
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 6
Activated partial thromboplastin time-charlson comorbidity index score as a predictor of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt
Lingyi Zhu1,2#; Qi Huang1,2#; Zijian Zhu1,2#; Chaoming Huang1,2; Yeyu Zhang2; Shiman Zhu2; Shiji Fang2,3; Lili Yang2; Fazong Wu2; Min Xu2,3; Minjiang Chen2,3; Zhongwei Zhao1-3*; Jiansong Ji1-3*; Liyun Zheng1-3*
1Lishui Joint Training Base, Zhejiang Chinese Medical University, China.
2Zhejiang Key Laboratory of Imaging and Interventional Medicine, the Fifth Affiliated Hospital of Wenzhou Medical University,
China.
3Clinical College of The Affiliated Central Hospital, School of Medicine, Lishui University, China.
#These authors have been equally contributed to this article.
*Corresponding Author : Liyun Zheng, MD, PhD,
Jiansong Ji, MD, PhD & Zhongwei Zhao, MD, PhD
Zhejiang Key Laboratory of Imaging and Interventional
Medicine, the Fifth Affiliated Hospital of Wenzhou
Medical University, 323000, China.
Tel: +86 0578 2285011;
Email: Zhengliyun@wmu.edu.cn; jjstcty@wmu.edu.cn;
Zhaozw79@163.com
Received : Feb 20, 2026
Accepted : Mar 11, 2026
Published : Mar 18, 2026
Archived : www.jjgastro.com
Copyright : © Zhao Z, Ji J, Zheng L (2026).
Abstract
Objective: The study aimed to retrospectively evaluate the predictive value of the Activated Partial Thromboplastin Time-Charlson Comorbidity Index (APTT-CCI) score for Hepatic Encephalopathy (HE) following Transjugular Intrahepatic Portosystemic Shunt (TIPS).
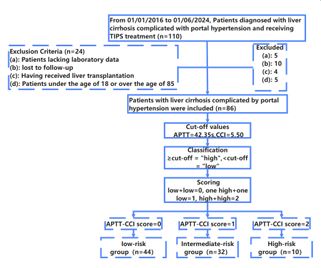
Methods: A total of 86 cirrhotic patients with portal hypertension who underwent TIPS at Lishui Central Hospital between 01/01/2016 and 01/06/2024 were included. The Youden index for APTT and CCI was used to determine optimal cutoff values. Based on the binary classification of APTT and CCI, patients were categorized into three groups: low-risk, intermediate-risk, and high-risk. The area under the curve of the APTT-CCI score was calculated to evaluate its predictive accuracy for HE. The median time to HE development was compared. Multivariate Cox regression analysis was performed to identify independent risk factors for post-TIPS HE and overall survival.
Results: The optimal cutoff values for APTT and CCI were 42.35 s and 5.50, respectively. The APTT-CCI score showed good predictive performance for post-TIPS HE, with AUC values of 0.79 (95% CI: 0.69-0.90), 0.82 (95% CI: 0.71-0.93), and 0.84 (95% CI: 0.74-0.94) for 1-year, 2-year, and 3-year HE occurrence, respectively. The median time to HE development was significantly different across the three groups: 65.00 months (95% CI: 47.97-82.03) for the low-risk group, 50.00 months (95% CI: 0.00-110.05) for the intermediate-risk group, and 1.00 months (95% CI: 0.00-7.20) for the high-risk group (χ2=22.02, P< 0.001). However, the median overall survival of the three groups was not significantly different. Multivariate Cox regression identified APTT-CCI score (HR=2.25, 95% CI: 1.32-3.83, P=0.003), preoperative HE (HR=3.25, 95% CI: 1.10-9.63, P=0.03), and active bleeding history (HR=0.25, 95% CI: 0.09-0.68, P=0.006) as independent predictors of post-TIPS HE. Independent risk factors for post-TIPS survival included GGT (HR=1.00, 95% CI: 1.00-1.01, P< 0.001), ALB (HR=0.94, 95% CI: 0.89-1.00, P=0.032), and Na (HR=0.89, 95% CI: 0.83-0.95, P=0.001).
Conclusions: The APTT-CCI score can serve as a promising predictor for HE development in cirrhotic patients with portal hypertension undergoing TIPS.
Keywords: Activated partial thromboplastin time; Charlson comorbidity index; Transjugular intrahepatic portosystemic shunt; Hepatic encephalopathy; Portal hypertension.
Citation: Zhu L, Huang Q, Zhao Z, Ji J, Zheng L, et al. Activated partial thromboplastin time-charlson comorbidity index score as a predictor of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. J Gastroenterol Res Pract. 2026; 6(3): 1250.
Introduction
Liver cirrhosis is the advanced stage of chronic liver disease and poses a significant global health burden. Between 2009 and 2019, the global population of cirrhosis rose from 1.378 billion to 1.691 billion cases [1]. In China, the incidence of chronic liver diseases experienced a sharp increase over the same period, growing from 6.83 million to 11.87 million cases [2]. Portal hy pertension (PHT) is a common complication of liver cirrhosis, characterized by increased pressure within the portal venous system. It can lead to serious clinical consequences, including esophageal and gastric variceal bleeding, ascites, hepatic en cephalopathy, and hepatorenal syndrome. These complications pose significant threats to the patient’s life and can drastically impact their prognosis [3,4]. Transjugular Intrahepatic Portosys temic Shunt (TIPS) is an effective approach to reduce the pres sure in the portal venous system by creating a conduit between the hepatic veins and the portal vein [5], which can effectively mitigate the risk of variceal bleeding and ascites-related symp toms [6]. However, 30%-55% of individuals develop Hepatic Encephalopathy (HE) within one year post-TIPS [7], which is strongly linked to poor health-related quality of life, frequent hospitalizations, and an increased mortality rate [8,9]. There fore, a careful evaluation of the patients before TIPS insertion is crucial.
Various risk factors have been identified, including advanced age, Child-Pugh score, Model for End-Stage Liver Disease (MELD) score, body mass index, controlling nutritional status score, and a history of previous HE [10-13]. However, despite these advances, limitations remain. Many existing studies fail to comprehensively account for the influence of chronic comor bidities, such as diabetes, cardiovascular diseases, and renal impairment. It has been reported that the incidence of HE is as sociated with various extrahepatic chronic diseases such as dia betes, chronic kidney disease, and cardiovascular disease [14 18]. Chronic kidney disease contributes to the accumulation of toxic substances due to impaired renal excretion, disrupting liv er detoxification processes [18]. Similarly, diabetes exacerbates ammonia metabolism disorders through mechanisms such as increased intestinal glutaminase K activity and enhanced mus cle protein breakdown, leading to hyperammonemia [14]. Thus, it is necessary to comprehensively assess the impact of chronic comorbidities on the development of HE.The Charlson Comor bidity Index (CCI) incorporates information on various chronic diseases, providing a comprehensive measure of a patient’s overall health burden. As a validated tool, CCI is widely used to assess the impact of comorbid conditions on clinical outcomes. Previous studies have identified CCI as an independent risk fac tor for both the prognosis of TIPS and mortality in patients with liver cirrhosis [19,20]. Thus, integrating CCI into predictive mod els could potentially enhance their accuracy and clinical utility.
In addition to chronic disease burden, coagulation disorders are also recognized as poor prognostic factors in chronic liver disease, often resulting from liver failure. Advanced liver cirrho sis is associated with reduced synthesis of coagulation factors, abnormal platelet count and function, and imbalances in the fibrinolytic system, all of which contribute to a higher risk of complications and poorer outcomes [21]. Supporting this, Tan et al. [22] demonstrated a dose-response relationship between the international normalized ratio (INR) and the occurrence of HE in liver cirrhosis, highlighting the predictive value of coagula tion parameters for HE. Similarly, Kakisaka et al. [23] identified INR and Prothrombin Time (PT) as risk factors for HE, further emphasizing the link between coagulation abnormalities and HE development. Additionally, Rui et al. [24] reported that PT and Activated Partial Thromboplastin Time (APTT) are indepen dent predictors of mortality in acute-on-chronic liver failure, underscoring their prognostic relevance in liver-related compli cations. Given these findings, integrating coagulation dysfunc tion markers such as INR, PT, and APTT into the evaluation of TIPS patients might enhance the prediction of HE occurrence, offering a more comprehensive approach to risk stratification.
Considering the potential advantages of CCI and APTT in pre dicting the risk of HE, a novel scoring system was developed. Specifically, the Youden index for APTT and CCI was calculated for each patient to determine optimal cutoff values. Based on the binary classification of APTT and CCI, patients were catego rized into three groups: Low-Risk (Low APTT + Low CCI), Inter mediate-Risk (High APTT + Low CCI or Low APTT + High CCI), and High-Risk (High APTT + High CCI). The Area Under the Curve (AUC) of the APTT-CCI score was analyzed, and independent risk factors for the time to develop HE post-TIPS were identified. For individual prediction, a nomogram was constructed, and its re liability will be validated. By integrating CCI with coagulation parameters, this approach comprehensively accounts for both the systemic burden of chronic comorbidities and the localized effects of liver dysfunction, offering a tool for risk stratification and individualized prevention strategies.
Materials and methods
Patients
This study was approved by the Institutional Review Board of Lishui Central Hospital in accordance with the Declaration of Helsinki (Approval No: 2023-746).The database was accessed following the approval on December 7, 2023.The need for pa tient’s informed consent was waived,and all methods were car ried out in accordance with relevant guidelines and regulations. 86 cirrhotic patients with PHT who underwent TIPS at Lishui Central Hospital between 01/01/2016 and 01/06/2024 were in cluded. The inclusion criteria were as follows: ① Patients with cirrhosis who had been diagnosed with PHT and had a history of esophagogastric variceal rupture bleeding and refractory as cites; The exclusion criteria were as follows: ① Having received liver transplantation; ② Patients lacking laboratory data be fore TIPS and lost to follow-up; ③ Patients under the age of 18 or over the age of 85. The flowchart was shown in Figure 1. ④ Given that a history of previous HE episodes might compro mise the independence of postoperative HE risk assessment, this study did not classify it as an exclusion criterion. Instead, preoperative HE (Pre-HE) history was included in the baseline data and as a variable in the multivariate analysis (Table 1 and 2), with its potential confounding effects controlled through sta tistical methods.
Data collection
In this study, general information and clinical characteristics were retrospectively collected, including age, gender, etiol ogy of cirrhosis, history of Pre-HE, history of active bleeding, ascites status, MELD score, and Child-Pugh grade. Laboratory examination results encompassed red blood cell count (RBC, ×1012/L), White Blood Cell count (WBC, ×109/L), neutrophil count (×109/L), lymphocyte count (×109/L), Platelet Count (PLT, ×109/L), serum hemoglobin level (g/L), albumin level (g/L), cre atinine level (μmol/L), Alanine Aminotransferase (ALT, U/L), As partate Aminotransferase (AST, U/L), Alkaline Phosphatase (ALP, U/L), Gamma-Glutamyltransferase (GGT, U/L), and Total Biliru bin (TBIL, μmol/L). Additionally, coagulation function indicators included International Normalized Ratio (INR), APTT (s), and PT (s) , were also collected. Notably, the diagnosis of preoperative and postoperative HE was determined based on the West Haven Criteria [25]. In this study, patients were graded for HE before surgery and at each postoperative follow-up visit in accordance with the West Haven criteria. All assessments were indepen dently conducted by 2 internally trained physicians, covering core indicators such as consciousness status, cognitive function, and behavioral performance. In cases of discrepancies between the two physicians’ evaluation results, a final diagnosis was reached through joint review of the patients’ clinical data. The time to HE onset was defined as the interval from the date of TIPS to the development of HE. Overt Hepatic Encephalopathy (OHE) is characterized by distinct mental abnormalities (such as changes in personality and behavior) or altered consciousness and coma,which corresponds to grades 2 to 4 in the West Haven scale. Overall Survival (OS) was defined as the duration from the date of TIPS to death.
Transjugular intrahepatic portosystemic shunt
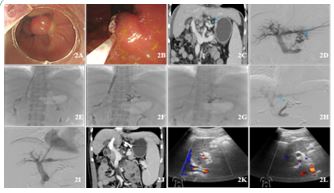
TIPS was performed by interventional physicians with more than 10 years of professional experience. Before the TIPS proce dure, all patients underwent necessary imaging examinations, including abdominal enhanced CT or liver enhanced MRI, to as sess the liver condition, portal vein system, and other relevant anatomical structures. These imaging data helped to guide the TIPS procedure and ensure optimal planning and accurate po sitioning of the catheter and stent. The specific operations of TIPS surgeries were as follows: (1) Under full ECG monitoring, the puncture points of the right internal jugular vein and right inguinal artery were localized by ultrasound, disinfected locally, and anesthetized with 2% lidocaine, followed by the Seldinger puncture technique. After successful puncture, a 5F catheter sheath was introduced. (2) Hepatic arteriography and indirect portal vein angiography were performed first to understand the location and patency of the portal vein. (3) The guide wire was introduced through the right jugular vein catheter, followed by the introduction of the RUPS-100 puncture sheath, which was sent to the right hepatic vein. Under fluoroscopy, the sheath was punctured into the portal vein branch, the guide wire and catheter were further introduced, and portal venous pressure was measured. (4) A dedicated 8 mm × 5-8 cm stent-graft (GORE®VIATORR®TIPS) was selected to establish a hepatic vein portal vein shunt. In some patients, a combined stent technique using an 8 mm × 5 cm covered stent and an 8 mm × 6 cm uncov ered stent was utilized. Finally, a 6-8 mm balloon catheter was introduced to dilate the stent. (5) The portal venous pressure was measured again, and the portal venous pressure gradient was calculated, the TIPS procedure was shown in Figure 2.
Construction of the APTT-CCI score and grouping method
The modeling method used in this study is based on the sen sitivity and specificity derived from the ROC curve. The Youden index is calculated using the formula: Youden Index = Sensitivity + Specificity - 1. The diagnostic cut-off value corresponding to the maximum value of the Youden index is considered the op timal diagnostic cut-off. Based on these cut-off values, patients were classified into the following groups: high APTT and low APTT, or high CCI and low CCI. Specifically, a binary classification system was then used to assign an APTT-CCI score. The APTTCCI score ranges from 0 to 2 as follows: 2 points: High APTT and high CCI; 1 point: High APTT and Low CCI or Low APTT and High CCI,0 points: either low APTT or low CCI. Lastly, all patients were categorized into three groups: Low-Risk (Low APTT + Low CCI), Intermediate-Risk (High APTT + Low CCI or Low APTT + High CCI), and High-Risk (High APTT + High CCI).
Statistical analysis
All statistical analyses were performed using SPSS (IBM SPSS Statistics, Version 26.0) and R (version 4.3.1). Continuous vari ables are presented as the mean±SD, and categorical variables as counts and frequencies. For continuous data, the one-way ANOVA and Kruskal-Wallis test were used, while categorical data were analyzed with the χ2 test. The optimal cutoff values for clinical indicators were determined by the Youden index. The predictive performance of non-invasive indicators was eval uated using the area under the Receiver Operating Characteris tic (ROC) curve. Independent risk factors for time to HE devel opment and OS were estimated using Cox proportional hazards regression. OS curves and the cumulative incidence of HE curves were estimated with the Kaplan-Meier method, and differences were compared using the log-rank test. A nomogram prediction model was established by integrating the independent risk fac tors for time to HE development and survival. Its accuracy was further validated using a calibration chart with 1000 bootstrap samples. The clinical utility of the nomogram was measured by decision curve analysis (DCA), which calculates the net benefit at different threshold probabilities.
Results
Optimal cutoff values for APTT-CCI score
The Youden index for APTT and CCI was 0.23 and 0.30, re spectively. ROC analysis determined the optimal cutoff values for APTT and CCI to be 42.35 and 5.50, respectively. The sen sitivity and specificity of APTT for predicting HE were 0.36 and 0.87, while the sensitivity and specificity of the CCI score were 0.54 and 0.77, respectively. According to the cutoff values of APTT and CCI, an APTT-CCI score was calculated for each pa tient. Among the 86 cirrhotic patients, 44 cases (51.2%) were assigned an APTT-CCI score of 0, 32 cases (37.2%) a score of 1, and 10 cases (11.6%) a score of 2. The low-risk group was defined by APTT <42.35 and CCI <5.50; APTT-CCI score=0. The intermediate-risk group was defined by APTT ≥42.35 and CCI <5.50, or APTT <42.35 and CCI ≥5.50; APTT-CCI score=1. The high-risk group was defined by APTT ≥42.35 and CCI ≥5.50; APTT-CCI score = 2.
Clinical features of cirrhotic patients with PHT who underwent TIPS
The mean age of the 86 cirrhotic patients included in this study was 55.74±10.74 years. Among the participants, 16(18.6%) were female, and 70(81.4%) were male. Of these patients, 53 cases (61.6%) had cirrhosis caused by viral hepatitis, while the remaining 33 cases (38.4%) had cirrhosis due to other causes, including alcoholic cirrhosis (22.1%), autoimmune liver disease (2.2%), and cryptogenic cirrhosis (14.1%). Additionally, 74.4% of patients presented with ascites, 33.7% had a history of active bleeding, and 12.8% experienced Pre-HE before TIPS. There were no significant differences in age, gender, etiology of cirrhosis, history of active bleeding, ascites status, MELD score, RBC count, WBC count, neutrophil count, lymphocyte count, platelet count, hemoglobin level, albumin level, creatinine level, ALP, GGT, AST, ALT, INR (all P>0.05). However, notable inter group differences emerged across key clinical and biochemical indicators. Biochemical analyses revealed statistically significant variations in TBIL and PT levels among the three risk groups, with the highest values consistently documented in the high-risk cohort (Table 1), which aligned with impaired hepatic synthetic and excretory function in this group. This trend was mirrored in liver function stratification by Child-Pugh classification: the distribution of severe liver function impairment exhibited a clear risk-associated gradient across groups, with the high-risk group accounting for the largest proportion of Class C cases. Consistent with these markers of hepatic dysfunction, the prevalence of HE-related endpoints also varied significantly by risk stratum. For Pre-HE, the incidence of a prior Pre-HE history rose progressively from the low-risk to the intermediate-risk group, and peaked in the high-risk group. Similarly, with regard to OHE following TIPS, significant differences in OHE incidence were observed across groups, with the high-risk cohort demonstrating the consistently highest frequency of post-TIPS OHE.
APTT-CCI score as a prognostic indicator for HE
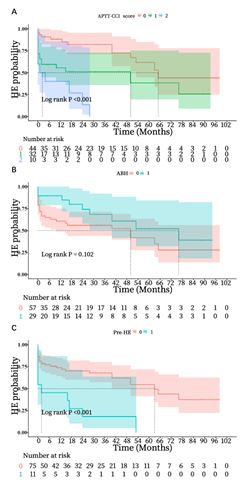
A total of 39 (45.3%) patients had developed HE by the fol low-up date. The median time to HE development was 65.00 months (95% CI: 47.97-82.03) for the low-risk group, and the median time to development of HE was 50.00 months (95% CI: 0.00-110.05) for intermediate-risk group, and the median time to development of HE was 1.00 months (95% CI: 0.00-7.20) for high-risk group (χ2=22.02, P<.001) (Figure 3A). Univariate Cox re gression analysis was conducted to identify parameters associ ated with time to HE development. Significant factors (P<0.05), including active bleeding history, APTT-CCI score, and Pre-HE, were further evaluated using multivariate analysis to determine their impact on time to HE development. Multivariate analysis revealed that active bleeding history (HR=0.25, 95% CI: 0.09 - 0.68, P=0.006), APTT-CCI score (HR=2.25, 95% CI: 1.32-3.83, P=0.003), and Pre-HE (HR=3.25, 95% CI: 1.10 - 9.63, P=0.03) were independent prognostic factors (Table 2). Additionally, the APTT-CCI score was identified as an independent predictor, with APTT-CCI score of 1 (HR=2.08, 95% CI: 0.94-4.63, P=0.072) and APTT-CCI score of 2 (HR=5.27, 95% CI: 1.75-15.84, P=0.003) significantly associated with the time to HE development. The three independent risk factors were incorporated into a nomo gram prediction model (Figure 4A); the C-index was 0.77 (95% CI: 0.69-0.85), and the AUC values for predicting 1-year, 2-year, and 3-year HE occurrence probabilities were 0.79 (95% CI: 0.69 0.90), 0.82 (95% CI: 0.71-0.93), and 0.84 (95% CI: 0.74-0.94), respectively, indicating that the model had good discriminative ability. The calibration curve for predicting the prognosis after TIPS in the prediction model was basically consistent with the observed values (Figures 4B,C & D). The prediction model based on the nomogram can accurately predict the prognosis of pa tients after TIPS, and the high clinical decision-making value of this model is confirmed by the DCA decision curve (Figures 4E,F & G).
OS analysis
A total of 42(48.8%) patients had died by the follow-up date, the median OS in the low-risk, intermediate-risk, and high-risk groups was determined to be 59.00 months (95% CI: 28.13-89.87), 47.00 months (95% CI: 22.43-71.57), and 56.00 months (95% CI: 23.90-88.10). However, the differences among the groups were not statistically significant (χ2=1.35, P=0.509). Univariate Cox regression analysis was conducted to identify parameters associated with OS. Significant factors (P<0.05), including GGT, ALB, and Na, were further evaluated using multivariate analysis to determine their impact on OS. Multi variate analysis revealed that GGT (HR=1.00, 95% CI: 1.00-1.01, P<0.001), ALB (HR=0.94, 95% CI: 0.89-1.00, P=0.032), and Na (HR=0.89, 95% CI: 0.83-0.95, P=0.001) were independent prog nostic factors (Table 3). The three independent risk factors were incorporated into the nomogram prediction model (Figure 5A), the C-index was 0.69 (95% CI: 0.60-0.79), and the Area Under Curve (AUC) values for predicting the 1-year, 2-year, and 3-year survival probabilities were 0.72 (95% CI: 0.58-0.86), 0.69 (95% CI: 0.55-0.83), and 0.72 (95% CI: 0.59-0.85), indicating that the model had good discriminative ability. The calibration curve for predicting the prognosis after TIPS in the prediction model was basically consistent with the observed values (Figures 5B,C & D). The prediction model based on the nomogram can accu rately predict the prognosis of patients after TIPS, and the high clinical decision-making value of this model is confirmed by the DCA decision curve (Figures 5E,F & G).


Table 1: Baseline demographic and clinical characteristics of patients.
| Variables | Total (n=86) | Low-risk Group(n=44) | Intermediate-risk group(n=32) | High-risk group(n=10) | P value |
|---|---|---|---|---|---|
| Age(Years) | 55.74±10.74 | 56.84±9.52 | 54.78±11.84 | 54.00±12.34 | 0.618 |
| Sex(n,%) | 0.423 | ||||
| Male | 70(81.4) | 35(79.5) | 28(87.5) | 7(70.0) | |
| Female | 16(18.6) | 9(20.5) | 4(12.5) | 3(20.0) | |
| Aetiology (n,%) | 0.298 | ||||
| Viral hepatitis | 53(61.6) | 25(56.8) | 23(71.9) | 5(50.0) | |
| Others | 33(38.4) | 19(43.2) | 9(28.1) | 5(50.0) | |
| Pre-HE | 0.041 | ||||
| Yes | 11(12.8) | 2(4.5) | 6(18.8) | 3(30.0) | |
| No | 75(87.2) | 42(95.5) | 26(81.3) | 7(70.0) | |
| Active bleeding history | 0.877 | ||||
| Yes | 29(33.7) | 15(34.1) | 10(31.3) | 4(40.0) | |
| No | 57(66.3) | 29(65.9) | 22(68.8) | 6(60.0) | |
| Ascites(n,%) | 0.053 | ||||
| Yes | 64(74.4) | 28(63.6) | 27(84.4) | 9(90.0) | |
| No | 22(25.6) | 16(36.4) | 5(15.6) | 1(10.0) | |
| OHE | <0.001 | ||||
| Yes | 39(45.3) | 13(29.5) | 17(53.1) | 9(90.0) | |
| No | 47(54.7) | 21(70.5) | 15(46.9) | 1(10.0) | |
| MELD score | 8.36±3.31 | 8.12±3.28 | 8.47±3.71 | 8.90±2.56 | 0.396 |
| Child-Pugh grade | 0.006 | ||||
| grade A | 26(30.2) | 21(47.7) | 4(12.5) | 1(10.0) | |
| grade B | 45(52.3) | 16(36.4) | 24(75.0) | 5(50.0) | |
| grade C | 15(17.4) | 7(15.9) | 4(12.5) | 4(40.0) | |
| RBC(×10¹²/L) | 2.97±0.67 | 2.99±0.67 | 3.03±0.67 | 2.75±0.68 | 0.563 |
| WBC(×10⁹/L) | 5.13±4.26 | 5.40±4.87 | 4.38±2.14 | 7.30±5.68 | 0.218 |
| Neutrophil(×10⁹/L) | 3.71±3.89 | 4.02±4.59 | 2.79±1.63 | 5.36±5.19 | 0.262 |
| Lymphocyte(×10⁹/L) | 0.88±0.67 | 0.86±0.58 | 0.76±0.57 | 1.32±1.08 | 0.434 |
| Platelet(×10⁹/L) | 78.20±45.44 | 86.11±48.95 | 68.16±41.32 | 75.50±38.34 | 0.179 |
| Hemoglobin(g/L) | 87.19±22.41 | 87.00±24.16 | 87.44±19.15 | 87.30±26.26 | 0.997 |
| Albumin(g/L) | 30.61±5.30 | 31.61±5.73 | 29.58±4.41 | 29.08±4.86 | 0.167 |
| Creatinine(μmol/L) | 83.88±68.61 | 89.84±85.18 | 78.00±45.88 | 76.50±46.79 | 0.427 |
| ALT(U/L) | 53.74±146.42 | 33.05±42.68 | 53.91±174.78 | 144.30±278.11 | 0.572 |
| AST(U/L) | 65.99±141.32 | 46.18±64.28 | 50.88±93.36 | 158.50±266.17 | 0.325 |
| ALP(U/L) | 110.97±66.01 | 105.70±71.02 | 112.84±44.91 | 128.90±98.60 | 0.178 |
| GGT(U/L) | 81.97±164.90 | 69.16±100.10 | 97.09±240.25 | 94.30±65.10 | 0.193 |
| TBIL(μmol/L) | 27.22±17.52 | 24.92±16.99 | 26.66±17.79 | 38.97±14.62 | 0.010 |
| INR | 1.42±0.32 | 1.39±0.36 | 1.40±0.28 | 1.59±0.26 | 0.100 |
| PT(s) | 15.98±3.72 | 15.37±3.84 | 16.05±3.12 | 18.53±4.21 | 0.036 |
Abbreviations: Pre-HE: Preoperative hepatic encephalopathy; MELD: Model for End-Stage Liver Disease; RBC: Red Blood Cell; WBC: White Blood Cell; ALT: Alanine Aminotransferase; AST: Aspartate Aminotransferase; ALP: Alkaline Phosphatase; GGT: Gamma-Glutamyltransferase; TBIL: Total Bilirubin; INR: International Normalized Ratio; PT: Prothrombin Time.
Table 2: Factors associated with risk of HE after Transjugular intrahepatic portosystemic shunt.
| Variables | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR(95% CI) | P value | HR(95% CI) | P value | |
| Age | 1.00(0.97 - 1.04) | 0.803 | ||
| Sex | 0.71(0.28 - 1.81) | 0.466 | ||
| Alcohol | 1.71(0.90 - 3.26) | 0.104 | 1.13(0.49 - 2.65) | 0.77 |
| Viral hepatitis | 0.88(0.46 - 1.69) | 0.706 | ||
| Active bleeding history | 0.56(0.27 - 1.16) | 0.120 | 0.25(0.09 - 0.68) | 0.006 |
| Ascites | 2.44(1.06 - 5.64) | 0.037 | 2.20(0.87 - 5.61) | 0.10 |
| RBC | 0.72(0.44 - 1.17) | 0.186 | 0.86(0.47 - 1.60) | 0.64 |
| AST | 1.00(1.00 - 1.00) | 0.139 | 1.00(1.00 - 1.00) | 0.43 |
| TBIL | 1.01(0.99 - 1.03) | 0.195 | 1.00(0.98 - 1.03) | 0.81 |
| ALP | 1.00(1.00 - 1.00) | 0.063 | 1.00(1.00 - 1.01) | 0.67 |
| GGT | 1.00(1.00 - 1.00) | 0.009 | 1.00(1.00 - 1.00) | 0.11 |
| Na | 0.91(0.85 - 0.98) | 0.010 | 0.95(0.88 - 1.03) | 0.23 |
| MELD score | 1.04(0.97 - 1.11) | 0.270 | ||
| Creatinine | 1.00(1.00 - 1.01) | 0.252 | ||
| APTT- CCI score | 2.53(1.62 - 3.94) | <0.01 | 2.25(1.32 - 3.83) | 0.003 |
| INR | 0.87(0.30 - 2.55) | 0.802 | ||
| Pre-HE | 3.46(1.66 - 7.23) | 0.036 | 3.25(1.10 - 9.63) | 0.03 |
| Child-Pugh grade | 1.27(0.79 - 2.05) | 0.321 | ||
| Neutrophil | 0.99(0.92 - 1.08) | 0.893 | ||
| Lymphocyte | 0.87(0.50 - 1.50) | 0.614 | ||
Table 3: Factors associated with risk of overall survival after Transjugular intrahepatic portosystemic shunt.
| Variables | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR(95% CI) | P value | HR(95% CI) | P value | |
| Pre-HE | 1.72(0.72 - 4.11) | 0.224 | ||
| AST | 1.00(1.00 - 1.00) | 0.995 | ||
| ALT | 1.00(1.00 - 1.00) | 0.716 | ||
| GGT | 1.01(1.01 - 1.01) | 0.016 | 1.00(1.00 - 1.01) | <0.001 |
| Platelet | 1.01(1.00 ~ 1.01) | 0.061 | 1.00(1.00 – 1.01) | 0.410 |
| APTT- CCI score | 1.12(0.73 - 1.72) | 0.613 | ||
| Albumin | 0.96(0.90 ~ 1.01) | 0.117 | 0.94(0.89 - 1.00) | 0.032 |
| Na | 0.89(0.83 ~ 0.95) | <0.001 | 0.89(0.83 - 0.95) | 0.001 |
| CR | 1.00(1.00 ~ 1.00) | 0.346 | ||
| INR | 1.32 (0.52 ~ 3.36) | 0.555 | ||
| HGB | 0.99 (0.98 ~ 1.01) | 0.466 | ||
| NLR | 0.97 (0.91 ~ 1.03) | 0.297 | ||
| PLR | 1.00 (1.00 ~ 1.00) | 0.682 | ||
Discussion/Conclusion
In this study, we suggest that an APTT-CCI score is an inde pendent predictive factor for HE development in cirrhotic pa tients with PHT undergoing TIPS. The high-risk group was asso ciated with a significantly poorer prognosis for HE development than the other groups. However, a high APTT-CCI score did not indicate poor OS, although there was a tendency towards short er OS in the intermediate-risk group than in the low-risk group.
Previous studies have confirmed that various scoring sys tems, such as the Child-Pugh score, MELD score, and other pre dictive models, are associated with the occurrence of HE after TIPS in cirrhotic patients with PHT. However, these models have certain limitations that affect their prognostic value [11,26]. For example, the Child-Pugh score, which evaluates liver function based on clinical and biochemical parameters, has been widely used to assess the severity of liver disease. However, its ability to predict the development of HE after TIPS was limited because it does not fully account for dynamic changes in liver function or the impact of portal pressure changes post-TIPS. Furthermore, its subjective nature in assessing ascites and encephalopathy may have introduced variability [27,28]. While the MELD score has been widely used for predicting mortality in patients with cirrhosis, its prognostic effectiveness in predicting HE after TIPS is controversial. The MELD score may be less accurate in pa tients with lower MELD score [29]. This has been shown to re duce its predictive value in determining the risk of HE, especial ly in those with compensated cirrhosis or lower baseline score. The MELD score primarily focuses on liver function parameters (bilirubin, creatinine, INR) but does not incorporate inflamma tory markers or other factors that might influence the risk of HE post-TIPS [30]. Furthermore, a study by Liao et al. [10] proposed a novel nomogram for predicting OHE after TIPS in patients with PHT. While this model showed promise, it may be limited by its reliance on specific markers that may not be universally avail able in clinical practice. Thus, accurately identifying patients at risk of developing HE after TIPS remains a challenge.
In this retrospective study, we identified that the APTT-CCI score was an independent risk factor for the occurrence of HE in patients with PHT after TIPS. Consistent with previous findings, APTT, as a coagulation function indicator, has been reported to impact the prognosis of patients after TIPS [31]. For a more comprehensive prediction of HE development in cirrhotic pa tients with PHT undergoing TIPS, we incorporated APTT with the CCI, an indicator of comorbidities. Previous studies have indicated that the CCI was an independent risk factor for prog nosis following TIPS [19], supporting the idea that comorbidi ties may enhance the predictive accuracy of the APTT-CCI score for HE. In this study, the median time to HE development was 65.00 months (95% CI: 47.97–82.03) in the low-risk group, 50.00 months (95% CI: 0.00–110.05) in the intermediate-risk group, and 1.00 months (95% CI: 0.00–7.20) in the high-risk group (χ²=22.02, P<0.001). These results predict a shorter dura tion until HE onset and a worse prognosis in patients with a high APTT-CCI score.
In addition, our findings also suggested that a history of HE before TIPS is a predictor of postoperative HE. A history of Pre-HE indicates that the patient’s liver function and systemic condition were in a relatively poor state: the liver’s ability to metabolize and detoxify neurotoxins had decreased, and fac tors such as intestinal flora disturbance may have already ex isted, which in turn increased the likelihood of postoperative HE [13,32-34]. The history of active bleeding is an independent risk factor for the occurrence of HE after TIPS in patients, which is consistent with previous studies [35,36]. The possible reasons were that preoperative active bleeding caused intestinal hem orrhage, where intestinal bacteria break down blood proteins and produced large amounts of ammonia. This ammonia was absorbed into the bloodstream, increasing the liver’s detoxifi cation burden and potentially leading to hepatic encephalopa thy. For personalized evaluation, a nomogram was established by incorporating active bleeding history, APTT- CCI score, and Pre-HE. The C-index, calibration curves, and DCA confirmed that the model had good predictive performance, indicating that the predictive model based on the APTT-CCI score could be used to evaluate the risk of post-TIPS HE in cirrhotic patients with PHT.
The APTT-CCI score, as a reliable predictive tool for post-TIPS HE, demonstrates clear clinical applicability in informing deci sion-making. Firstly, regarding TIPS surgical decision-making: the high-risk group demonstrated a median HE onset time of only 1.00 months, indicating an extremely high short-term HE risk. For such patients, TIPS should not be arbitrarily excluded as a treatment option, but a more rigorous multidisciplinary evaluation was required. Secondly, existing evidence has con firmed that rifaximin combined with lactulose can effectively reduce the recurrence of post-TIPS HE by inhibiting intestinal ammonia-producing bacteria [37]. Given the high risk of HE in the APTT-CCI high-risk group, preoperative initiation or imme diate postoperative administration of rifaximin prophylaxis was recommended to mitigate the risk of early HE onset. For inter mediate-risk patients, prophylactic use could be individualized based on additional risk factors such as a history of Pre-HE or active bleeding. Low-risk patients may only require close moni toring without routine prophylaxis. Thirdly, the APTT-CCI score could serve as a supplementary screening tool to optimize the patient cohort. Integrating it with traditional indicators such as Child-Pugh grade and MELD score helped identify patients who may have benefited more from TIPS while avoiding unneces sary surgical risks in those with excessively high HE susceptibil ity. For example, patients with both a high APTT-CCI score and Child-Pugh grade C may have needed to be prioritized for liver transplantation evaluation rather than TIPS, as the combined risks of HE and poor liver function may outweigh the therapeutic benefits.
Since the APTT-CCI score showed efficacy in predicting HE, we further evaluated its efficacy in predicting OS. However, the results showed that the APTT-CCI score did not effectively predict OS. This finding reflects the fact that factors contribut ing to a higher risk of postoperative HE may not necessarily be the key determinants of OS. The APTT and CCI scores primar ily focus on coagulation and comorbidities, but they do not encompass all potential factors that could influence patients’ survival [38,39]. Consequently, a higher APTT-CCI score did not consistently correlate with a shorter survival time. In addition, a higher incidence of HE did not consistently correlate with a shorter survival time [40]. Therefore, our results suggest that while the APTT-CCI score is a useful predictor for the develop ment of HE, it is not an effective predictor of OS in these pa tients. To further identify independent risk factors for OS in this cohort, we performed univariate and multivariate analyses and found that GGT, albumin, and Na were independent risk factors for the prognosis of patients with PHT after TIPS.
As a key enzyme involved in the glutamyl cycle, elevated se rum levels of GGT have traditionally been regarded as a hall mark indicator of hepatobiliary system injury, cholestasis, or alcoholic liver injury. Preoperative GGT levels have been consid ered to be related to the survival of patients after TIPS. Elevated GGT levels often indicate impaired liver function, which could negatively impact the prognosis following the procedure [41]. Extensive damage to hepatocytes in patients with liver cirrhosis led to a decline in synthetic function. A low albumin level was essentially a marker of insufficient hepatic reserve function. TIPS only alleviated PHT but could not reverse the underlying liver lesions. Patients with low albumin had weaker postopera tive hepatic metabolism, detoxification, and repair capabilities, making them more prone to progression to liver failure, which directly affected survival [42]. Hyponatremia in cirrhotic pa tients was associated with sodium and water retention caused by the liver’s impaired ability to inactivate antidiuretic hor mone, as well as intestinal malabsorption induced by PHT. This electrolyte disturbance could further damage hepatocyte func tion, exacerbate abnormal ammonia metabolism, and may also trigger prerenal injury. Due to the imbalance of intravascular os motic pressure, patients with hyponatremia were more prone to complications such as refractory ascites and infections after TIPS, increasing the risk of poor prognosis [43]. A nomogram for overall survival based on these independent factors showed a high C-index, and the calibration curve was highly consistent with the observed values. DCA indicated that our nomogram could be applied to guide clinical practice.
This study had limitations: the single-center design and small sample size may have limited generalizability; external valida tion was needed. Unknown confounders (e.g., gut microbiota) were not assessed. Additionally, while TIPS has been increasing ly used in pediatric populations for cirrhotic and non-cirrhotic indications, our study focused on adults. As noted by Di Giorgio et al. [44], dedicated prognostic tools were needed for pediatric TIPS patients, highlighting the need for future research in this area.
In summary, we investigated the prognostic value of the APTT-CCI score in predicting the development of post-TIPS HE in cirrhotic patients with PHT. Our results demonstrated that the APTT-CCI score, along with a history of preoperative active bleeding and pre-existing HE, was an independent risk factor for the development of post-TIPS HE. Specifically, the APTT-CCI score effectively predicted the time to HE development, offering a potential tool for early identification of patients at risk of this complication. However, while the APTT-CCI score was a use ful predictor for HE, it was not associated with predicting OS in this cohort. This finding suggests that although the occurrence of HE post-TIPS may be a critical factor in patient management, it does not necessarily correlate with a poor prognosis in terms of OS. Collectively, the APTT-CCI score showed promise as a pre dictor for the development of post-TIPS HE in cirrhotic patients with PHT, and further studies with larger, multicenter cohorts and external validation were needed to confirm its clinical util ity and explore its potential role in guiding treatment strategies for these patients.
Declarations
Competing interests statement: The authors have no relevant financial or non-financial interests to disclose.
Ethics approval: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of The Fifth Affiliated Hospital of Wenzhou Medical University (Approval No: 2023-746).
Funding: This work was supported by the Key R&D Program of Lishui City (2021ZDYF12, 2022ZDYF20) National Natural Science Foundation of China (82272090).
Acknowledgments: We thank all patients involved in this study.
Author contributions: All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Chaoming Huang, Qi Huang, Zijian Zhu, Lingyi Zhu, Liyun Zheng, Zhongwei Zhao, Jiansong Ji. The first draft of the manuscript was written by Chaoming Huang, Lingyi Zhu, Shiji Fang, and Liyun Zheng and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Data Availability: The data are available from the corresponding author on reasonable request.
References
- Lan Y, Wang H, Weng H, Xu X, Yu X, Tu H, et al. The burden of liver cirrhosis and underlying etiologies: results from the Global Burden of Disease Study 2019. Hepatol Commun. 2023; 7: e0026.
- Li M, Wang ZQ, Zhang L, Zheng H, Liu DW, Zhou MG. Burden of cirrhosis and other chronic liver diseases caused by specific etiologies in China, 1990-2016: findings from the Global Burden of Disease Study 2016. Biomed Environ Sci. 2020; 33: 1-10.
- Kaji K, Yoshiji H. Can portal hypertension and hepatic decompensation be predicted? J Gastroenterol. 2020; 55: 662-663.
- Simonetto DA, Liu M, Kamath PS. Portal hypertension and related complications: diagnosis and management. Mayo Clin Proc. 2019; 94: 714-726.
- Vizzutti F, Schepis F, Arena U, Fanelli F, Gitto S, Aspite S, et al. Transjugular intrahepatic portosystemic shunt (TIPS): current indications and strategies to improve the outcomes. Intern Emerg Med. 2020; 15: 37-48.
- Wang HL, Lu WJ, Zhang YL, Nie CH, Zhou TY, Zhou GH, et al. Comparison of transjugular intrahepatic portosystemic shunt in the treatment of cirrhosis with or without portal vein thrombosis: a retrospective study. Front Med (Lausanne). 2021; 8: 737984.
- Cheng S, Hu G, Jin Z, Wang Z, Xue H. Prediction of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt based on CT radiomic features of visceral adipose tissue. Acad Radiol. 2024; 31: 1849-1861.
- Moscucci F, Nardelli S, Pentassuglio I, Pasquale C, Ridola L, Merli M, et al. Previous overt hepatic encephalopathy rather than minimal hepatic encephalopathy impairs health-related quality of life in cirrhotic patients. Liver Int. 2011; 31: 1505-1510.
- Labenz C, Baron JS, Toenges G, Schattenberg JM, Nagel M, Sprinzl MF, et al. Prospective evaluation of the impact of covert hepatic encephalopathy on quality of life and sleep in cirrhotic patients. Aliment Pharmacol Ther. 2018; 48: 313-321.
- Liao Y, Zhang L, Wang JT, Yue ZD, Fan ZH, Wu YF, et al. A novel nomogram predicting overt hepatic encephalopathy after transjugular intrahepatic portosystemic shunt in portal hypertension patients. Sci Rep. 2023; 13: 15244.
- Wang Z, Wu YF, Yue ZD, Zhao HW, Wang L, Fan ZH, et al. Comparative study of indocyanine green-R15, Child-Pugh score, and model for end-stage liver disease score for prediction of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. World J Gastroenterol. 2021; 27: 416-427.
- Gu L, Yin X, Cheng Y, Wang X, Zhang M, Zou X, et al. Overweight/obesity increases the risk of overt hepatic encephalopathy after transjugular intrahepatic portosystemic shunt in cirrhotic patients. J Pers Med. 2023; 13: 1-10.
- Li J, Feng D, Pang N, Zhao C, Gao L, Liu S, et al. Controlling nutritional status score as a new indicator of overt hepatic encephalopathy in cirrhotic patients following transjugular intrahepatic portosystemic shunt. Clin Nutr. 2022; 41: 560-566.
- Labenz C, Nagel M, Kremer WM, Hilscher M, Schilling CA, Toenges G, et al. Association between diabetes mellitus and hepatic encephalopathy in patients with cirrhosis. Aliment Pharmacol Ther. 2020; 52: 527-536.
- Gairing SJ, Schleicher EM, Labenz C. Diabetes mellitus: risk factor and potential future target for hepatic encephalopathy in patients with liver cirrhosis? Metab Brain Dis. 2023; 38: 1691-1700.
- Akhtar AJ, Alamy ME, Yoshikawa TT. Extrahepatic conditions and hepatic encephalopathy in elderly patients. Am J Med Sci. 2002; 324: 1-4.
- Bengmark S. Bio-ecological control of chronic liver disease and encephalopathy. Metab Brain Dis. 2009; 24: 223-236.
- Hung TH, Tseng CW, Tseng KC, Hsieh YH, Tsai CC, Tsai CC. Effect of renal function impairment on the mortality of cirrhotic patients with hepatic encephalopathy: a population-based 3-year follow-up study. Medicine (Baltimore). 2014; 93: e79.
- Ronald J, Rao R, Choi SS, Kappus M, Martin JG, Sag AA, et al. No increased mortality after TIPS compared with serial large volume paracenteses in patients with higher model for end-stage liver disease score and refractory ascites. Cardiovasc Intervent Radiol. 2019; 42: 720-728.
- Coppel S, Mathur K, Ekser B, Patidar KR, Orman E, Desai AP, et al. Extra-hepatic comorbidity burden significantly increases 90-day mortality in patients with cirrhosis and high model for end-stage liver disease. BMC Gastroenterol. 2020; 20: 302.
- Tripodi A. Liver disease and hemostatic (dys)function. Semin Thromb Hemost. 2015; 41: 462-467.
- Tan J, He Y, Li Z, Zhang Q, Yang Y, Xu Q, et al. Analysis of the dose-response relationship between the international normalized ratio and hepatic encephalopathy in patients with liver cirrhosis using restricted cubic spline functions. Front Public Health. 2022; 10: 919549.
- Kakisaka K, Kataoka K, Suzuki Y, Kuroda H, Takikawa Y. Appropriate timing to start and optimal response evaluation of high-dose corticosteroid therapy for patients with acute liver failure. J Gastroenterol. 2017; 52: 977-985.
- Rui F, Yang H, Guo Z, Ge Z, Hu X, Zhang L, et al. Derivation and validation of prognostic models for predicting survival outcomes in acute-on-chronic liver failure patients. J Viral Hepat. 2021; 28: 1719-1728.
- American Association for the Study of Liver Diseases, European Association for the Study of the Liver. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline. J Hepatol. 2014; 61: 642-659.
- Kumar S, Shah S, Singh B, Pradhan A. Comparison between creatinine-modified Pugh score and Child-Pugh score for prognostication in decompensated cirrhosis. Cureus. 2024; 16: e62311.
- Wang J, Zhang Z, Yan X, Li M, Xia J, Liu Y, et al. Albumin-bilirubin (ALBI) as an accurate and simple prognostic score for chronic hepatitis B-related liver cirrhosis. Dig Liver Dis. 2019; 51: 1172-1178.
- Toyoda H, Johnson PJ. The ALBI score: from liver function in patients with HCC to a general measure of liver function. JHEP Rep. 2022; 4: 100557.
- Wang Z, Wu YF, Yue ZD, Zhao HW, Wang L, Fan ZH, et al. Comparative study of indocyanine green-R15, Child-Pugh score, and model for end-stage liver disease score for prediction of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. World J Gastroenterol. 2021; 27: 416-427.
- Huang CH, Tseng HJ, Amodio P, Chen YL, Wang SF, Chang SH, et al. Hepatic encephalopathy and spontaneous bacterial peritonitis improve cirrhosis outcome prediction: a modified seven-stage model as a clinical alternative to MELD. J Pers Med. 2020; 10: 186.
- Charlson ME, Carrozzino D, Guidi J, Patierno C. Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom. 2022; 91: 8-35.
- Rowley MW, Choi M, Chen S, Hirsch K, Seetharam AB. Refractory hepatic encephalopathy after elective transjugular intrahepatic portosystemic shunt: risk factors and outcomes with revision. Cardiovasc Intervent Radiol. 2018; 41: 1765-1772.
- Seifert LL, Schindler P, Schoster M, Weller JF, Wilms C, Schmidt HH, et al. Recurrence of hepatic encephalopathy after TIPS: effective prophylaxis with combination of lactulose and rifaximin. J Clin Med. 2021; 10: 4763.
- Peter P, Andrej Z, Katarina SP, Manca G, Pavel S. Hepatic encephalopathy after transjugular intrahepatic portosystemic shunt in patients with recurrent variceal hemorrhage. Gastroenterol Res Pract. 2013; 2013: 398172.
- Wen J, Liu Q, Song J, Tong M, Peng L, Liang H. Lactulose is highly potential in prophylaxis of hepatic encephalopathy in patients with cirrhosis and upper gastrointestinal bleeding: results of a controlled randomized trial. Digestion. 2013; 87: 132-138.
- Foster KJ, Lin S, Turck CJ. Current and emerging strategies for treating hepatic encephalopathy. Crit Care Nurs Clin North Am. 2010; 22: 341-350.
- Xu XT, Jiang MJ, Fu YL, Xie F, Li JJ, Meng QH. Incidence and efficacy of strategies for preventing hepatic encephalopathy following transjugular intrahepatic portosystemic shunt: a meta-analysis. World J Hepatol. 2025; 17: 104890.
- Sivapornpan N, Ratana-Amornpin S, Siramolpiwat S. Hemostatic parameters predict 90-day mortality in hospitalized cirrhotic patients with acute decompensation: a prospective cohort study. Blood Coagul Fibrinolysis. 2022; 33: 176-183.
- Jepsen P, Vilstrup H, Andersen PK, Lash TL, Sørensen HT. Comorbidity and survival of Danish cirrhosis patients: a nationwide population-based cohort study. Hepatology. 2008; 48: 214-220.
- Nardelli S, Riggio O, Marra F, Gioia S, Saltini D, Bellafante D, et al. Episodic overt hepatic encephalopathy after transjugular intrahepatic portosystemic shunt does not increase mortality in patients with cirrhosis. J Hepatol. 2024; 80: 596-602.
- Lin L, Huang ZY, Liu K, Tong XC, Zhang ZX, Xue Y. The free triiodothyronine, gamma-glutamyl transpeptidase and spontaneous bacterial peritonitis index: a novel model for predicting 1-year mortality in patients with HBV-related hepatic encephalopathy. Hepat Med. 2024; 16: 1-9.
- Bettinger D, Sturm L, Pfaff L, Hahn F, Kloeckner R, Volkwein L, et al. Refining prediction of survival after TIPS with the novel Freiburg index of post-TIPS survival. J Hepatol. 2021; 74: 1362-1372.
- Tejedor-Tejada J, Fuentes-Valenzuela E, García-Pajares F, Nájera-Muñoz R, Almohalla-Álvarez C, Sánchez-Martín F, et al. Long-term clinical outcome and survival predictors in patients with cirrhosis after 10-mm-covered transjugular intrahepatic portosystemic shunt. Gastroenterol Hepatol. 2021; 44: 620-627.
- Di Giorgio A, Nicastro E, Agazzi R, Colusso M, D’Antiga L. Long-term outcome of transjugular intrahepatic portosystemic shunt in children with portal hypertension. J Pediatr Gastroenterol Nutr. 2020; 70: 615-622.