
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 6
A typical presentation of Whipple’s disease: A case report challenging the classic triad
Ines Lassoued1*; Wafa Dahmani1,3; Nour Elleuch1,3; Sarra Mestiri2,3; Aya Hammami1,3; Ahlem Brahem1,3; Aida Ben Slama1,3; Sihem Hmissa2,3; Hanene Jaziri1,3; Mehdi Ksiaa1,3
1Department of Gastroenterology, Sahloul Hospital, Sousse, Tunisia.
2Department of Patholology, Sahloul Hospital, Sousse, Tunisia.
3Faculty of Medicine, Ibn El Jazzar, Sousse, Tunisia.
*Corresponding Author : Ines Lassoued
Department of Gastroenterology, Sahloul Hospital,
Sousse, Tunisia.
Email: lasswediness@gmail.com
Received : Jan 05, 2026
Accepted : Feb 02, 2026
Published : Feb 09, 2026
Archived : www.jjgastro.com
Copyright : © Lassoued I (2026).
Abstract
Whipple’s Disease (WD) is a rare, potentially life-threatening infection caused by Tropheryma whipplei, characterized by a diverse array of symptoms that complicate diagnosis. We present a case of a 64-year-old male with chronic gastrointestinal symptoms, predominantly abdominal pain and watery diarrhea, who notably lacked the classical arthralgias associated with WD. Histopathological examination of duodenal biopsies revealed PAS positive macrophages, confirming the diagnosis. The patient was treated with a standard antibiotic regimen, resulting in significant clinical improvement and complete symptom resolution. This case underscores the diagnostic complexities of WD and emphasizes the necessity for a high index of suspicion even in atypical presentations. Adherence to established treatment protocols is essential for achieving optimal patient outcomes.
Keywords: Whipple’s disease; Tropheryma whipplei; Chronic diarrhea; Chronic systemic infection.
Citation: Lassoued I, Dahmani W, Elleuch N, Mestiri S, Hammami A, et al. A typical presentation of Whipple’s disease: A case report challenging the classic triad. J Gastroenterol Res Pract. 2026; 6(2): 1246.
Introduction
Whipple’s Disease (WD) is a chronic, systemic, relapsing in fection caused by Tropheryma whipplei, an actinobacterium found widely in the environment. It is a rare condition, with a prevalence of 1-3 per 1,000,000, predominantly affecting middle-aged Caucasian men [1,2]. On average, patients are diagnosed at around 55 years of age, and approximately 85% of cases occur in males [3]. The disease presents with a broad spectrum of symptoms. In fact, the classic triad of diarrhea, weight loss, and arthralgias is well-documented; however atypi cal presentations can confound diagnosis, which leads to a real diagnostic challenge [4].
Herein we report a case of a 64-year-old male patient pre senting with chronic gastrointestinal symptoms and signs of malabsorption. This report contributes to the understanding of WD’s variable clinical presentations and emphasizes the need for maintaining a high index of suspicion for the disease in pa tients with unexplained chronic gastrointestinal complaints.
Case presentation
A 64-year-old man presented with a six-month history of progressive weight loss, fatigue, abdominal pain, nausea, and watery diarrhea. He reported no prior medical history, surger ies, or relevant travel history. Physical examination showed that he was conscious and cooperative but cachectic in appearance. The patient was afebrile and did not have palpable nodules or joint changes. Laboratory workup revealed iron deficiency ane mia (Hemoglobin 8.2 g/dl, ferritin 10 ng/mL) and hypoalbumin emia (28 g/dL) hypocholesterolemia (2 g/L). He did not have leukocytosis (6.5×109/L) or neutrophilia (4.7×109/L). Inflamma tory markers were elevated (C-reactive protein and erythrocyte sedimentation at 20 mg/dL and 90 mm, respectively). Serologic and stool evaluations for common infectious etiologies were negative. Celiac disease serology was also negative. Abdominal Computed Tomography (CT) demonstrated mesenteric lymph adenopathy.
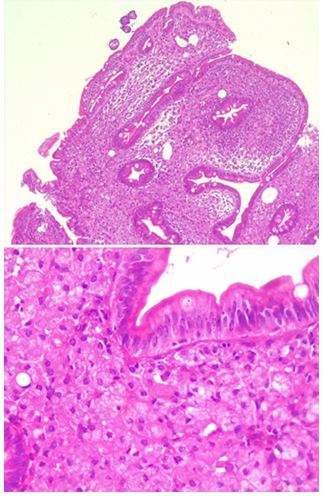
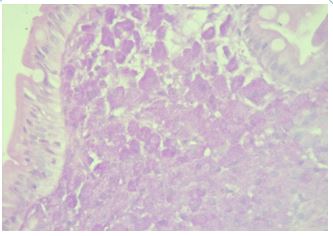
Esophagogastroduodenoscopy (EGD) showed thickened duodenal folds with whitish plaques diffusely distributed in the distal duodenum, while colonoscopy yielded normal results. Duodenal biopsies revealed PAS-positive macrophages in the lamina propria (Figures 1 & 2), confirming the diagnosis of WD.
The patient received intravenous ceftriaxone at a dosage of 2 g per day for two weeks, followed by a year-long course of oral trimethoprim (160 mg) and sulfamethoxazole (800 mg) taken twice daily. The patient began to show significant improvement within two weeks of starting the treatment and eventually ex perienced complete resolution of symptoms during a 12-month follow-up period.
Discussion
Whipple’s disease remains a rare but clinically significant condition characterized by its multisystemic involvement and diagnostic challenges. In this case report, the patient primarily presented with gastrointestinal symptoms including abdominal pain and chronic diarrhea, which are classic symptoms of WD. The absence of arthralgias in our case underscores the limita tions of relying solely on the classic triad for diagnosis. Previ ous reports support this observation. For example, Khrais et al. described a 67-year-old immunocompromised patient with HIV and WD who also lacked arthralgias [5]. Similarly, Kutlua et al. (2021) documented a case where WD manifested only with diarrhea and malabsorption, aligning with the gastrointestinal focused presentation observed in our patient [6].
Thus, WD, although rare, should be considered as a potential diagnosis for abdominal pain and chronic diarrhea due to its po tentially fatal outcome if untreated [7,8].
Given its potential for severe complications if left untreated, WD should be considered in the differential diagnosis for pa tients presenting with chronic abdominal pain and diarrhea, even in the absence of the complete symptom triad [7,8]. While our patient did not show systemic organ involvement, it is important to recognize that WD can also present with neu rological, ophthalmologic, pulmonary, cardiac, or hematologic manifestations. Such systemic involvement necessitates prompt diagnosis and treatment to prevent serious outcomes [7,9,10].
The treatment regimen employed in this case—initial in travenous ceftriaxone followed by a prolonged course of oral trimethoprim-sulfamethoxazole—aligns with established pro tocols that have demonstrated good prognoses and reduced relapse rates [7,11,12]. The patient’s response to treatment was prompt, with significant improvement observed within two weeks and complete resolution of symptoms thereafter. This outcome is consistent with previous literature supporting the efficacy of prolonged antibiotic therapy in achieving remission and preventing recurrence. Long-term follow-up will be manda tory to ensure sustained remission.
Conclusion
Whipple’s Disease (WD) presents a real diagnostic challenge due to its rarity and diverse symptomatology. This case under scores the critical need for clinicians to maintain a heightened suspicion of WD in patients presenting with chronic gastroin testinal symptoms even in the absence of the complete classic symptom triad.
In this instance, prompt diagnosis was facilitated through histopathological examination. This highlights the necessity for early recognition and initiation of treatment, crucial for prevent ing potentially fatal outcomes associated with untreated WD.
Continued vigilance and adherence to treatment protocols are imperative to mitigate the risk of relapse and ensure sus tained patient well-being.Clinicians should be aware of the diverse presentations of WD and not rely solely on the classic symptom triad for diag nosis. A thorough diagnostic evaluation and a high index of suspicion are essential for early detection and effective man agement. Continued vigilance and adherence to treatment pro tocols are key to optimizing patient outcomes and preventing the potentially severe consequences of untreated WD. This case serves to reinforce the need for a broad clinical perspective and meticulous diagnostic approach in managing this complex dis ease.
Declarations
Author’s contributions: W Dahmani, I Lassoued: Conceptu alization and Writing; N. Elleuch, A Hammami: Formal analysis; S. Mestiri and S. Hmissa: Formal analysis pathological findings; A Ben Slama, A Brahem: Supervision; H Jaziri and M Ksiaa: Vali dation.
Financial & competing interests’ disclosure: No relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript have been used. This includes employment, consultancies, hono raria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Disclosure of interest: We, as authors, declare that there are no conflicts of interest regarding the publication of this article.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research: This study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from the patient for publication of this case report and the accompanying images. According to institutional policy, ethical committee approval was not required for single-patient case reports.
References
- Schneider T, Moos V, Loddenkemper C, Marth T, Fenollar F, Raoult D. Whipple’s disease: new aspects of pathogenesis and treatment. Lancet Infect Dis. 2008; 8: 179–90.
- Biagi F, Balduzzi D, Delvino P, Schiepatti A, Klersy C, Corazza GR. Prevalence of Whipple’s disease in north-western Italy. Eur J Clin Microbiol Infect Dis. 2015; 34: 1347–8.
- Moos V, Schneider T. Changing paradigms in Whipple’s disease and infection with Tropheryma whipplei. Eur J Clin Microbiol Infect Dis. 2011; 30: 1151–8.
- Kucharz EJ, Kramza J, Grosicka A, Pieczyrak R. Clinical manifestations of Whipple’s disease mimicking rheumatic disorders. Reumatologia. 2021; 59: 104–10.
- Khrais A, Han B, Ramasamy D, Kumar S. Whipple’s disease without arthropathy in an immunocompromised patient. Cureus. 2022; 14
- Smith J, Doe A. Whipple’s disease mimicking celiac disease: a case report. Dig Dis. 2017; 35: 345–50
- Ruggiero E, Zurlo A, Giantin V, Piovan E, Rodella L, Pavan M, et al. Relapsing Whipple’s disease: a case report and literature review. Eur J Gastroenterol Hepatol. 2016; 28: 267–70.
- Loughran D, Beale L, Lodge F, Habboush H, Stock D. Whipple’s in the valleys: a case of Whipple’s with thrombocytopenia and endocarditis. J Clin Pathol. 2014; 67: 445–8.
- Kutlu O, Erhan SŞ, Gökden Y, Kandemir Ö, Tükek T. Whipple’s disease: a case report. Med Princ Pract. 2020; 29: 90–3.
- Sampaio F, Moreira J, Jordão S, Vieira B, Pereira S, Carvalho R. Whipple’s disease orbitopathy: case report and review of literature. Orbit. 2022; 41: 112–7.
- Dutly F, Altwegg M. Whipple’s disease and Tropheryma whippelii. Clin Microbiol Rev. 2001; 14: 561–83.
- Durand DV, Lecomte C, Cathébras P, Rousset H, Godeau P. Whipple disease: clinical review of 52 cases. The SNFMI Research Group on Whipple Disease. Medicine (Baltimore). 1997; 76: 170–84.