes (Figure 2) [10].
Minimal deviation dysplasia includes subtle changes that require loss of MLH1 expression by Immunohistochemistry (IHC) to support the diagnosis, with these lesions accounting for 19% of SSL-D which could be potentially missed by histopathologists (Figure 3).
We found that SSL-D was not always subtyped in our department. This is not uncommon in routine diagnostic practice and currently is not mandated by WHO guidelines. Some cases were graded into low- or high-grade dysplasia.
We aim to describe the rates and subtypes of dysplasia in SSLs and evaluate interobserver agreement between histopathologists.
Materials and methods
We identified SSLs by searching the local laboratory information system for all cases between 01/01/2021 and 31/12/2022. Cases were divided into 2 cohorts based on if they were initially referred for endoscopy via the National Bowel Cancer Screening Program or from a ‘symptomatic’ pathway. Traditional serrated adenomas were excluded.
In the first part of the study, we noted the total number of SSLs in each case, presence of dysplasia and location in the bowel in which they occurred. In cases where dysplasia was not subtyped in the original report (68 cases) the slides were reviewed by two histopathologists (JM and DG). 66 of these cases were available for review from file. Dysplasia was also graded (low-grade or high-grade) in this part of the study. JM and DG assigned a dysplasia subtype (serrated, adenomatous, minimal deviation dysplasia and not otherwise specified) in addition to a grade (low or high grade). Final decision was made by consensus for each case regarding dysplasia subtype.
In the second part of the study, two gastrointestinal histopathologists (ZAIS and DG) reviewed the available slides of the original 92 SSL-D cases. A total of 66 cases were available for review.
50 random non-dysplastic SSLs from the 2-year study period were also reviewed to serve as controls. The presence and subtype of dysplasia was noted. They both reviewed detailed diagnostic criteria of serrated versus adenomatous/intestinal dysplasia in SSL-D prior to review based on WHO 5th Edition criteria and descriptions in the paper by Liu et al (Figure 4) [1,3,8]. They were blinded to the original report diagnoses. Cohen’s kappa coefficient (k) was calculated to evaluate interobserver agreement.
In cases where there was disagreement between the two pathologists, either regarding the presence of dysplasia or the subtype of dysplasia present, a third senior gastrointestinal histopathologist (KS) reviewed the slides with discordant interpretations to serve as the final arbiter.
Results
Over the 2-year study period, 1805 of SSLs were identified. Of these 1805 lesions, 92 (92/1805, 5.1%) were reported as having dysplasia. There were similar levels of dysplasia between the screening cohort (9/172, 5.2%) and the symptomatic cohort (83/1633, 5.1%).
SSLs in the screening cohort were predominantly right sided, accounting for 90 (90/172, 52%) lesions (transverse 41/172, 24%, left side 41/172, 24%). SSLs were also predominantly right sided in the symptomatic cohort, totalling 859 (859/1633, 52.5%) lesions (transverse 459/1633, 28%, left side 313/1633, 19%). A location was not provided in 2 (2/1633, 0.12%) lesions in the original report.
We found that SSL-D was not always subtyped in our department. Dysplasia was not subtyped in the original report of 68 SSL-D and these cases were reviewed by two histopathologists (JM and DG) and a subtype assigned. 66 H+E slides were available for review. Dysplasia subtypes among the 92 SSL-D in the first part of the study are outlined in (Table 1).
In the screening cohort, 3/9 (33.3%) SSL-D patients were male and mean age was 65.4 years (Range 60-70). In the symptomatic cohort, 35/83 (42.2%) were male with mean age of 65.7 years (Range of 31-90).
In the second part of the study, two gastrointestinal histopathologists reviewed the available slides of the original 92 SSL-D cases. They first received education on dysplasia subtyping based on WHO 5th Edition criteria and descriptions in the paper by Liu et al [1,3,8].
One case was reclassified as a tubular adenoma on review and subsequently excluded from the analysis.
Among the remaining 115 cases, Pathologist 1 classified 58/115 (50.4%) of the lesions as SSL-D and Pathologist 2 classified 49/115 (42.6%) as SSL-D. There was a moderate level of agreement regarding the diagnosis of SSL-D, with a Cohen’s kappa coefficient (k) of 0.566.
Of the 115 reviewed cases, 42 cases were identified where diagnosis could not be agreed between the two pathologists and these cases were reviewed by a third gastrointestinal pathologist.
Of the cases with discrepancies, 11 were reclassified as SSL without dysplasia, and one case was classified as SSL with serrated dysplasia.
After review, 26 cases demonstrated adenomatous dysplasia, 21 demonstrated serrated dysplasia and 6 demonstrated mixed dysplasia (Table 2). Adenomatous dysplasia was generally easier to diagnose in our experience given the morphologic similarities with dysplasia seen in conventional adenomas.
Of the 66 cases which had originally been classified as SSL-D that were reviewed, only 53 were deemed to be truly dysplastic by senior GI pathologists and review of diagnostic criteria as laid out in on WHO 5th Edition and based on the descriptions in the paper by Liu et al [1,3,8].
The age of these patients with SSL-D ranged from 31 to 92 years, with an average age of 66.7 years. 34/53 (64%) were female. Two patients had a known history of Sessile Serrated Polyposis (SSP) and one patient had a diagnosis of Lynch syndrome. There was a right-side predilection with the most common site of SSL-D being the ascending colon (23/53, 43%), followed by transverse colon (12/53, 22.6%).
We attempted to grade dysplasia in our study. 52/53 (98%) showed low-grade dysplasia and 1/53 (2%) showed high-grade dysplasia.
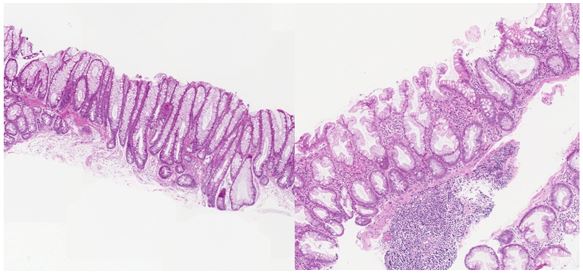

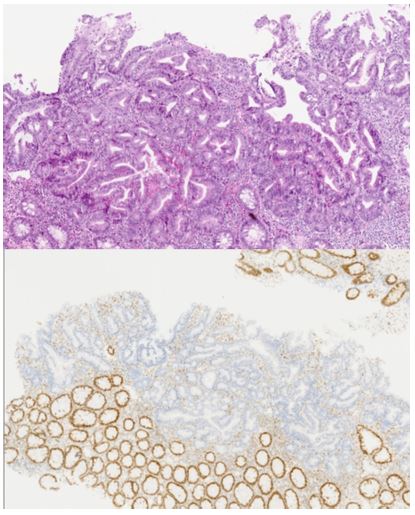
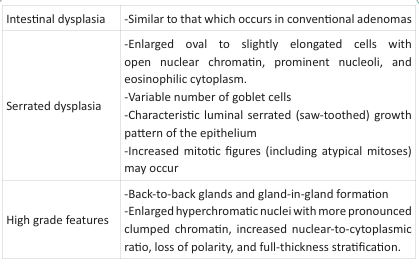
Table 1: Dysplasia subtypes in 92 SSL-D.
| Dysplasia subtype | Number of lesions |
|---|---|
| Low-grade, adenomatous | 52/92 (56.5%) |
| Low-grade, serrated | 32/92 (34.8%) |
| High-grade, adenomatous | 4/92 (4.3%) |
| Low-grade, adenomatous with TSA like areas | 1/92 (1.1%) |
| Low-grade, serrated and adenomatous | 2/92 (2.2%) |
| Low-grade, Not Otherwise Specified (NOS) | 1/92 (1.1%) |
Table 2: Dysplasia subtypes in 53 SSL-D, after review by senior GI pathologist.
| Dysplasia subtype | Number of lesions |
|---|---|
| Adenomatous | 26/53 (49.1%) |
| Serrated | 21/53 (39.6%) |
| Mixed | 6/53 (11.3%) |
Discussion
Serrated colorectal lesions are characterised by a serrated (sawtooth or stellate) architecture of the epithelium [1]. Until 2010, with the release of WHO 4th Edition criteria, these were generally considered low risk lesions with little malignant potential, despite rare cases showing progression [8,11-13]. The WHO 5th Edition currently describes 5 subtypes of serrated colorectal polyps: hyperplastic polyps, TSAs, unclassified serrated adenomas, SSLs and SSL-D with SSL/SSL-D and TSAs having a risk of progression to CRC [1].
SSL-D’s are much less frequently encountered than SSL’s. We report a dysplasia rate of approximately 5% in SSL’s over a 2 year period, which is in keeping with internationally reported rates of 4-8% [2]. SSL’s and SSL-D’s are more frequently found on the right side of the colon but, when encountered, left sided SSLs are reported to have higher rates of dysplasia than their right sided counterparts [2,14-16]. We found that most SSL-D’s occurred on the right side of the colon, with 23/53 (43%) occurring in the ascending colon and 12/53 (22.6%) in the transverse.
There was no difference in rates of SSL’s, their rates of dysplasia or distribution in the colon between the screening and symptomatic cohorts.
In the first part of our study, we found that dysplasia subtype was frequently not included in reports in our centre (68/92 (74%)). The WHO, Digestive System Tumours (5th Ed.) describes both intestinal/adenomatous and serrated dysplastic changes which may be present in SSL-D’s but does not provide a definitive subclassification system or strict diagnostic criteria. It is also recognised that multiple morphological patterns of dysplasia can occur in a single lesion [1].
Ours is not the first study to attempt to standardise the subclassification system for SSL-D’s. Cenaj et al, in a study including 86 patients with SSL-D, divided lesions into serrated dysplasia (50/86, 58%), adenomatous dysplasia (22/86, 25%) and mixed dysplasia (14/86, 16%). In comparison, our study found adenomatous dysplasia to be the most common dysplasia subtype in SSL-D (26/53, 49%) [9].
They divided lesions into low- and high-grade. They found that high-grade lesions had higher mean patient age, higher mean polyp size and a higher prevalence of adenocarcinoma within the polyp than low-grade lesions [9]. In our study, we found 1/53 (2%) SSL-D to harbour high grade dysplasia without containing invasive carcinoma. Current guidance, as per the WHO, is not to grade these lesions, arguing poor reproducibility due to the heterogeneity of histological changes seen in dysplastic lesions [1,3,17].
The significance of grade remains undetermined. A study by Sugai et al argued that the highest risk of progression to CRC in SSL-D was an association with Mismatch Repair (MMR) protein inactivation. They too divided lesions into serrated and adenomatous dysplasia and graded the dysplasia seen. Interestingly, and in contrast to Cenaj et al. they found that serrated dysplasia was associated with an increased risk of malignant transformation compared with intestinal dysplasia in their study of 54 SSL-D’s [7,9].
Loss of MLH1 expression in SSL crypts, even in the absence of conventional dysplasia, may precede the development of adenocarcinoma and represents an advanced serrated lesion [18].
MLH1 IHC was only available for 14/92 (15%) of SSL-D in our series. Loss of expression was seen in 2 lesions (2/92), both with low-grade serrated dysplasia apparent on H+E stains. Loss of MLH1 expression may be seen even in cases with only subtle morphologic changes suggestive of dysplasia, such as in “minimal deviation” dysplasia described by Liu et al. [3]. The cost-benefit of universal MLH1 testing remains to be determined [19].
We found that after a brief period of education, modest agreement between pathologists could be achieved, with a Cohen’s Kappa Coefficent (k) of 0.56. In a study looking at data from the Dutch Pathology Registry (PALGA) in 2014 and 2015, they noted substantial interlaboratory variability in the diagnosis of SSL vs hyperplastic polyps. After implementation of a mandatory e-learning module this variability significantly decreased and they argued that education and consensus meetings can be used to improve interobserver agreement between pathologists [20].
Conclusion
The spectrum of changes in SSL-D’s is wide and ranges from subtle architectural and cytological features to evident villous, crowding or complex architecture and atypical nuclear features [1]. Dysplasia is important to recognise given risk of progression to CRC [1,3,9,17]. There are no gold-standard criteria widely used currently to subtype dysplasia in these lesions [3,7,9]. We have shown that, through review of diagnostic criteria, diagnosis of these lesions can be reproducible among GI pathologists. Standardised education, the use of GI pathology consensus meetings and the more widespread use of molecular adjuncts could all serve as methods to improve interobserver agreement between pathologists [3,8,21].
References
- Pai RRC, Makinen M. Colorectal serrated lesions and polyps. In: WHO Classification of Tumours, Digestive System Tumours. 5th ed. International Agency for Research on Cancer; Available from: https://tumourclassification.iarc.who.int/chaptercontent/31/57
- Yang JF, Tang SJ, Lash RH, Wu R, Yang Q. Anatomic distribution of sessile serrated adenoma/polyp with and without cytologic dysplasia. Arch Pathol Lab Med. 2015; 139: 388-93.
- Liu C, Walker NI, Leggett BA, Whitehall VL, Bettington ML, Rosty C. Sessile serrated adenomas with dysplasia: morphological patterns and correlations with MLH1 immunohistochemistry. Mod Pathol. 2017; 30: 1728-38.
- IJ JE, de Wit K, van der Vlugt M, Bastiaansen BA, Fockens P, Dekker E. Prevalence, distribution and risk of sessile serrated adenomas/polyps at a center with a high adenoma detection rate and experienced pathologists. Endoscopy. 2016; 48: 740-6.
- Bettington M, Walker N, Rosty C, Brown I, Clouston A, McKeone D, et al. Clinicopathological and molecular features of sessile serrated adenomas with dysplasia or carcinoma. Gut. 2017; 66: 97-106.
- Cenaj O, Gibson J, Odze RD. Clinicopathologic and outcome study of sessile serrated adenomas/polyps with serrated versus intestinal dysplasia. Mod Pathol. 2018; 31: 633-42.
- Sugai T, Uesugi N, Osakabe M, Yao T, Yanagawa N, Ajioka Y. Characterization of sessile serrated adenomas with dysplasia including intramucosal adenocarcinoma and colorectal carcinoma with a microsatellite instability phenotype. Hum Pathol. 2024; 145: 9-15.
- Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO classification of tumours of the digestive system. 2010.
- Cenaj O, Gibson J, Odze RD. Clinicopathologic and outcome study of sessile serrated adenomas/polyps with serrated versus intestinal dysplasia. Mod Pathol. 2018; 31: 633-42.
- Rutter MD, East J, Rees CJ, Cripps N, Docherty J, Dolwani S, et al. British Society of Gastroenterology/Association of Coloproctology of Great Britain and Ireland/Public Health England post-polypectomy and post-colorectal cancer resection surveillance guidelines. Gut. 2020; 69: 201-23.
- Crockett SD, Nagtegaal ID. Terminology, molecular features, epidemiology, and management of serrated colorectal neoplasia. Gastroenterology. 2019;157:949-66.e4.
- Booth AL, Taggart MW, Ono Y, Gonzalez RS. From mixed hyperplastic/adenomatous polyp to sessile serrated lesion: a long and winding road for long and winding crypts. Arch Pathol Lab Med. 2020;145:1289-96.
- Mezzapesa M, Losurdo G, Celiberto F, Rizzi S, d’Amati A, Piscitelli D, et al. Serrated colorectal lesions: an up-to-date review from histological pattern to molecular pathogenesis. Int J Mol Sci. 2022;23:8.
- Meester RGS, van Herk M, Lansdorp-Vogelaar I, Ladabaum U. Prevalence and clinical features of sessile serrated polyps: a systematic review. Gastroenterology. 2020;159:105-18.e25.
- Jung P, Kim HW, Park SB, Kang DH, Choi CW, Kim SJ, et al. Clinical and endoscopic characteristics of sessile serrated lesions with dysplasia/carcinoma. Korean J Intern Med. 2023;38:349-61.
- Răduţă D, Dincă OM, Micu GV, Nichita L, Cioplea MD, Buşcă RM, et al. MLH1, BRAF and p53: searching for significant markers to predict evolution towards adenocarcinoma in colonic sessile serrated lesions. Rom J Morphol Embryol. 2021;62:971-9.
- O’Brien MJ, Zhao Q, Yang S. Colorectal serrated pathway cancers and precursors. Histopathology. 2015;66:49-65.
- Yozu M, Kem M, Cenaj O, Mino-Kenudson M, Odze RD, Misdraji J. Loss of expression of MLH1 in non-dysplastic crypts is a harbinger of neoplastic progression in sessile serrated adenomas/polyps. Histopathology. 2019;75:376-84.
- Angerilli V, Vink-Börger ME, van Roermund NS, van Lijnschoten G, Kuijpers CCHJ, van Grieken NCT, et al. Dysplasia in sessile serrated lesions: frequency, interobserver variability and added value of immunohistochemistry. Histopathology. 2026.
- Ijspeert JEG, Madani A, Overbeek LIH, Dekker E, Nagtegaal ID. Implementation of an e-learning module improves consistency in the histopathological diagnosis of sessile serrated lesions within a nationwide population screening programme. Histopathology. 2017;70:929-37.
- Pai RK, Bettington M, Srivastava A, Rosty C. An update on the morphology and molecular pathology of serrated colorectal polyps and associated carcinomas. Mod Pathol. 2019;32:1390-415.