
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 6
Beyond proton pump inhibitors: Vonoprazan in acid related diseases
Jain Kashish S1; Raval Adarsh V1; Zine Sandip P2*
1Research Student, Department of Quality Assurance, SVKMs Dr. Bhanuben Nanavati College of Pharmacy, India.
2Assistant Professor, Department of Pharmaceutical Chemistry, SVKMs Dr. Bhanuben Nanavati College of Pharmacy, India.
*Corresponding Author : Zine Sandip P
Assistant Professor, Department of Pharmaceutical
Chemistry, SVKMs Dr. Bhanuben Nanavati College of
Pharmacy, India.
Tel: 8369586929;
Email: sandip.zine@bncp.ac.in
Received : Jan 05, 2026
Accepted : Feb 05, 2026
Published : Feb 12, 2026
Archived : www.jjgastro.com
Copyright : © Sandip ZP (2026).
Abstract
Although Proton Pump Inhibitors (PPIs) are indispensable in the treatment of acid-related diseases, there are several restric tions in the use of PPIs. These include the prolonged onset of ac tion, interindividual variability, and pH-dependence. Vonoprazan, a Potassium-Competitive Acid Blocker (P-CAB), has an extremely strong and long-lasting antisecretory effect. The following is an unstructured review that includes basic researches, Randomized Clinical Trials, and review papers, as well as real data and its use as an off-label drug. The drug has demonstrated enhanced rates of wound healing in patients with Gastro Esophageal Reflux Diseases and Peptic Ulcer Diseases, a higher eradication rate of Helicobacter pylori, and gastric acidity control compared with PPI therapy. In terms of the overall rebound acid secretion and hypergastrinemi as, the safety profile of the drug is similar to that of PPI therapy. New indications of the drug involve GERD, Barrett’s esophagus, and Zollinger-Ellison syndrome. This medication holds a promise of an entire paradigm shift in the management of various conditions associated with acid reflux. Their long-term basic research will as sert its classified placement in this regard.
Keywords: Vonoprazan; Potassium-competitive acid blockers (P-CABs); Proton Pump Inhibitors (PPIs); Gastroesophageal Reflux Disease (GERD); Helicobacter pylori eradication; Acid-related disorders; Erosive esophagitis; Gastric acid suppression.
Abbreviations: PPI: Proton Pump Inhibitor; P-CAB: Potassium Competitive Acid Blocker; GERD: Gastroesophageal Reflux Disease; H.pylori: Helicobacter pylori; VPN: Vonoprazan; NSAID: Nonsteroidal Anti-Inflammatory Drug; EE: Erosive Esophagitis; EoE: Eosinophilic Esophagitis; LDA: Low-Dose Aspirin; LA: Los Angeles; GU: Gastric Ulcer; DU: Duodenal Ulcer; FD: Functional Dyspepsia; MALT: Mucosa-Associated Lymphoid Tissue; ECL: Enterochromaffin Like Cells; Cmax: Maximum Plasma Concentration; RCT: Randomized Controlled Trial; LPZ: Lansoprazole; ESD: Endoscopic Submucosal Dissection; CYP: Cytochrome P450; ATPase: Adenosine Triphosphatase; TKI: Tyrosine Kinase Inhibitor; DDI: Drug–Drug Interaction
Citation: Kashish J, Adarsh R, Sandip ZP. Beyond proton pump inhibitors: Vonoprazan in acid related diseases. J Gastroenterol Res Pract. 2026; 6(2): 1247.
Introduction
The “gastric acid-related disorders” are actually a broad spectrum of diseases brought about by either excess or inappropriate secretion of the gastric juices. These include GERD, PUD, and Helicobacter pylori infections. The symptoms of heartburn, regurgitation, and even Esophageal injury are manifestations of GERD, which are brought about by the aberrant reflux of these juices into the esophagus itself [1]. As for gastric acid disorders, it would be important for effective management of such disorders considering the fact that such disorders actually threaten lives under extreme scenarios [1]. There are actually disorders brought about by the chronic aspect of disorders such that Esophagitis, Barrett Esophagus, and even the increased susceptibility to Esophageal Carcinomas all exist. The catastrophic consequences of such disorders precipitating Bleeding, Perforation, and even gastric outlet obstruction actually exist under peptic ulcers [2]. Esophagitis and disabilities with regard to day-to-day activities are also precipitated by such disorders associated with gastro-esophageal reflux disease or GERD or even Esophagitis, which are actually quite common disorders such that refluxing precipitates actually through the reflux of stomach content into the Esophagus itself [3].
The “prevalence” of GERD under individuals belonging to the group under Northern America actually stands at an alarmingly high level of 18.1%-27.8%, European health groupings actually stands at quite high risk with regard to health actually at 8.8% 25.9%, The groupings under Asia stands actually quite low pass ing at 2.5%-7.8% [4].
Although GERD has historically been less common in Asian populations than in Western ones, it has recently exhibited a sharply rising tendency in Asia [5].
The impact of GERD on health care use and medical expen diture has been substantial because of the widespread nature and chronic characteristics of this disease [6]. GERD is the most common gastrointestinal illness that has been reported from outpatient clinic visits in the US [7], and the annual medical bills for this disease approximate $15 billion–20 billion [8].
Proton Pump Inhibitors (PPIs), for example, are widely used in the treatment of acid-related disorders including Gastro esophageal Reflux Disease (GERD), stomach and duodenal ul cers, Ulcers induced by the use of NSAIDS, and the eradication treatment of Helicobacter pylori [9].
The traditional PPIs Include benzimidazole drugs, which ir reversibly inhibit the enzyme hydrogen potassium (H+, K+) ATPase, which is found in the parietal cells of the stomach and is primarily responsible for the production of H+ ions, thereby making the PPIs more effective inhibitors of acid secretion in the stomach compared to the histamine H2 receptor antago nists [10]. Despite the widespread use of PPIs by prescribing them as the first line of treatment for the aforementioned dis eases, it has become evident that there is a lot of difficulties which need to be improved [11]. First, it takes several days to reach the maximal effect. Due to the slow start of the effect, only one-third of the reflux symptoms of patients suffering from GERD can be relieved after the first administration of PPI medi cations. Further, one-half of them tolerate the pain even after taking the drugs for three consecutive days. Third, it has poor night-time performance. Finally, PPI can only function in an acid environment, meaning that the PPI is unstable under acidic con ditions. Therefore, the enteric coating of the latter is required [12]. In addition, there is a considerable amount of empirical data available regarding the several negative consequences as sociated with the chronic administration of PPI, such as the in duction of dementia, osteoporosis, ischemic-heart disease, and renal damage [13-15].
Vonoprazan (Voquezna®), the world’s first PCAB-monoiso form, is also evaluated as part of combination regimens for H. pylori infections. In 2014, this drug received the first permit to launch within Japan due to its use [16]. Based on ‘Phase 3 trial PHALCON HP: A randomized active-controlled clinical study in the USA and Europe, vonoprazan is now approved to use in combination with Amoxicillin or Amoxicillin in combination with Clarithromycin in the USA for adults to treat H. pylori infections [17], following vonoprazan’s formulation change to address concerns over residues of nitrosamine impurities in earlier commercial product [18]. Moreover, vonoprazan is approved for use in adults for all grades of erosive esophagitis in the USA as monotherapy to relieve symptoms of heartburn to heal and maintain [19].
A new class of Potassium-Competitive Acid Blocker (P-CAB), named Vonoprazan (VPN), was developed as an alternative to traditional Proton Pump Inhibitors (PPIs) for the treatment of conditions associated with excess stomach acid [20]. While PPIs work by inhibiting the H+/K+ ATPase enzyme of parietal cells of the stomach, VPN fully and competitively inhibits the potassium-binding site of the aforementioned enzyme, lead ing to faster and sustained reduction of stomach acid secretion. This makes the drug highly ideal for people experiencing con ditions associated with excess stomach acid, given its mecha nism of action which makes it more reliable and efficacious than PPIs for acid suppression [21]. VPN works by reversibly block ing potassium ions to suppress the action of H+, K+-adenosine triphosphatase (ATPase), thus lowering stomach acid secretion [22]. The advantage of using VPN over PPIs resides largely in its insensitivity to acid-stimulated action and its capacity to re liably provide a reasonably fast and sustained anti-acid action irrespective of diet and genetic predispositions [23].
Pharmacology of potassium-competitive acid blockers
Mechanism of action
The distinct interaction of vonoprazan with the gastric pump is due to its unique chemical structure, which has been de scribed as a pyrrole derivative with a sulfonyl group [24].
P-CABs have been found to be absorbed systemically, acting through reversible binding to the H+\K+ ATPase pump on the parietal cell of the stomach, also known as the ‘proton pump,’ by inhibiting access of potassium ions to the potassium binding site of the proton pump, thereby decreasing the secretion of gastric juice [25]. PCABs bind to both the active and inactive form of the proton pump, which is located in the cytoplasmic as well as the extracytoplasmic regions, respectively. Their intra cellular accumulation is also independent of pH. PCABs inhibit access of potassium ions to the potassium binding site of the pump through ion (reversible) binding [26].
In contrast to PPIs, which are acid-labile drugs, PCABs are stable in the acidic microenvironment of the stomach. Hence, they do not require a gastroprotector and chauffered nicely in neutral and acidic pH. The drug concentrate in the secretory canaliculi and are sequestered in the gastric mucosa. Directly and independently inhibit H+/K+-ATPase without activating them. Hence, they are not classified as a drug/prodrug [27].
Pharmacokinetics & pharmacodynamics
Chemically, Vonoprazan is represented as 1-[5-(2-fluorophenyl)-1-pyridin-3-ylsulfonylpyrrol-3-yl]-N methylmethanamine [33]. Vonoprazan fumarate has a novel chemical structure that belongs to the pyrrole derivatives, with a different chemical structure from the past P-CABs, such as SCH 28080 and AZD0865, with a benzimidazole ring, or revapra zan, with a pyrimidine ring [34]. Vonoprazan’s basic pKa value of 9.06 enables the compound to remain unchanged in the blood stream, hence diffusing easily into parietal cells. Later, when inside the highly acidic secretory canaliculi, the compound becomes protonated, hence “trapped,” leading to a marked concentration. The process of acid trapping has been shown to significantly increase the affinity of the compound with H⁺/K⁺ ATPase, an activity that leads to rapid, potent, and sustained inhibition of gastric acid secretion. Indeed, this is a marked dif ference from the past P-CAB agents [35]. In animal or simulation studies, Vonoprazan showed a marked affinity to the stomach parietal cell during the resting state or during the actively se creting state. Moreover, the affinity during the resting state was shown to be higher than the actively secreting state, but lanso prazole showed high affinity within the actively secreting state. Vonoprazan’s basic pKa (9.06) enables the compound to easily diffuse into the cell without needing a protonated form, hence leading to [36].
Pharmacokinetics
It is quickly absorbed, with maximum concentration achieved in 2 hours, although the half-life (t1/2) in human plas ma is much longer (approximately 7 hours in Japanese subjects dosed with 20 mg vonoprazan in an overnight fasted state) than in PP is (which have half-lives of t1/2=1 to 2 hours), as depicted in pharmacokinetic profile. Moreover, vonoprazan does not ne cessitate acid-catalysis for activation. Consequently, in investi gation of acid suppression activity, vonoprazan was shown to have equal efficacy when taken either pre- or post-breakfast ad ministration [37]. Notably, vonoprazan exhibited potent activ ity in acid suppression which persisted for an extended period from the very first day of administration in a dose-dependent manner, cumulating over an ensuing seven days. A practically complete achlorhydria was induced in Japanese as well as UK subjects treated with vonoprazan (40 mg) [38]. It is important to note that vonoprazan-induced acid inhibition was consider ably quicker and more profound compared to PPIs. The effects became observable already from the very first day of adminis tration. Even on Day 7, namely during already seven days when PPis stabilize to reach an equal acid suppression effect, vono prazan in comparison to esomeprazole (20 mg) and Rabeprazole (10 mg) clearly outperformed these two medications during acid-reducing activity (i.e., percentage of cumulative time with in which intragastric pH >4 was maintained in 24 hours) [39].
Drug-drug interactions
The study evaluated possible Drug Drug Interactions in vitro with rat liver microsomes and in vivo with ultra-performance liquid chromatography-tandem mass spectrometry for the de tection of probe drug metabolites in rat plasma.
Vonoprazan inhibits CYP3A4 (IC50: 22.48 µM), CYP2C9 (IC50: 18.34 µM), CYP2D6 (IC50: 3.62 µM), and CYP2B6 (IC50: 3.68µM Different cytochrome P-450 isoenzymes catalyze the two processes of initiation through hepatic metabolism, which constitute the biotransformation of clopidogrel. However, CY P2C19 is the major one involved in the process of activation. The hepatocellular metabolism of vonoprazan also takes place largely through CYP3A4. The combined therapy of vonoprazan or esomeprazole and clopidogrel must, therefore, be consid ered jointly due to the following reasons. Esomeprazole, on the other hand, is metabolized through the liver, largely CYP2C19, with a minor contribution from CYP3A4. However, they both can potentially inhibit CYP2C19, the major site of the possible metabolism and activation of clopidogrel in the liver [41].
The co-administration of voriconazole notably raises blood levels of vonoprazan due to the inhibitory effect of voriconazole on CYP3A4 metabolism. This leads to a high drug concentration and a decrease in its clearance. Excess drug can produce intense inhibition of gastric secretion and also increase the risk of hy pergastrinemia due to a higher drug concentration [42].
Vonoprazan showed a strong inhibitory effect on venlafaxine metabolism, which resulted in a significantly increased systemic exposure of venlafaxine and its O-desmethyl venlafaxine me tabolite [43].Vonoprazan shows higher strength and longer duration of gastric acid suppression. The co-administration of vonoprazan with Tyrosine Kinase Inhibitors leads to substantial underexpo sure, possibly because of the pronounced bioavailability reduc tion at higher gastric pH levels. Vonoprazan is contraindicated or to be used cautiously with these TKIs, possibly mandating alternative approaches to acid suppression [44].
Vonoprazan clinical applications and efficacy
GERD and erosive esophagitis
The most relevant Randomized Controlled Trials which stud ied and demonstrated effectiveness of conventional Proton Pump Inhibitors and Potassium-Competitive Acid Blocker (Vo noprazan) in managing GERD and Esophagitis is summarized be low. The main clinical findings, relief in early symptoms, rate of healing, and trial parameters presented in the tables highlight key determinants.
Faster healing of early lesions and similar heartburn relief for vonoprazan, greater efficacy for severe erosive esophagitis.
It provides faster relief of symptoms for severe erosive esophagitis, maintains long-term healing with reduced recur rence rates within 24-48 weeks, and has healing rates that are comparable to or even greater than standard PPIs [48].
The reduction of the average total GERD-Q score (from 11.96 to 8.92, p< 0.001) indicates that vonoprazan significantly decreased the incidence of symptoms related to reflux. More over, patients with vonoprazan showed significantly lower scores compared to patients with PPI therapy for the incidence of heartburn, regurgitation, and lack of sleep associated with GERD, respectively.
The effectiveness of vonoprazan 20 mg was significantly greater than Rabeprazole 10 mg and 15 mg of Lansoprazole added with Esomeprazole 10 mg and Omeprazole 10 mg. This implies that the dose can also be increased to 20 mg because vonoprazan 10 mg was not effective to prove its potential to produce a superior effect of GERD maintenance over the rec ommended PPIs in Japan [50].
H. Pylori eradication
Heliobacter pylori are the type of microaerophilic, spiral shaped, gram-negative bacteria that can be found inhabiting the human stomach mucosa, along with being the prime cause of many cases of gastro duodenal diseases [51].
H. pylori often causes chronic gastritis, which can also be associated with severe symptoms such as stomach cancer and MALT [52].
PPI-triple therapy has remained the mainstay of H. pylori therapy for over two decades in various parts of the globe in cluding the United States of America. This typically includes PPI, Clarithromycin, and either Amoxicillin or Metronidazole [53]. The efficacy rate has, however, decreased to lower than 80% in Europe and United States [54] owing to high levels of resistance to Clarithromycin [55].
Japan sees high prescribing of VAC triple therapy as the main treatment for anti-H. pylori, which has over a million prescrip tions per year [56], although resistance levels of clarithromycin to H. pylori are high [57].
Both Regimens had high rates of eradication; this includes 92.5% for high dose Amoxicillin/Vonoprazan, as well as 88.9% for the low dose. Strict adherence exceeded 955 in all groups, although adverse reactions were of mild nature (12-15%) with out any severe events. This draws the final conclusion that Vo noprazan’s strong acid suppression ability helps in amoxicillin therapy [58].
Dual therapy of vonoprazan and amoxicillin Eradication rates: 92.9%, noninferior to 91.9% for triple therapy, and similar safety profiles. The dual therapy regimens were superior when infections were caused by organisms resistant to clarithromy cin, 92.3% vs 76.2%. A 7-day home treatment of vonoprazan + amoxicillin is thus effective for eradication without having to resort to clarithromycin, especially when resistance rates are high [59].
Ulcers caused by NSAIDs
Owing to the fact that non-steroidal anti-inflammatory drugs and Low Dose Aspirin are recognized for their immunosuppres sive action on the mucosa that resists the acidity of the stomach through pathways related to the suppression of natural prosta glandins in the stomach mucosa [60], they are associated with unfavourable outcomes of bleeding ulcers and ulcers of the stomach or intestine [61]. As many as 20% of Asians are rec ognized to fall ill with Peptic ulcer diseases, which include acid related chronic conditions [62]. Among patients getting treat ment for bleeding ulcers, 7.6% had been using LDA in Japanese research [62].
In a separate study, it was determined that incidence of ulcers among of Low dose Aspirin-users was between 11.9% -15.2%, regardless of formulation of Aspirin [63].
In addition, certain observational studies have pointed out the increased use of LDA [64] as a major contributing factor for the onset of bleeding ulcers. 38(12.4%) of 305 patients on LDA had endoscopically detected ulcer lesions, as reported in the Japanese single institutional study [65].
Untreated ulcers can become recurrent or present as acute gastrointestinal bleeding. These are usually found in the stom ach (gastric ulcer, GU) or in the duodenum (duodenal ulcer, or DU) [66].
Helicobacter pylori infection and Nonsteroidal Anti-Inflamma tory Drug (NSAID) use are the two major risk factors associated with gastrointestinal injury and acid-related peptic ulcers [67].
When undergoing Low dose Aspirin therapy, proton pump inhibitors are used for the prevention of recurrent stomach or duodenal (peptic) ulcers; however, recurrent ulcers have been observed in some individuals showing that secondary prophy laxis is not completely effective [68].
Safety and tolerability
The three endpoints tested in all six trials included the heal ing rates at the 2-week, 4-week, and 8-week endpoints. Gener ally, the trial established that the healing rates in erosive esoph agitis margins were superior in Vonoprazan compared to PPI at the 2-week, 4-week, and also the 8-week endpoint [72].
A total of 40,937 patients with a history of lansoprazole use had 500 reported cases of microscopic colitis. On the other hand, among 11,102 patients with a history of vonoprazan use, there were only 55 reported cases of microscopic colitis [73].
Results from some research inquiry that excessive use of ac id-reducing medication can alter the microbial ecosystem of the intestines, thus predisposing one to an increased risk of Clos tridium difficile Infection [74].
For patients treated with vonoprazan and esomeprazole, H. pylori test negativity was observed in 20 out of 20 (100%) and 17 out of 18(94.4%) cases [75]
The listed adverse reactions of the drugs vonoprazan dual pak(both the vonoprazan and the amoxicillin) and vonoprazan triple pak (vonoprazan,amoxicillin, and clarithromycin) that oc curred in ≥2% of patients include Nasopharyngitis, Diarrhea, Constipation, Flatulence, Dyspepsia, Headache, and Abdominal pain.The serious adverse reactions listed, though <2% of pa tients, include but are certainly not limited to,blood disorders such as anemia and neutropenia, bone fractures, infections, and cardiac abnormalities such as QT prolongation [16].
Compared to PPIs, vonoprazan, which is safer and more tol erable, could decrease cases of diarrhea and loose stool in pa tients with acid reflux [76].
Patients with clarithromycin-resistant strains treated with the VAC regimen had significantly higher eradication rates than those treated with the lansoprazole, amoxicillin, and clarithro mycin regimen in post hoc analysis performed in phase III re search [77].
Vonoprazan had no impact on kidney function, according to the clinic data analysis of a small-scale randomized research trial involving patients with diabetic nephropathy, since serum creatinine levels and Estimated Glomerular Filtration Rate re mained unaltered after therapy. Relative to pretrial levels, a small, significant reduction was noticed in proteinuria, whereas there was little difference in PPI control. The tolerability was adequate, with no cases reported for acute kidney injury or kidney-associated adverse reactions [78].
Studies conducted on rats and rabbits at therapeutic doses of the drug showed insignificant abnormalities, although severe exposure caused mild skeletal retardations and decreased fetal weights, usually with maternal toxicity. In general, the outcome of the tests indicates the teratogenic potential is very low at the standard doses, but with a note of concern due to the unavail ability of any human pregnancy data [79].
Emerging indications and off-label uses
Vonoprazan and PPIs are among the most used acid inhibi tors for the management of bleeding and ulcers due to ESD. As stated in some research, vonoprazan proved as effective as PPIs for ulcers resulting from ESD [80].
Nonetheless, some studies showed a superiority of vonopra zan over PPIs in repairing ulcers resulting from ESD [81,82].
As stated by Takahashi et al., shrinkage ratios of less than 90% at the fourth week are indicative of delayed ulcer healing [83].
Within this small population of EoE patients, the study con ducted by Kuzumoto et al. revealed that the response rates for symptoms, endoscopy, and histology for vonoprazan 20mg were comparable to PPIs, and while numerically it was among the higher rates of complete relief of symptoms (75.7%), it was not statistically different [84].
Response rates in the 10mg and 20mg vonoprazan arms at the second week were 31.0% and 35.7% (p=0.937), at week four in the study they were 75.8% and 78.6% (p=1.00), and 72.4% and 75.9% at week 8 (p=0.24). There was no significant differ ence between the response rates in the two groups [85].
Very little information is available regarding the dosage of vonoprazan in treating Functional Dyspepsia [86].
Currently, four meta-analyses of Vonoprazan revealed con flicting results. One trial revealed Vonoprazan to be superior to PPIs in ulcer healing at 8 weeks after ESD [87], and in another trial, Vonoprazan was found to accelerate the healing process at 4 and 8 weeks after ESD [88].
A total of 13 studies, including 1,510 subjects, were identi fied which included reports of healing of ulcers and/or ratios of shrinkage of ESD-induced ulcers after vonoprazan [89].
Real world data
The reported adverse events were abdominal pain, palpita tions, headaches, loose motion, and nausea & vomiting. Among these, abdominal pain recorded the least number, while loose motion recorded the highest. Zuberi et al. observed that vono prazan dual therapy had fewer instances of adverse events and proved more tolerable than conventional triple therapy. Only a few patients in the vonoprazan group showed moderate events of nausea, vomiting, bloating, & diarrhea, yet none of these events were severe enough to warrant discontinuation of this therapeutic regimen [90].
A comparison of the safety and effectiveness of triple thera py with vonoprazan and triple therapy with PPI was carried out. The incidence of side effects was much lower and the tolerance was higher in the vonoprazan-based triple therapy compared to PPI-based therapy, as stated in the meta-analysis [91].
Likewise, another retrospective study found the efficacy of vonoprazan in PPI-resistant patients with GERD. In this study, vonoprazan 10 mgdaily was given to 24 patients with PPI-re sistant GERD. After one month of vonoprazan administration, there was a significant reduction in Izumo scoring (5.8±1.7 to 1.9±1.9, p<0.001), and symptoms of GERD also improved in 88% (21 out of 24) and 42% (10 out of 24) of patients without any adverse effects. In conclusion, vonoprazan 10 mgdaily is ef fective in PPI-resistant patients with GERD.
Out of 1,642 patients, 840(51.2%) were male and 802(48.8%) were female with a mean age of 39.81±14.61 years. The mean score of GerdQ was 20.37±15.87 at baseline, 7.24±8.15 in the second week, and 3.70±6.31 in the fourth week of treatment respectively (p<0.001). The eradication rate of H. pylori was 90.74%. The great percentage of patients had regurgitation of acid or heartburn for less than one day a week in more than 70% of the weeks. The great percentage of patients, 78.13% (1,283 patients), had a good compliance rate. The total patients with a mild side effect were 37(2.3%) patients.
Vonoprazan showed a marked efficacy in the prophylaxis of GERD symptoms, reducing the risk of the disease by alleviating symptoms, and it also completely eradicated the H. pylori infec tion with a high efficacy. In general, the drug Vonoprazan has shown effectiveness in treating PPI-resistant reflux esophagitis patients.
The trial involved 24 patients with PPI-refractory reflux esophagitis, 58.3% of whom had severe erosive esophagitis. The endoscopic healing of patients with esophagitis was 87.5%, including patients with severe esophagitis at 85.7%, at 4 weeks after switching from PPI to vonoprazan at a dose of 20 mg per day. Also, the symptoms of GERD were markedly improved the next day after changing anti-reflux drugs [93].
Vonoprazan markedly decreased the incidence of disorders caused by the release of stomach acid because it has a strong inhibitory effect on the release of the acid [94]. More than 95% of the subjects received either PPI or PCAB to prevent mucosal damage caused by aspirin [95].
The cumulative body of comparative data indicates that P CABs like vonoprazan and tegoprazan are genuine, or even pref erable, alternatives to PPIs in the case of acid-related diseases (GERD, esophagitis, ulcers) where rapid, potent, or sustained acid inhibition is needed [96,97].
Future directions and research gaps
Most of the research on Vonoprozan has continued to fo cus on the eradication of H. pylori. Vonoprazan dual and triple therapies are more effective than PPI-based regimens, especial ly in high clarithromycin-resistant rates, according to the latest research on RCTs and meta-analyses available [101]. There is a significant information gap with regard to pediatric/teenager GERD, with current pharmacokinetic studies in children aiming at identifying appropriate dosing, and expanding indications within the young group [99]. Long-term safety studies, such as VISION, are also important for tracking potential hazards like mucosal hyperplasia, Enterochromaffin Like Cells changes or neoplasia because of the potent and sustained acid-suppres sive effect that vonoprazan has, compared with PPIs [102]. Big clinical trials in China and Asia are evaluating effectiveness in various combinations of H. pylori resistances, real world compli ance rates, and differing healthcare environments; worldwide acceptance needs experiences from diverse populations [102] Vonoprazan proved to be more effective in healing and main taining compared to Lansoprazole in both mild and severe Ero sive Esophagitis despite being costly. The annual expenses for the Vonoprazan 10&20 mg group were expected to be €833.28 & €166.56 respectively, whereas for the Lansoprazole, the cost was estimated to be €330.96. Vonoprazan proved to be more ef fective in healing irrespective of the difference in the cost. Heal ing percentages compared to 71.1% of the healing rates of the Lansoprazole group for the Vonoprazan 10&20 mg in the case of mild disease were found to be 81.3% & 82.3% respectively. In the case of severe disease, healing percentages compared to the healing rates of the 61.5% & 74.7% of the Lansoprazole group for the Vonoprazan 10 & 20 mg were found to be 77.2%. Vonoprazan is costly, clinically effective in case The long-term use of vonoprazan has not been demonstrated to exert any kind of significant safety risk in randomized trials and programs, such as the VISION program, despite the fact that the highly effective acid inhibition and resulting elevation in gastrin concentrations mandate constant safety surveillance. The cost-effectiveness evaluations in progress are showing varying region-dependent results, which are nonetheless positive. Worldwide large-scale safety registration programs and real-world comparisons as well as new economic models are required for the precise de termination of the long-term vonoprazan safety benefits and cost value in healthcare settings [1,102,104].
Conclusion
Vonoprazan, as the first P-CAB on the market, substantially surpasses PPIs in terms of pharmacological efficacy and clini cal efficacy. Its rapid onset, phi independent activation, and CY P2C19 independent degradation allow frequent and prolonged acid reduction, resulting in better healing of erosive esophagitis, increased rates of H. pylori eradication, and successful treatment of refractive conditions. Safety, tolerance in short/intermediate term therapy are established based on results of major RCTS, while hypergastrinemia in long term therapy, CYP3A4 mediated pharmacokinetic interactions, therapy in patients with hepatic impairment, pediatrics, or cost issues remain as yet unclear. Conclusion: Vonoprazan is a viable option and often a superior alternative to PPIs, offering a lot of promise regarding shifting practice patterns for a spectrum of acidic diseases. If safety in the long term and cost performance continue to provide a suit able return on early efficacy, it should have a more defined role within that spectrum.

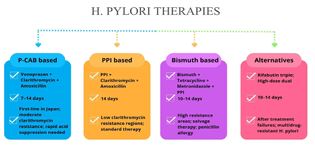

Table 1: Comparison of P-CABs and PPIs
| Parameter | Potassium-Competitive Acid Blockers (P-CABs) | Proton Pump Inhibitors (PPIs) |
|---|---|---|
| Chemical stability in acid | Stable under acidic conditions | Unstable in acid; require enteric coating for protection |
| Prodrug nature | Active in native form | Administered as prodrugs; activated in acidic environment to form sulfenamide intermediates |
| Binding characteristics [28] | Reversibly and ionically block K+ access to the gastric proton pump | Form irreversible covalent bonds with cysteine residues on active H+/K+-ATPase pumps |
| Elimination half-life (hours) [29] | Approximately 6-9 hours | Typically 1-2 hours |
| Timing of administration | Can be taken without regard to meals owing to longer duration of action [30] | Should be administered 30-60 minutes before food intake for optimal activation during peak acid secretion [31] |
| Dosing frequency for maximal acid suppression (days) [32] | Once daily often sufficient | Usually requires 3-5 days for maximum effect |
| Representative drugs | Vonoprazan, tegoprazan, fexuprazan, linaprazan, revaprazan, keverprazan. | Omeprazole, esomeprazole, lansoprazole, dexlansoprazole, pantoprazole, rabeprazole |
Table 2: Randomised clinical trials comparing vonoprazan and lansoprazole for the treatment of erosive oesophagitis.
| Study (Year) | Design/Patients | Treatment | Comparator | Healing rate (Eight weeks) | Early effect (two- four weeks) | Symptom relief/Key findings |
|---|---|---|---|---|---|---|
| Randomised Clinical Trial: Vonoprazan vs Lansoprazole for Healing of Erosive Oesophagitis. Alimentary Pharmacology & Therapeutics [45]. | Multicentre randomized controlled trial conducted in Japan involving patients with erosive esophagitis (LA Grades A-D). | Vonoprazan 20 mg once daily | Lansoprazole 30 mg once daily | 99.0% vs 95.5% | Not reported | Both groups showed high healing rates; Vonoprazan demonstrated sustained healing during maintenance. |
| Randomized, Double-Blind Study Comparing Vonoprazan and Lansoprazole in Asian patients with Erosive Esophagitis Gut [46]. | Phase III double-blind multicenter trial in Asian patients with erosive esophagitis. | Vonoprazan 20 mg once daily | Lansoprazole 30 mg once daily | 92.4% VS 1.3% | 75% vs 68% after two weeks (Vonoprazan considerably higher) | Vonoprazan produced faster restoration in patients with more severe Esophagitis (gradesC/D). |
| A Randomized trial comparing Vonoprazan and Lansoprazole for the treatment and maintenance of Erosive Esophagitis. Gastroenterology [47]. | Large international randomized controlled trial including North American and European patients with mild to severe erosive esophagitis (Grades A-D). | Vonoprazan 20 mg once daily | Lansoprazole 30 mg once daily | 92.9% vs 84.6% | Faster healing at 2 weeks, especially in severe (Grades C/D cases) | Vonoprazan provided faster early healing and comparable heartburn alliievation; better efficacy in severe erosive esophagitis. |
Table 3: Randomised controlled trials evaluating vonoprazan for ulcer healing and secondary prevention of NSAID- and low-dose aspirin associated peptic ulcers.
| Study | Design / Sample size | Primary endpoint | Key results |
|---|---|---|---|
| Mizokami et al. Gut 2018 (NSAID secondary prevention) [69] | RCT, n=642 (VPZ 10 mg, VPZ 20 mg, LPZ 15 mg) | Recurrent peptic ulcer at 24 weeks | VPZ10: 3.3%, VPZ20: 3.4%, LPZ 5.5%; Non-inferior |
| Kawai et al. Gut 2018 (LDA secondary prevention) [70] | RCT, n=621 (LPZ 15 mg, VPZ 10 mg, VPZ 20 mg) | Recurrent peptic ulcer at 24 weeks | LPZ: 2.8%, VPZ10: 0.5%, VPZ20: 1.5%; Non-inferior |
| Miwa et al. AP&T 2017 (Gastric ulcer) [71] | RCT, GU: VPZ n=231, LPZ n=225 | Healing of gastric ulcer at 8 weeks | VPZ: 93.5%, LPZ: 93.8%; Diff -0.3% (95% CI -4.75 to 4.21); Non-inferior |
| Miwa et al. AP&T 2017 (Duodenal ulcer) [71] | RCT, DU: VPZ n=178, LPZ n=180 | Healing of duodenal ulcer at 6 weeks | VPZ: 95.5%, LPZ: 98.3%; Diff -2.8% (95% CI -6.40 to 0.75); Non-inferiority not confirmed |
Table 4: Ongoing and recently registered clinical trials evaluating vonoprazan in Helicobacter pylori infection and gastro-oesophageal reflux disease.
| Trial/Study | Focus/Patient population | Status/Key notes |
|---|---|---|
| VA Dual Sequential Therapy NCT06929962 [98] | Vonoprazan + amoxicillin dual therapy for treatment-naïve Helicobacter pylori infection | Started April 2025; estimated completion December 2026. Open-label, randomized, multicenter. |
| Phase 1 pediatric GERD trial (adolescents or children with GERD) NCT05343364 [99] | Pharmacokinetics, pharmacodynamics, and safety of vonoprazan (10 or 20 mg daily) in pediatric patients with symptomatic GERD | Listed as concluded or updating (latest registry update April 2025) for adolescents; similar design for children 6-12 years. |
| NCT06564246-Vonoprazan vs Pantoprazole in GERD [100] | Vonoprazan 20mg vs Pantoprazole 40 mg in GERD patients; a comparison | Began in 2024, with a primary completion date of 2026, recruiting at the moment |
References
- Padwale V, Kirnake V, Daswani R, Kodmalwar A, Gupta A. A comprehensive review on the efficacy and safety of vonoprazan in the management of gastric acid-related diseases. Cureus. 2024.
- Dent J, Armstrong D, Delaney B, Moayyedi P, Talley NJ, Vakil N. Symptom evaluation in reflux disease: workshop background, processes, terminology, recommendations, and discussion outputs. Gut. 2004; 53: iv1–24.
- Tanvir F, Nijjar GS, Aulakh SK, Kaur Y, Singh S, Singh K, et al. Gastroesophageal reflux disease: new insights and treatment approaches. Cureus. 2024.
- Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: a meta-analysis. Gut. 2018; 67: 430–440.
- El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014; 63: 871–880.
- Gawron AJ, French DD, Pandolfino JE, Howden CW. Economic evaluations of gastroesophageal reflux disease medical management. Pharmacoeconomics. 2014; 32: 745–758.
- Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012; 143: 1179–1187.e3.
- Shaheen NJ, Hansen RA, Morgan DR, Gangarosa LM, Ringel Y, Thiny MT, et al. The burden of gastrointestinal and liver diseases, 2006. Am J Gastroenterol. 2006; 101: 2128–2138.
- Shanika LGT, Reynolds A, Pattison S, Braund R. Proton pump inhibitor use: systematic review of global trends and practices. Eur J Clin Pharmacol. 2023; 79: 1159–1172.
- Sachs G, Shin JM, Howden CW. Review article: the clinical pharmacology of proton pump inhibitors. Aliment Pharmacol Ther. 2006; 23: 2–8.
- Veettil SK, Sadoyu S, Bald EM, Chandran VP, Khuu SAT, Pitak P, et al. Association of proton pump inhibitor use with adverse health outcomes: an umbrella review. Br J Clin Pharmacol. 2022; 88: 1551–1566.
- Huang S, Li B, Pang XY, Gao WW. Efficacy and safety of vonoprazan-based treatment of Helicobacter pylori infection: a systematic review and network meta-analysis. BMC Infect Dis. 2024; 24: 953.
- Jaynes M, Kumar AB. The risks of long-term use of proton pump inhibitors: a critical review. Ther Adv Drug Saf. 2019; 10: 1–14.
- Park CH, Kim EH, Roh YH, Kim HY, Lee SK. The association between the use of proton pump inhibitors and the risk of hypomagnesemia: a systematic review and meta-analysis. PLoS One. 2014; 9: e112558.
- Xie Y, Bowe B, Li T, Xian H, Balasubramanian S, Al-Aly Z. Proton pump inhibitors and risk of incident CKD and progression to ESRD. J Am Soc Nephrol. 2016; 27: 3153–3163.
- Garnock-Jones KP. Vonoprazan: first global approval. Drugs. 2015; 75: 439–443.
- Chey WD, Mégraud F, Laine L, López LJ, Hunt BJ, Howden CW. Vonoprazan triple and dual therapy for Helicobacter pylori infection: randomized clinical trial. Gastroenterology. 2022; 163: 608–619.
- Phathom Pharmaceuticals. Phathom Pharmaceuticals reported nitrosamine impurity in their vonoprazan-based products. Nitrosamines Exchange [Internet]. [cited 2024 May 10]. Available from: https://nitrosamines.usp.org/news/phathompharmaceuticals-reported-nitrosamine-impurity-theirvonoprazan-based-products
- Shirley M. Vonoprazan: a review in Helicobacter pylori infection. Drugs. 2024; 84: 319–327.
- Fung S. Vonoprazan: a review in erosive esophagitis and non-erosive gastro-esophageal reflux disease. Drugs. 2025; 85: 945–955.
- Shin JM, Kim N. Pharmacokinetics and pharmacodynamics of the proton pump inhibitors. J Neurogastroenterol Motil. 2013; 19: 25–35.
- Zhang M, Xiao Y, Chen M. The role of vonoprazan in patients with erosive esophagitis. Therap Adv Gastroenterol. 2022; 15: 1–12.
- Miyazaki H, Igarashi A, Takeuchi T, Teng L, Uda A, Deguchi H, et al. Vonoprazan versus proton pump inhibitors for healing gastroesophageal reflux disease: a systematic review. J Gastroenterol Hepatol. 2019; 34: 1316–1328.
- Sakurai Y, Nishimura A, Kennedy G, Hibberd M, Jenkins R, Okamoto H, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of TAK-438 (vonoprazan) in healthy subjects. Clin Transl Gastroenterol. 2015; 6: e94.
- Patel A, Laine L, Moayyedi P, Wu J. AGA clinical practice update on integrating potassium-competitive acid blockers into clinical practice. Gastroenterology. 2024; 167: 1228–1238.
- Laine L, Sharma P, Mulford DJ, Hunt B, Leifke E, Smith N, et al. Pharmacodynamics and pharmacokinetics of vonoprazan and lansoprazole in US subjects. Am J Gastroenterol. 2022; 117: 1158–1161.
- Scarpignato C, Hunt RH. Potassium-competitive acid blockers: current clinical use and future developments. Curr Gastroenterol Rep. 2024; 26: 273–293.
- Sachs G, Shin JM, Vagin O, Lambrecht N, Yakubov I, Munson K. The gastric H,K-ATPase as a drug target. J Clin Gastroenterol. 2007; 41: S226–242.
- Yang X, Li Y, Sun Y, Zhang M, Guo C, Mirza IA, et al. Vonoprazan: a novel and potent alternative in the treatment of acid-related diseases. Dig Dis Sci. 2018; 63: 302–311.
- Hori Y, Matsukawa J, Takeuchi T, Nishida H, Kajino M, Inatomi N. Antisecretory effect of TAK-438 compared with lansoprazole. J Pharmacol Exp Ther. 2011; 337: 797–804.
- Mejia A, Kraft WK. Acid peptic diseases: pharmacological approach to treatment. Expert Rev Clin Pharmacol. 2009; 2: 295–314.
- Graham DY, Dore MP. Update on the use of vonoprazan: a competitive acid blocker. Gastroenterology. 2018; 154: 462–466.
- DrugBank Online. Vonoprazan: uses, interactions, mechanism of action. 2024. Available from: https://go.drugbank.com/drugs/DB11822
- Arikawa Y, Nishida H, Kurasawa O, et al. Discovery of TAK-438 as a potassium-competitive acid blocker. J Med Chem. 2012; 55: 4446–4456.
- Shin JM, Inatomi N, Munson K, et al. Characterization of TAK-438, a novel potassium-competitive acid blocker. J Pharmacol Exp Ther. 2011; 339: 412–420.
- Kong W, Sun B, Wang Z, et al. Pharmacokinetic–pharmacodynamic modeling of vonoprazan. Acta Pharmacol Sin. 2020; 41: 852-865.
- Echizen H. Pharmacokinetic and pharmacodynamic considerations of vonoprazan fumarate. Clin Pharmacokinet. 2016; 55: 409–418.
- Jenkins H, Sakurai Y, Nishimura A, et al. Safety and pharmacodynamics of repeated doses of TAK-438. Aliment Pharmacol Ther. 2015; 41: 636–648.
- Sakurai Y, Mori Y, Okamoto H, et al. Acid-inhibitory effects of vonoprazan compared with PPIs. Aliment Pharmacol Ther. 2015; 42: 719–730.
- Wang Y, Wang C, Wang S, et al. Cytochrome P450-based drug-drug interactions of vonoprazan. Front Pharmacol. 2020; 11: 1–12.
- Higuchi T, Yamade M, Takahashi S, et al. Influence of vonoprazan dosing on intragastric pH and clopidogrel function. Eur J Clin Pharmacol. 2022; 78: 955–963.
- Shen J, Wang B, Wang S, et al. Effects of voriconazole on vonoprazan pharmacokinetics in rats. Drug Des Devel Ther. 2020; 14: 2199–2206.
- Chen F, Jiang H, Xu J, et al. Effects of vonoprazan on venlafaxine pharmacokinetics. Drug Des Devel Ther. 2020; 14: 4815–4824.
- Xu ZY, Li JL. Drug–drug interactions with EGFR tyrosine kinase inhibitors. Onco Targets Ther. 2019; 12: 5467–5484.
- Ashida K, Sakurai Y, Hori T, et al. Vonoprazan vs lansoprazole for healing erosive oesophagitis. Aliment Pharmacol Ther. 2016; 43: 240–251.
- Xiao Y, Zhang S, Dai N, Fei G, Goh KL, Chun HJ, et al. Phase III, randomised, double-blind, multicentre study to evaluate the efficacy and safety of vonoprazan compared with lansoprazole in Asian patients with erosive oesophagitis. Gut. 2020; 69: 224–230.
- Laine L, DeVault K, Katz P, Mitev S, Lowe J, Hunt B, et al. Vonoprazan versus lansoprazole for healing and maintenance of healing of erosive esophagitis: a randomized trial. Gastroenterology. 2023; 164: 61–71.
- Oshima T, Igarashi A, Nakano H, Deguchi H, Fujimori I, Fernandez J. Network meta-analysis comparing vonoprazan and proton pump inhibitors for heartburn symptoms in erosive esophagitis. J Clin Gastroenterol. 2022; 56: 493–504.
- Niikura R, Yamada A, Hirata Y, Hayakawa Y, Takahashi A, Shinozaki T, et al. Efficacy of vonoprazan for gastroesophageal reflux symptoms in patients with proton pump inhibitor-resistant non-erosive reflux disease. Intern Med. 2018; 57: 2443–2450.
- Miwa H, Igarashi A, Teng L, Uda A, Deguchi H, Tango T. Systematic review with network meta-analysis: indirect comparison of the efficacy of vonoprazan and proton-pump inhibitors for maintenance treatment of gastroesophageal reflux disease. J Gastroenterol. 2019; 54: 718–729.
- Katelaris P, Hunt R, Bazzoli F, Cohen H, Fock KM, Gemilyan M, et al. Helicobacter pylori World Gastroenterology Organization global guideline. J Clin Gastroenterol. 2023; 57: 111–126.
- Malfertheiner P, Megraud F, Rokkas T, Gisbert JP, Liou JM, Schulz C, et al. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. 2022; 71: 1724–1762.
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG clinical guideline: treatment of Helicobacter pylori infection. Am J Gastroenterol. 2017; 112: 212–239.
- Nyssen OP, Bordin D, Tepes B, Pérez-Aisa Á, Vaira D, Caldas M, et al. European Registry on Helicobacter pylori management (Hp-EuReg): patterns and trends in first-line empirical eradication prescription and outcomes of 5 years and 21,533 patients. Gut. 2021; 70: 40–54.
- Argueta EA, Alsamman MA, Moss SF, D’Agata EMC. Impact of antimicrobial resistance rates on eradication of Helicobacter pylori in a US population. Gastroenterology. 2021; 160: 2181–2183.e1.
- Graham DY, Lu H, Shiotani A. Vonoprazan-containing Helicobacter pylori triple therapies contribution to global antimicrobial resistance. J Gastroenterol Hepatol. 2021; 36: 1159–1163.
- Shah SC, Iyer PG, Moss SF. AGA clinical practice update on the management of refractory Helicobacter pylori infection: expert review. Gastroenterology. 2021; 160: 1831–1841.
- Hu Y, Xu X, Liu XS, He C, Ouyang YB, Li NS, et al. Fourteen-day vonoprazan and low- or high-dose amoxicillin dual therapy for eradicating Helicobacter pylori infection: a prospective, open-label, randomized non-inferiority clinical study. Front Immunol. 2023; 13.
- Suzuki S, Gotoda T, Kusano C, Ikehara H, Ichijima R, Ohyauchi M, et al. Seven-day vonoprazan and low-dose amoxicillin dual therapy as first-line Helicobacter pylori treatment: a multicentre randomised trial in Japan. Gut. 2020; 69: 1019–1026.
- Sugano K, Matsumoto Y, Itabashi T, Abe S, Sakaki N, Ashida K, et al. Lansoprazole for secondary prevention of gastric or duodenal ulcers associated with long-term low-dose aspirin therapy: results of a prospective, multicenter, double-blind, randomized, double-dummy, active-controlled trial. J Gastroenterol. 2011; 46: 724–735.
- Nakashima S, Arai S, Mizuno Y, Yoshino K, Ando S, Nakamura Y, et al. A clinical study of Japanese patients with ulcer induced by low-dose aspirin and other non-steroidal anti-inflammatory drugs. Aliment Pharmacol Ther. 2005; 21: 60–66.
- Nema H, Kato M, Katsurada T, Nozaki Y, Yotsukura A, Yoshida I, et al. Investigation of gastric and duodenal mucosal defects caused by low-dose aspirin in patients with ischemic heart disease. J Clin Gastroenterol. 2009; 43: 130–132.
- Nakayama M, Iwakiri R, Hara M, Ootani H, Shimoda R, Tsunada S, et al. Low-dose aspirin is a prominent cause of bleeding ulcers in patients who underwent emergency endoscopy. J Gastroenterol. 2009; 44: 912–918.
- Shiotani A, Sakakibara T, Yamanaka Y, Imamura H, Tarumi KI, Manabe N, et al. Upper gastrointestinal ulcer in Japanese patients taking low-dose aspirin. J Gastroenterol. 2009; 44: 126–131.
- Wu J, Tang R. Managing peptic ulcer and gastroesophageal reflux disease in elderly Chinese patients: focus on esomeprazole. Clin Interv Aging. 2013; 8: 1433–1443.
- Sung JJY, Kuipers EJ, El-Serag HB. Systematic review: the global incidence and prevalence of peptic ulcer disease. Aliment Pharmacol Ther. 2009; 29: 938–946.
- Yeomans N, Lanas A, Labenz J, van Zanten SV, van Rensburg C, Rácz I, et al. Efficacy of esomeprazole (20 mg once daily) for reducing the risk of gastroduodenal ulcers associated with continuous use of low-dose aspirin. Am J Gastroenterol. 2008; 103: 2465–2473.
- Mizokami Y, Oda K, Funao N, Nishimura A, Soen S, Kawai T, et al. Vonoprazan prevents ulcer recurrence during long-term NSAID therapy: randomised, lansoprazole-controlled non-inferiority and single-blind extension study. Gut. 2018; 67: 1042–1051.
- Kawai T, Oda K, Funao N, Nishimura A, Matsumoto Y, Mizokami Y, et al. Vonoprazan prevents low-dose aspirin-associated ulcer recurrence: randomised phase 3 study. Gut. 2018; 67: 1033–41.
- Miwa H, Uedo N, Watari J, Mori Y, Sakurai Y, Takanami Y, et al. Randomised clinical trial: efficacy and safety of vonoprazan vs lansoprazole in patients with gastric or duodenal ulcers. Aliment Pharmacol Ther. 2017; 45: 240–52.
- Simadibrata DM, Syam AF, Lee YY. A comparison of efficacy and safety of potassium-competitive acid blocker and proton pump inhibitor in gastric acid-related diseases: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2022; 37: 2217–28.
- Nakanishi K, Uwai Y, Nabekura T. Vonoprazan-associated microscopic colitis and continued use after onset: a study using a Japanese pharmacovigilance database. In Vivo. 2025; 39: 2363–70.
- Yang M, Ren C, Yang Z. Vonoprazan may induce Clostridium difficile infection and nephrotoxicity. Gastroenterology. 2023; 164: 699.
- Miao J, Hu C, Tang J, Wang W, Wang Y, Men R, et al. Pharmacokinetics, safety, and tolerability of vonoprazan- or esomeprazole-based bismuth-containing quadruple therapy. Clin Pharmacol Drug Dev. 2023; 12: 1036–44.
- Gong H, Han D, Liu S, Liu C, Zhu X, Chen D. Adverse events of vonoprazan in the treatments of acid-related diseases: a systematic review and meta-analysis. Rev Esp Enferm Dig. 2022.
- Murakami K, Sakurai Y, Shiino M, Funao N, Nishimura A, Asaka M. Vonoprazan as a component of first- and second-line triple therapy for Helicobacter pylori eradication. Gut. 2016; 65: 1439–46.
- Ahmed RM, Soliman AR, Mohammed A. Vonoprazan attenuates proteinuria in diabetic kidney disease through potential direct renal mechanism. Sci Rep. 2025; 15: 41446.
- Li T, Qiao H, Yue P, Cai M, He X. Embryo–fetal toxicity assessment of vonoprazan in rats and rabbits. J Appl Toxicol. 2018; 38: 987–95.
- Hirai A, Takeuchi T, Takahashi Y, Kawaguchi S, Ota K, Harada S, et al. Comparison of the effects of vonoprazan and lansoprazole for treating endoscopic submucosal dissection-induced artificial ulcers. Dig Dis Sci. 2018; 63: 974–81.
- Ban H, Sugimoto M, Otsuka T, Murata M, Nakata T, Hasegawa H, et al. Letter: potassium-competitive acid blocker vs proton pump inhibitor for healing artificial ulcers. Aliment Pharmacol Ther. 2017; 46: 564–5.
- Horikawa Y, Mizutamari H, Mimori N, Kato Y, Fushimi S, Sato S, et al. Short-term efficacy of potassium-competitive acid blocker following gastric endoscopic submucosal dissection. Scand J Gastroenterol. 2018; 53: 243–51.
- Takahashi K, Sato Y, Kohisa J, Watanabe J, Sato H, Mizuno K, et al. Vonoprazan 20 mg vs lansoprazole 30 mg for endoscopic submucosal dissection-induced gastric ulcers. World J Gastrointest Endosc. 2016; 8: 716.
- Kuzumoto T, Tanaka F, Sawada A, Nadatani Y, Otani K, Hosomi S, et al. Vonoprazan shows efficacy similar to proton pump inhibitors in eosinophilic esophagitis. Esophagus. 2021; 18: 372–9.
- Bunchorntavakul C, Jaigla P. Efficacy of vonoprazan 10 mg and 20 mg for proton pump inhibitor-refractory functional dyspepsia. JGH Open. 2024; 8.
- Shinozaki S, Osawa H, Hayashi Y, Miura Y, Sakamoto H, Yano T, et al. Vonoprazan therapy is as effective as acotiamide therapy for functional dyspepsia without heartburn. J Gastrointestin Liver Dis. 2023; 32: 23–9.
- Kim EH, Park SW, Nam E, Lee JG, Park CH. Comparative efficacy of anti-ulcer medications after gastric endoscopic submucosal dissection. Surg Endosc. 2019; 33: 1271–83.
- Jaruvongvanich V, Poonsombudlert K, Ungprasert P. Vonoprazan versus proton-pump inhibitors for ESD-induced ulcers. Eur J Gastroenterol Hepatol. 2018; 30: 1416–21.
- Martin, Zhou Y, Meng CX, Takagi T, Tian YS. Vonoprazan vs proton pump inhibitors in treating post-ESD ulcers and preventing bleeding. Medicine (Baltimore). 2020; 99: e19357.
- Zuberi BF, Ali FS, Rasheed T, Bader N, Hussain SM, Saleem A. Comparison of vonoprazan–amoxicillin dual therapy with standard triple therapy for Helicobacter pylori eradication. Pak J Med Sci. 2022; 38.
- Lyu QJ, Pu QH, Zhong XF, Zhang J. Efficacy and safety of vonoprazan-based versus proton pump inhibitor-based triple therapy for Helicobacter pylori eradication: a meta-analysis of randomized clinical trials. Biomed Res Int. 2019; 2019: 1–8.
- Abbasi A, Siddiqui SA, Ram B, Khan JUA, Sheikh K, Ali A, et al. Real-world evidence to evaluate the efficacy and safety of vonoprazan in gastrointestinal disorders in the Pakistani population. Cureus. 2023; 15.
- Hoshino S, Kawami N, Takenouchi N, Umezawa M, Hanada Y, Hoshikawa Y, et al. Efficacy of vonoprazan for proton pump inhibitor-resistant reflux esophagitis. Digestion. 2017; 95: 156–61.
- Hatta W, Koike T, Abe H, Ogata Y, Saito M, Jin X, et al. Recent approach for preventing complications in upper gastrointestinal endoscopic submucosal dissection. DEN Open. 2022; 2.
- Sasaki S, Ota K, Sanomura M, Mori Y, Tanaka H, Hakoda A, et al. Widespread use of proton pump inhibitors or potassium-competitive acid blocker has changed the status of gastrointestinal bleeding in patients with ischemic heart disease: real-world data from high-volume centers. BMC Gastroenterol. 2024; 24: 177.
- Ahmed S, Asghar S, Khanzada M, Soxi F, Gundala Raja H, Gul M, et al. Comparing proton pump inhibitors and emerging acid-suppressive therapies in gastroesophageal reflux disease: a systematic review. Cureus. 2025; 17.
- Ouyang M, Zou S, Cheng Q, Shi X, Zhao Y, Sun M. Comparative efficacy and safety of potassium-competitive acid blockers versus proton pump inhibitors for peptic ulcer with or without Helicobacter pylori infection: a systematic review and network meta-analysis. Pharmaceuticals (Basel). 2024; 17: 698.
- ClinicalTrials.gov. Vonoprazan and amoxicillin dual therapy for Helicobacter pylori infection. Bethesda (MD): National Library of Medicine (US). 2025. Available from: https://clinicaltrials.gov/study/NCT06929962
- ClinicalTrials.gov. Pharmacokinetic study of vonoprazan in adolescents with gastroesophageal reflux disease. Bethesda (MD): National Library of Medicine (US); 2025. Available from: https://clinicaltrials.gov/study/NCT05343364
- ClinicalTrials.gov. Vonoprazan versus pantoprazole for gastroesophageal reflux disease. Bethesda (MD): National Library of Medicine (US); 2025. Available from: https://clinicaltrials.gov/study/NCT06564246
- Yu T, Lu T, Deng W, Yao D, He C, Luo P, et al. Microbiome and function alterations in the gastric mucosa of asymptomatic patients with Helicobacter pylori infection. Helicobacter. 2023; 28.
- Uemura N, Kinoshita Y, Haruma K, Yao T, Kushima R, Kanoo T. Rationale and design of the VISION study: a randomized, open-label study to evaluate the long-term safety of vonoprazan as maintenance treatment in patients with erosive esophagitis. Clin Exp Gastroenterol. 2018; 11: 51–6.
- Jeyarajan S, K T, Pimpalnerkar S, Deng EZ, Ahmad Z, Banerjee D, et al. Evaluating the cost-effectiveness of replacing lansoprazole with vonoprazan for treating erosive oesophagitis. BMJ Open Gastroenterol. 2025; 12: e001709.
- Ishii M, Kawai T, Tsujita K, Igarashi A, Suzuki M, Deguchi H, et al. Cost-effectiveness of vonoprazan compared with proton pump inhibitors in patients taking low-dose aspirin for secondary prevention of cardiovascular events in Japan. Circ J. 2023; 87.