
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 6
Hepatic encephalopathy survival and readmission rates on lactulose, rifaximin, zinc, and L-carnitine “quad” therapy
Connor Wayman, MD*; Joshua Pagan-Busigo, MD; Elizabeth Peck, BA; Lucie Pham, BS; Paul Gaglio, MD
Department Transplant Hepatology, Rutgers New Jersey Medical School, New Jersey, USA.
*Corresponding Author : Connor Wayman
Department Transplant Hepatology, Rutgers New Jersey
Medical School, New Jersey, USA.
Tel: 858-472-1083;
Email: waymanconnor@gmail.com
Received : Jan 02, 2026
Accepted : Feb 10, 2026
Published : Feb 17, 2026
Archived : www.jjgastro.com
Copyright : © Wayman C (2026).
Abstract
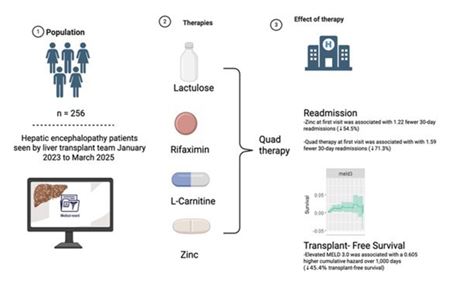
Background: Hepatic Encephalopathy (HE) is a common and often life-threatening complication of acute and chronic liver disease, marked by cognitive dysfunction and high healthcare utilization, including frequent hospitalizations and readmissions. Current treatment strategies for hepatic encephalopathy consist of lactulose and rifaximin, which work to modulate toxins and other encephalopathogenic compounds. Limited data exist regarding the additive effects of zinc and L-carnitine, both of which have shown potential benefits in smaller studies.
Objective: This study aimed to evaluate the impact of these medications—individually and in combination as a quadruple therapy regimen—on hospitalization, readmission, and survival outcomes among patients with HE.
Methods: We conducted a retrospective observational study analyzing patients with documented hepatic encephalopathy seen by the transplant hepatology team. A total of 256 patients met inclusion criteria. Medication exposures were recorded at first clinical contact, receipt ever, and most recent encounter. Patient characteristics and clinical variables including MELD-3.0, West Haven score, transplant status were collected.
Results: Patients who received zinc supplementation on initial visit for hepatic encephalopathy had significantly reduced re hospitalizations (p=0.011). When propensity matched, quadruple therapy recipients (lactulose, rifaximin, zinc, l-carnitine) also had fewer readmissions. (p=0.0013, with mean readmissions 0.64 per 30 days in quadruple therapy recipients vs. 2.23 per 30 days in matched cohort).
Conclusion: Patients who received zinc supplementation experienced decreased rates of re-admissions and trended towards better survival. After propensity matching was done for severity of liver disease, patients with receipt of quadruple therapy had reduced readmission rates.
Keywords: Hepatic encephalopathy; Zinc; Lactulose; Rifaximin; L-carnitine; Survival; Readmission.
Citation: Wayman C, Pagan-Busigo J, Peck E, Pham L, Gaglio P. Hepatic encephalopathy survival and readmission rates on lactulose, rifaximin, zinc and l-carnitine “quad” therapy. J Gastroenterol Res Pract. 2026; 6(2): 1248.
Introduction
Hepatic encephalopathy is a common neuropsychiatric com plication of decompensated liver disease, representing a wide spectrum of cognitive impairments. Patients with hepatic en cephalopathy may experience alterations to their memory, be havior, coordination, and consciousness [1]. The disease is be lieved to be induced by increased exposure to multiple toxins and encephalopathogenic agents which produce an imbalance in glutamine and glutamate causing astrocyte swelling and ce rebral edema [2-4]. Hepatic encephalopathy is associated with significant disease burden, negatively impacting patient func tioning and quality of life. It also has a significant healthcare burden, leading to frequent hospitalizations and readmissions [5,6]. Hepatic encephalopathy has a reported 1-year mortality of 64% and can be a significant predictor of poor prognosis in acute and chronic liver disease [7-9].
Current treatment strategies for hepatic encephalopathy consist of lactulose and rifaximin. Lactulose is a nonabsorbable disaccharide, which acts by reducing the intestinal production/ absorption of ammonia and other toxins by inducing a laxative effect, reducing intraluminal pH, and decreasing ammonia producing bacteria [10]. The use of lactulose is associated with a reduction in the risk of hepatic encephalopathy occurrence or reoccurrence, when compared with placebo or no interven tion. Lactulose is approved for preventing and treating portal systemic encephalopathy [11,12].
Rifaximin is an antibiotic with evidence of benefit on recov ery from HE, prevention of recurrence, and on mortality. Mech anism of action is not completely understood, with evidence of both a direct effect on host ammonia clearance, as well as evidence of preferentially promoting the growth of ammonia clearing microbiota in the gut by helping to remove their com petition [13-16].
While lactulose and rifaximin have been the mainstay of treatment, other approaches have also been investigated. The liver is responsible for zinc metabolism; zinc deficiency is as sociated with poor prognosis in chronic liver disease. Studies have demonstrated that zinc supplementation can improve psychomotor performance and quality of life in patients with liver cirrhosis and minimal hepatic encephalopathy. Zinc sup plementation is also associated with significant improvement in performance on neuro-cognitive testing, including the number connection test, stroop testing, driving simulators and animal naming test. However, it is unclear whether zinc supplementa tion could demonstrate improvement in other clinical areas, such as reduction in HE recurrence [17-20].
There is also evidence for the use of acetyl-L-carnitine in patients with hepatic encephalopathy. Studies have shown L carnitine can reduce blood ammonium levels compared with placebo and decrease loss of muscle mass. Some studies have shown reduction in number of hospital admissions for hepatic encephalopathy, although the long-term impact of this therapy is unknown. There is also mixed evidence on acetyl- L-carnitine’s ability to improve quality of life [21-24].
As such, there is a lack of evidence on the effect of quadru ple therapy (lactulose, rifaximin, zinc, and L-carnitine) in the treatment or prevention of hepatic encephalopathy. Our study is a retrospective, observational study which investigates cor relations between pre- and post-liver transplant patients who had hepatic encephalopathy. We aimed to analyze the effect of these therapies related to which medications reduced overall admission rates and affected survivability.
Methods
This study utilized a retrospective observational study de sign. All transplant hepatology encounters from January 2023 to March 2025 were tabulated, of which 2318 unique medi cal record numbers (mrn) were available and a list generated. These include patients initially seen as early as 2008. This in cludes inpatient hepatology consultation, direct admission to the hepatology primary service, and pre- and post liver trans plant clinic encounters spanning from 2008 to March 2025. Uti lizing problem list and patient diagnosis list, we queried any one with associated “altered mental status,” “encephalopathy,” “confusion” or “hepatic coma.” 283 patient mrn were originally identified using these criteria. They were de-identified into a separate list of mrn associated only with their study ID that was kept apart from the rest of their study data, and their charts were reviewed.
o Of the 283 generated and reviewed, 27 were excluded from analysis with 256 patients remaining (Graph 1).
o 12 patients were excluded due to a clear alternative diagnosis of encephalopathy without any clear evidence of hepatic encephalopathy. Unclear or multifactorial cases in patients with cirrhosis were considered as hepatic encephalopathy.
o 11 post-transplant patients were excluded when it could not be determined if there was a true history of hepatic encephalopathy, largely due to age of data or paucity of available data concerning their pre-transplant course.
o 4 patients were excluded who had encounters generated but we could not determine if they had ever been seen by a hepatology provider.
o 18 additional patients were discovered during chart review who had not been physically seen after January 2023, but instead their last visit was earlier (typically end of 2022). After collecting these data the decision was made to include these 18 patients, in the study analysis.
This occurred because these patients or their representa tives or family members had correspondence with the trans plant clinic, usually medication refills but sometimes questions or updates, and had an eligible encounter falling within the date range that was captured by the search.
Age was not an inclusion or exclusion criteria. Our youngest patient was 23, and oldest was 81 years old. Gaps, incomplete data, and blanks were purposely left in the data when a data point could not be determined.
Data collection procedures:
o EPIC Electronic Medical Record was used to gather data by direct chart review.Demographic data was collected including age, sex, race, ethnicity and etiology of liver disease.
o Clinical data was collected including dates of first contact with the hepatology division, date of first hospitalization for hepatic encephalopathy, whether hospitalized for hepatic encephalopathy and number of readmissions if any, their Model for end stage liver disease 3.0 (Meld 3.0) scores on first contact. Additional data collected included Meld 3.0 on last readmission, Westhaven hepatic encephalopathy scores, presence of documented protein calorie malnutrition, presence of transjugular intrahepatic portosystemic shunt (TIPS), presence of known anatomic porto- systemic shunt, active alcohol use preceding admission, infection present during admission, GI bleeding during admission, transplant status and date of transplant, whether deceased and when if deceased, and lost to follow-up status.
o Presence of documented use of lactulose, rifaximin, zinc or l-carnitine. We evaluated if medication being taken on first contact (first admission or office visit with a Hepatologist) and called this “early,” if present having been taken at all at any point and called this “ever” and if taking on last visit with Hepatology or last visit before transplant if a transplant recipient and called this “late.”
Statistical analysis
o Data was analyzed using R statistical software v4.5.0 and R studio, with associated statistical packages in R as necessary.
o Missing data for vast majority of statistical applications left in place as blank or NA (not available) as appropriate. During the rare instances that data could not be analyzed with NA or blanks present, a mean substitution imputation was utilized.
o To better evaluate quadruple therapy recipients, propensity score matching was used to generate “matched” patients to each quadruple therapy patient and comparisons made. Matched patients were drawn from the pool of non quadruple therapy recipients and were matched based on age, MELD 3.0 score, West Haven score on first contact, presence of protein calorie malnutrition, presence of TIPS and known presence of portosystemic shunt.
Ethics approval
This study was submitted and received IRB approval before initiated - reference is #Pro2024002273 with our institution
Results
Demographic analysis revealed 150 men, 103 women (59% vs. 41%), with 3 not identified. The quadruple therapy group was noted to be 19 women and 17 men (52.8% vs. 47.2%). White, Hispanic/Latino followed by Black patients made up the largest racial and ethnic groups. (n=109 White, 81 Hispanic/La tino, and 28 Black). Quadruple therapy was highest prevalence in Asian patients and lowest in Black patients compared to the overall patient population (4.3% Asian Overall, 8.3% on Quadru ple Therapy, 10.9 % Black Overall, 5.5% on Quadruple Therapy) (Table 1).
249 received lactulose therapy at any point, 243 patients were on lactulose therapy early, 234 receiving this at last visit or before transplant. 225 patients received Rifaximin, 178 patients were on Rifaximin early, 214 on last visit or before transplant. 153 patients received Zinc therapy, 84 patients received Zinc early, 147 received on last visit or before transplant. 38 Patients received L-carnitine therapy, 13 patients received L-carnitine early, 38 on last visit or before transplant (Graph 2). There were 13 patients who received quadruple therapy early, 36 on last visit or before transplant, and 36 patients who received qua druple therapy at any point throughout the study (Graph 2).
Survival data was evaluated using cox regression, Aalen re gression modelling, and Kaplan- Meier curves as appropriate. In terms of medications for overall population, early Lactulose receipt was found to be statistically significant for a positive as sociation with transplant-free survivial and lost-to-follow-up free death events. The large majority of our population received lactulose early (243 out of 256). This may suggest the few who didn’t have lactulose early may have had milder HE not requir ing therapy (Table 2). The survival graphs hint that patients who initiated Zinc early may have improved survival, but this finding did not reach statistical significance (Graph 3).
Demographics and liver risk factors did not seem to influence survival or freedom from HE. Meld 3.0 was the only statistically significant predictor of survival, with higher MELD score associ ated with worse survival (p=0.016) (Table 3). The Aalen graphs do suggest that protein calorie malnutrition demonstrated a more pronounced negative effect on transplant-free and lost to-follow up free survival when analyzing the data over time compared to the other demographics, but was not statistically significant. (up-slope in “proteincal Yes”) (Graph 4).
We then evaluated the effect of quadruple therapy on total hospitalizations using Welch t-testing, with receipt of quadruple therapy associated with a significant increase in total hospital izations, perhaps reflecting that these patients were more de compensated with more severe HE requiring multiple therapies (p=0.0029) (Table 4). Using cox regression, we identified no statistical significance related to each individual medication in terms of receipt ever, however early L-carnitine receipt did have an association with increased total hospitalizations. This pos sibly suggests a similar trend of more severe HE ramping up to tertiary therapies faster, itself being associated with more hos pitalizations. (p=0.0164) (Table 5).
When investigating readmission rates, our linear regres sion model suggested that early zinc receipt was associated with reduced rates of readmissions (p=0.011). Last contact or “late” presence of rifaximin, and late zinc were both indepen dently associated with increased readmission rates (Rifaximin p= 0.046, Zinc p=0.001) (Table 6) which may suggest benefits of supplementing zinc early on in the course.
An analysis of patients who received quadruple therapy re vealed that their mean MELD 3.0 was 21.9, vs. a mean of 20.5 for other patients, with increased death rates; 27.7% or 10 out of total 36 expired compared to 16.3% in the overall study (39 out of 239, 17 unknown). The initial mean HE West Haven score in patients who received quadruple therapy was 2.14, com pared to an overall West Haven score of 1.82 in the remain ing patients. We surmised the recipients of quadruple therapy appeared to be a higher risk group compared to the overall study population. To further assess these trends, we generated a propensity score matched group utilizing what we believed to be high risk factors including Meld 3.0, West Haven Score, Age, Protein-Calorie Malnutrition, presence of TIPS, and known portosystemic shunt. The 36 quadruple therapy recipients were then compared with this generated group of 36 similarly at risk patients in our study (Table 7) (Graph 5). This analysis revealed that there was no statistically significant difference in survival between the matched groups (p=0.25), Kaplan Meier curve shown in (Graph 6).
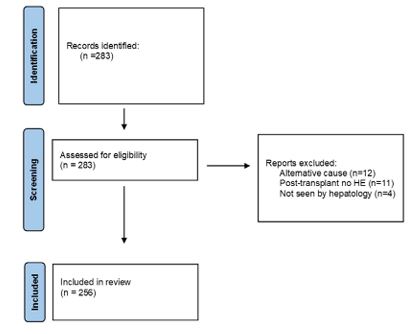
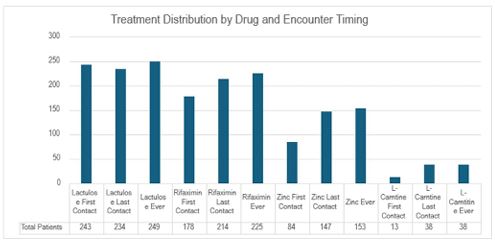
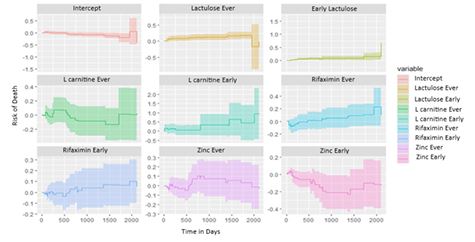
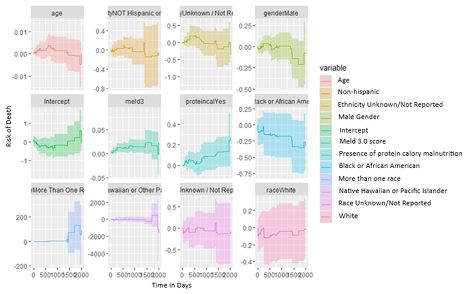
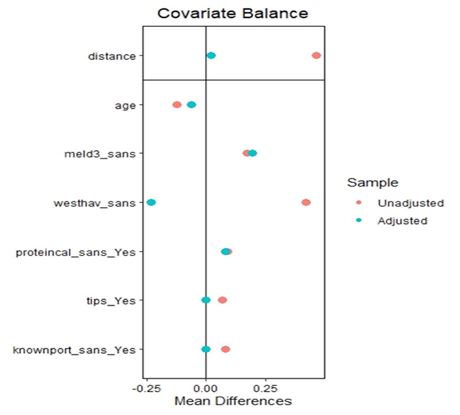
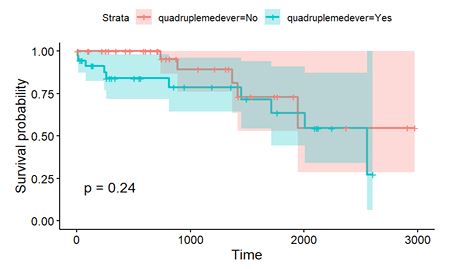
Table 1: Demographics with male predominating overall at 59% vs. 41%. White and then Hispanic/Latino making up the largest racial and ethnic groups.
| Overall study population (N=256) | Patients on quadruple therapy (N=36) | |
|---|---|---|
| Sex | ||
| Male | 150(59.3%) | 17(47.2%) |
| Female | 103(40.7%) | 19(52.8%) |
| Other | 0(0.0%) | 0(0.0%) |
| Prefer not to say | 0(0.0%) | 0(0.0%) |
| Race | ||
| American Indian / Alaska Native | 0(0.0%) | 0(0.0%) |
| Asian | 11(4.3%) | 3(8.3%) |
| Native Hawaiian or Other Pacific Islander | 1(0.4%) | 0(0.0%) |
| Black or African American | 28(10.9%) | 2(5.55%) |
| White | 109(42.6) | 19(52.8%) |
| More Than One Race | 3(1.2%) | 0(0.0%) |
| Unknown / Not Reported | 104(40.6%) | 12(33.3%) |
| Ethnicity | ||
| Hispanic or Latino | 81(31.6%) | 12(33.3%) |
| Not Hispanic or Latino | 157(61.3%) | 24(66.7%) |
| Unknown / Not Reported | 18(7.0%) | 0(0.0%) |
| Age (years) | ||
| Mean | 58.17(±10.93) | 57.03(±10.85) |
Table 2: Quadruple therapy Aalen regression model (N=250*, 35 out of 27 unique events times used).
| Variables | Slope | Coef | SE (Coef) | z | p-value |
|---|---|---|---|---|---|
| Intercept | -1.36x10-4 | -0.001150 | 0.00197 | -0.5840 | 0.55900 |
| At the patient's first visit with the hepatology team or upon discharge after their first hospitalization with Hepatic Encephalopathy: | |||||
| Lactulose | 2.55x10-4 | 0.003120 | 0.00106 | 2.9600 | 0.00309* |
| Rifaximin | 3.56x10-5 | 0.000751 | 0.00250 | 0.3010 | 0.76400 |
| Zinc | -2.92x10-4 | -0.004180 | 0.00277 | -1.5100 | 0.13200 |
| L-carnitine | 7.55x10-4 | 0.016800 | 0.01050 | 1.6000 | 0.11000 |
| At the patient's most recent contact with the hepatology team, or before transplant: | |||||
| Lactulose | 2.61x10-4 | 0.002990 | 0.00331 | 0.9050 | 0.36500 |
| Rifaximin | 5.60x10-5 | 0.001660 | 0.00296 | 0.5600 | 0.57600 |
| Zinc | 6.54x10-5 | 0.000809 | 0.00267 | 0.3030 | 0.76200 |
| L-carnitine | -2.77x10-5 | -0.000289 | 0.00368 | -0.0784 | 0.93700 |
Chi-Squared = 26.81 on 8 df
Overall Model p-value = 0.000763
*6 observations removed due to lack of data
Table 3: Aalen regression model (N=242*, 34 out of 36 unique event times used).
| Variables | Slope | Coef | SE (Coef) | z | p-value |
|---|---|---|---|---|---|
| Intercept | -4.33x10-4 | -4.15x10-3 | 1.09x10-2 | -0.382 | 0.702 |
| Race | |||||
| Black or African American | -5.61x10-4 | -8.78x10-3 | 6.91x10-3 | -1.270 | 0.204 |
| More Than One Race | 4.78x10-5 | 2.85x10-3 | 1.38x10-2 | 0.206 | 0.837 |
| Native Hawaiian or Pacific Islander | -1.95 | -2.04x10-2 | 2.76x10-2 | -0.737 | 0.461 |
| White | -3.11x10-4 | -3.70x10-3 | 6.54x10-3 | -0.565 | 0.572 |
| Unknown /Not Reported | -3.37x10-4 | -4.42x10-3 | 8.70x10-3 | -0.508 | 0.612 |
| Ethnicity | |||||
| Not Hispanic or Latino | 1.07x10-5 | -7.31x10-4 | 4.72x10-3 | -0.155 | 0.877 |
| Unknown / Not Reported | 5.20x10-4 | 2.87x10-3 | 5.97x10-3 | 0.482 | 0.630 |
| Age | 5.68x10-6 | 5.48x10-5 | 9.13x10-5 | 0.601 | 0.548 |
| Gender | |||||
| Male | -6.22x10-5 | -1.21x10-3 | 2.48x10-3 | -0.487 | 0.626 |
| Protein- Calorie Deficit | 1.83x10-4 | 3.15x10-3 | 2.02x10-3 | 1.560 | 0.118 |
| MELD 3 | 6.62x10-5 | 6.05x10-4 | 2.51x10-4 | 2.410 | 0.016* |
Table 4: Welch T-test.
| Mean (Quadruple Therapy) | Mean (No Quadruple Therapy) | t | df | p-value | 95% CI | |
|---|---|---|---|---|---|---|
| Quadruple Therapy vs. No Quadruple Therapy | 0.9444444 | 0.7990868 | -3.0743 | 74.931 | 0.002943 | [-0.24, -0.05 |
Table 5: Showing regression evaluation total hospitalization for each medication, early l-carnitine found to be significant for association with increased total hospitalizations.
| Coefficients | Estimate | Std. Error | t-value | Pr(>|t|) |
|---|---|---|---|---|
| Intercept | 0.056506 | 0.183390 | 0.308 | 0.7583 |
| At the patient's first visit with the hepatology team or upon discharge after their first hospitalization with Hepatic Encephalopathy: | ||||
| Lactulose | 0.206533 | 0.178598 | 1.156 | 0.2487 |
| Rifaximin | 0.074601 | 0.091690 | 0.814 | 0.4167 |
| Zinc | -0.008889 | 0.095391 | -0.093 | 0.9258 |
| L-carnitine | 0.477235 | 0.197541 | 2.416 | 0.0164* |
| At the patient's most recent contact with the hepatology team, or before transplant: | ||||
| Lactulose | -0.093852 | 0.153237 | -0.612 | 0.5408 |
| Rifaximin | 0.002751 | 0.118934 | 0.023 | 0.9816 |
| Zinc | 0.093118 | 0.092946 | 1.002 | 0.3174 |
| L-carnitine | 0.143182 | 0.125137 | 1.144 | 0.2537 |
Residual standard error = 0.5583 on 240 degrees of freedom (7 observations deleted due to missingness)
Multiple R-squared = 0.09101
Adjusted R-squared = 0.06071
F-statistic = 3.004 on 8 and 240 DF
p-value = 0.003137
Table 6: Showing readmission rates, results suggesting early zinc to be protective for re- admission rates, with rifaximin and zinc at last visit both associated with increased rates of re- admission.
| Coefficients | Estimate | Std. Error | t-value | Pr(>|t|) |
|---|---|---|---|---|
| Intercept | -0.03938 | 0.92328 | -0.043 | 0.96601 |
| At the patient's first visit with the hepatology team or upon discharge after their first hospitalization with Hepatic Encephalopathy: | ||||
| Lactulose | 0.50572 | 0.89615 | 0.564 | 0.57305 |
| Rifaximin | -0.18662 | 0.45862 | -0.407 | 0.68442 |
| Zinc | -1.21518 | 0.47681 | -2.549 | 0.01143* |
| L-carnitine | -1.46336 | 0.99578 | -1.470 | 0.14296 |
| At the patient's most recent contact with the hepatology team, or before transplant: | ||||
| Lactulose | 0.02184 | 0.74901 | 0.029 | 0.97676 |
| Rifaximin | 1.19540 | 0.59476 | 2.010 | 0.04554* |
| Zinc | 1.49838 | 0.46339 | 3.234 | 0.00139* |
| L-carnitine | 0.57318 | 0.62906 | 0.911 | 0.36310 |
Residual standard error = 2.816 on 245 degrees of freedom (2 observations deleted due to missingness)
Multiple R-squared = 0.1116
Adjusted R-squared = 0.0826
F-statistic = 3.847 on 8 and 245 DF
p-value = 0.0002759
Table 7: Propensity score matching summary for quadruple therapy patients.
| Characteristic | Description |
|---|---|
| Matching method | 1:1 Nearest Neighbor Matching (Without Replacement) |
| Distance metric | Propensity Score (estimated via Logistic Regression) |
| Matching estimand | ATT (Average Treatment effect on the Treated) |
| Number of observations | 256 (Original Sample), 72 (Matched Sample) |
| Matched groups | 36 Quadruple Therapy Patients matched with 36 Similar Controls |
| Matching covariates | - Age |
| - Protein-Calorie Malnutrition | |
| - Presence of TIPS | |
| - Known Portosystemic Shunt | |
| - MELD 3.0 Score | |
| - West Haven Score |
Table 8: Welch’s t-Test showing association between quadruple therapy and reduced readmissions. After propensity matching, receipt of quadruple therapy was associated with statistically significant reduction in readmissions, 0.64 readmissions every 30 days in the quadruple therapy recipient group vs. 2.23 readmissions every 30 days in the matched group that did not receive quadruple therapy (p=0.0013).
| Characteristic | Value |
|---|---|
| Test Type | Welch Two-Sample t-Test |
| Comparison Groups | Quadruple Therapy: Yes vs. No |
| Test Statistic (t) | 3.37 |
| Degrees of Freedom (df) | 62.28 |
| p-Value | 0.0013* |
| 95% Confidence Interval | [0.65, 2.54] |
| Mean Readmissions (No Group) | 2.23 |
| Mean Readmissions (Yes Group) | 0.64 |
Supplemental materials attached evaluated risks of etiology of liver disease and additional risk factors for readmission in our population.
After propensity score matching, Welch Two Sample T-test demonstrated a statistically significant reduction in readmis sion rates in quadruple therapy recipients compared to their matched cohort (p=0.0013) (mean readmissions at 0.64 per 30 days in quadruple therapy recipients vs. 2.23 per 30 days in the matched cohort of no quadruple therapy receipt) (Table 8).
Discussion
This retrospective observational study evaluated the effect of lactulose, rifaximin, zinc, and L-carnitine “quad therapy” on HE-related outcomes, including hospitalization, readmission, and survival, in a cohort of cirrhotic patients. Our retrospective findings help to identify new insights into the evolving role of adjunctive therapy in the management of HE, particularly when these interventions are initiated early in the disease course.
Zinc supplementation emerged as the most consistently beneficial agent, with early use associated with reduced hospi talization rates. Patients with receipt of zinc early also had some evidence of improved survival, but not quite meeting statisti cal significance. These findings align with previous reports that have identified zinc as a critical cofactor in urea cycle enzymes and a modulator of intestinal ammonia production. Yoshiji et al demonstrated that zinc administration improved event- free survival in cirrhotic patients, driven by improvements in hyper ammonemia and sarcopenia. This supports our observation that zinc has a meaningful impact on clinical outcomes when integrated into HE therapies early in the disease trajectory [25].
The significant association between initiation of quadru ple therapy and reduced readmissions after propensity score matching points to potential additive or synergistic effects when targeting multiple pathophysiologic pathways, including ammonia production, gut microbiome modulation, improve ment in sarcopenia and mitochondrial metabolism. Our find ings suggest that a comprehensive pharmacologic strategy may outperform standard dual therapy alone particularly in patients with difficult to manage HE.
We also identified that receipt of L-carnitine was associated with higher total hospitalization rates in our unadjusted models. This at first seems to contrast studies reporting neurocognitive improvements from L-carnitine. Malaguarnera et al observed reductions in ammonia levels and improvements in psychomet ric tests with L-carnitine therapy, and multiple studies show mechanistic evidence supporting L-carnitine’s role in neurologic improvement [26-31]. However, early L-carnitine receipt in our population may instead correlate to severity of disease.
Our study also included multiple survival and readmissions sub-analyses not mentioned above, including pain-stainking comparisons of each possible combination of all four medica tions, but showed no statistically significant findings or interest ing trends not otherwise mentioned above.
Conclusion
Early zinc supplementation in patients with hepatic encepha lopathy was associated with reduced readmissions for hepatic encephalopathy. Propensity matching identified that our sickest patients did no different in terms of survival while taking qua druple therapy, but patients taking all four of lactulose, rifaxi min, zinc and l-carnitine did benefit from significantly fewer re admissions. These results reinforce the need to consider timely, multidrug approaches in managing hepatic encephalopathy, and highlight key areas for future prospective trials [32].
References
- Elsaid MI, Rustgi VK. Epidemiology of hepatic encephalopathy. Clin Liver Dis. 2020; 24: 157–174.
- Zielińska M, Popek M, Albrecht J. Roles of changes in active glutamine transport in brain edema development during hepatic encephalopathy: an emerging concept. Neurochem Res. 2014; 39: 599–604.
- Lemberg A, Fernández MA. Hepatic encephalopathy, ammonia, glutamate, glutamine and oxidative stress. Ann Hepatol. 2009; 8: 95–102.
- Rudler M, Weiss N, Bouzbib C, Thabut D. Diagnosis and management of hepatic encephalopathy. Clin Liver Dis. 2021; 25: 393–417.
- Harris KB, Gonzalez HC, Gordon SC. The health care burden of hepatic encephalopathy. Clin Liver Dis. 2024; 28: 265–272.
- Rose CF, Amodio P, Bajaj JS, et al. Hepatic encephalopathy: novel insights into classification, pathophysiology and therapy. J Hepatol. 2020; 73: 1526–1547.
- Krishnarao A, Gordon FD. Prognosis of hepatic encephalopathy. Clin Liver Dis. 2020; 24: 219–229.
- Riggio O, Celsa C, Calvaruso V, et al. Hepatic encephalopathy increases the risk for mortality and hospital readmission in decompensated cirrhotic patients: a prospective multicenter study. Front Med (Lausanne). 2023; 10: 1184860.
- Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010; 362: 1071–1081.
- Hoilat GJ, Suhail FK, Adhami T, John S. Evidence-based approach to management of hepatic encephalopathy in adults. World J Hepatol. 2022; 14: 670–681.
- Poh Z, Chang PE. A current review of the diagnostic and treatment strategies of hepatic encephalopathy. Int J Hepatol. 2012; 2012: 480309.
- Sharma BC, Sharma P, Agrawal A, Sarin SK. Secondary prophylaxis of hepatic encephalopathy: an open-label randomized controlled trial of lactulose versus placebo. Gastroenterology. 2009; 137: 885–891.e1.
- Kimer N, Krag A, Møller S, Bendtsen F, Gluud LL. Systematic review with meta-analysis: the effects of rifaximin in hepatic encephalopathy. Aliment Pharmacol Ther. 2014; 40(2): 123-32. doi: 10.1111/apt.12803. Epub 2014 May 21. PMID: 24849268.
- Bass NM, Mullen KD, Sanyal A, Poordad F, Neff G, Leevy CB, Sigal S, Sheikh MY, Beavers K, Frederick T, Teperman L, Hill ebrand D, Huang S, Merchant K, Shaw A, Bortey E, Forbes WP. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010; 362(12): 1071-81. doi: 10.1056/NEJMoa0907893. PMID: 20335583.
- Bass NM, Mullen KD, Sanyal A, Poordad F, Neff G, Leevy CB, Sigal S, Sheikh MY, Beavers K, Frederick T, Teperman L, Hillebrand D, Huang S, Merchant K, Shaw A, Bortey E, Forbes WP. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010; 362(12): 1071-81. doi: 10.1056/NEJMoa0907893. PMID: 20335583.
- Kang DJ, Kakiyama G, Betrapally NS, Herzog J, Nittono H, Hylemon PB, Zhou H, Carroll I, Yang J, Gillevet PM, Jiao C, Takei H, Pandak WM, Iida T, Heuman DM, Fan S, Fiehn O, Kurosawa T, Sikaroodi M, Sartor RB, Bajaj JS. Rifaximin Exerts Beneficial Effects Independent of its Ability to Alter Microbiota Composition. Clin Transl Gastroenterol. 2016; 7(8): e187. doi: 10.1038/ctg.2016.44. PMID: 27560928; PMCID: PMC5543406.
- Fu J, Gao Y, Shi L. Combination therapy with rifaximin and lactulose in hepatic encephalopathy: a systematic review and meta-analysis. PLoS One. 2022; 17: e0267647.
- Ridola L, Faccioli J, Nardelli S, Gioia S, Riggio O. Hepatic encephalopathy: diagnosis and management. J Transl Int Med. 2020; 8: 210–219.
- Chavez-Tapia NC, Cesar-Arce A, Barrientos-Gutiérrez T, et al. A systematic review and meta-analysis of the use of oral zinc in the treatment of hepatic encephalopathy. Nutr J. 2013; 12: 74.
- Shen YC, Chang YH, Fang CJ, Lin YS. Zinc supplementation in patients with cirrhosis and hepatic encephalopathy: a systematic review and meta-analysis. Nutr J. 2019; 18: 34.
- Janyajirawong R, Vilaichone RK, Sethasine S. Efficacy of zinc supplement in minimal hepatic encephalopathy: a prospective randomized controlled study. Asian Pac J Cancer Prev. 2021; 22: 2879–2887.
- Diglio DC, Fernandes SA, Stein J, et al. Role of zinc supplementation in the management of chronic liver diseases: a systematic review and meta-analysis. Ann Hepatol. 2020; 19: 190–196.
- Ohara M, Ogawa K, Suda G, et al. L-carnitine suppresses loss of skeletal muscle mass in patients with liver cirrhosis. Hepatol Commun. 2018; 2: 906–918.
- Tani J, Morishita A, Sakamoto T, et al. L-carnitine reduces hospital admissions in patients with hepatic encephalopathy. Eur J Gastroenterol Hepatol. 2021; 32: 288–293.
- Martí-Carvajal AJ, Gluud C, Arevalo-Rodriguez I, Martí-Amarista CE. Acetyl-L-carnitine for patients with hepatic encephalopathy. Cochrane Database Syst Rev. 2019; 1: CD011451.
- Malaguarnera M, Pistone G, Elvira R, et al. Effects of L-carnitine in patients with hepatic encephalopathy. World J Gastroenterol. 2005; 11: 7197–7202.
- Yoshiji H, Noguchi R, Ikenaka Y, et al. Clinical impact of zinc administration for liver cirrhosis: a randomized controlled trial. Sci Rep. 2020; 10: 70585.
- Vilstrup H, Amodio P, Bajaj JS, et al. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by AASLD and EASL. Hepatology. 2014; 60: 715–735.
- Malaguarnera M, Vacante M, Giordano M, et al. The role of acetyl-L-carnitine in minimal hepatic encephalopathy. J Gastrointestin Liver Dis. 2019; 28: 77–85.
- Martí-Carvajal AJ, Gluud C, Arevalo-Rodriguez I, Martí-Amarista CE. Acetyl-L-carnitine for patients with hepatic encephalopathy. Cochrane Database Syst Rev. 2019; 1: CD011451.
- Nakanishi H, Hayakawa Y, Kubota Y, et al. Impaired brain function improved by L-carnitine in patients with cirrhosis: evaluation using near-infrared spectroscopy. Sci Rep. 2020; 10: 13566.
- Kamath PS, Kim WR. The model for end-stage liver disease (MELD). Hepatology. 2007; 45: 797–805.