
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 6
Association between circulating inflammatory proteins and the risk of autoimmune liver diseases
Haifu Zhang#; Qinxia Zhang#; Shuojun Li; Yonghang Feng; Biyun Xie*
Fuyang Campus of Zhejiang Provincial People’s Hospital (The First People’s Hospital of Fuyang), China.
#These authors have been equally contributed to this article.
*Corresponding Author : Biyun Xie
Fuyang Campus of Zhejiang Provincial People’s Hospital
(The First People’s Hospital of Fuyang, No. 300 Zhujian
Road, Chunjiang Subdistrict, Fuyang District, Hangzhou,
Zhejiang, China.
Email: angisxie@163.com
Received : Dec 15, 2025
Accepted : Jan 23, 2026
Published : Jan 30, 2026
Archived : www.jjgastro.com
Copyright : © Xie B (2026).
Abstract
Background: Autoimmune Liver Diseases (AILDs) are chronic liver diseases that affect the liver and biliary tract mediated by abnormal autoimmune mechanisms. The pathogenesis of AILDs is intricate, involving a multitude of inflammatory factors and confounding variables. Therefore, it is imperative to conduct a Mendelian Randomization (MR) study to elucidate this correlation.
Materials and methods: The associations between 91 circulating inflammatory proteins and AILDs, including autoimmune hepatitis, primary biliary cholangitis, and primary sclerosing cholangitis, were examined using two-sample MR analysis, utilizing genetic variants predominantly of European ancestry obtained from genome wide association studies databases. Inverse variance weighted randomization methods, MR-Egger, and weighted median were used to analyze the causal association between 91 circulating inflammatory proteins and AILDs. The Steiger test was employed to infer the direction of causality.
Results: Our findings indicated that C-C motif chemokine 23, T-cell surface glycoprotein CD6, C-X-C motif chemokine (CXCL)10, CXCL9, monocyte chemoattractant protein-1, and tumor necrosis factor ligand superfamily member 12 were positively associated with the risk of AILDs. In contrast, CUB domain-containing protein 1, fibroblast growth factor 19, interleukin-18 receptor 1, IL-6, and Oncostatin-M were identified as protective factors.
Conclusion: CXCL10, combined with CXCL9, exhibits strong potential to predict patients with AILDs.
Keywords: Circulating inflammatory proteins; Autoimmune liver diseases; Autoimmune hepatitis; Primary biliary cholangitis; Primary sclerosing cholangitis.
Citation: Zhang H, Zhang Q, Li S, Feng Y, Xie B. Association between circulating inflammatory proteins and the risk of autoimmune liver diseases. J Gastroenterol Res Pract. 2026; 6(2): 1245.
Introduction
Autoimmune Liver Diseases (AILDs) are chronic liver diseas es that affect the liver and biliary tract mediated by abnormal autoimmune mechanisms, including Autoimmune Hepatitis (AIH), Primary Biliary Cholangitis (PBC), and Primary Sclerosing Cholangitis (PSC), which may occur individually or in combina tion [1]. The etiology of AILDs primarily stems from aberrant immune functionality, leading to non-suppurative inflammatory liver disease and the subsequent involvement of hepatocytes and bile duct epithelial cells [2]. Although AILDs are relatively uncommon in the general population, epidemiological statistics show that their incidence and prevalence are still on the rise, with an incidence of 0.1-4.39 per 100,000 people and a preva lence of 0.78-42.9 per 100,000 people [3].
The clinical characteristics of different AILDs vary, and their onset is often insidious, with a wide age distribution. The di agnosis of AILDs is complex and sometimes requires a liver bi opsy for confirmation [4]. Prolonged and intricate diagnostic processes often lead to poor patient cooperation, with some patients presenting with cirrhosis at the time of diagnosis, sig nificantly impacting prognosis [5]. Therefore, early identifica tion and diagnosis of AILDs are crucial, as timely intervention can effectively mitigate disease progression to end-stage liver disease and greatly improve the overall prognosis [6].
Due to the elusive pathogenesis of AILDs, comprehensive assessment typically involves combining biochemical markers, one or more autoantibodies, and histopathology [7]. Although liver needle biopsy is an important component in diagnosing patients with AILD, it carries risks and cannot be performed continuously [8]. Moreover, in developing countries, where acquiring autoantibodies can be challenging, diagnosis de pends entirely on clinical presentation, along with biochemical and histological criteria for AILD evaluation [9]. Consequently, identifying easily obtainable biomarkers for assessing and aid ing the diagnosis and treatment of AILDs is crucial for enhanc ing patient outcomes. Clinical studies have demonstrated that complex aberrant immune responses mediated by T cells and inflammatory cytokines play pivotal roles in the development and progression of AILDs [10].
Cytokines can be easily obtained and quantified, and cur rent research has indicated their significant involvement in the pathogenesis and progression of AILDs [11]. Serum Interleukin (IL)18 levels were found to be significantly elevated in clinically untreated patients with PBC and showed a significant decrease following treatment [12]. The cytokine IL10 exerts a downregu latory effect on the pro-inflammatory response, attenuates the hepatitis response, and retards liver fibrosis [13]. Concurrently, experimental studies in mice demonstrated that helper T cell (TH)1 and TH17 cells facilitate the upregulation of C-X-C mo tif chemokine (CXCL)9 and CXCL10 expression within the liver, thereby instigating the progression of AIH in murine models [14].
Mendelian Randomization (MR) is an approach employed to investigate causal relationships between exposure and outcomes of interest [15]. This methodology utilizes single nucleotide polymorphisms (SNPs) as unconfounded proxies for exposure, thereby circumventing the residual confounding and reverse causality commonly encountered in conventional observational studies [16]. The MR design represents a crucial strategy for inferring causality without relying on Randomized Clinical Trials (RCTs), as genetic variants are randomly assorted during meiosis, emulating the principles of an RCT [17]. The pathogenesis of AILDs is intricate, involving a multitude of in flammatory factors and confounding variables. Therefore, it is imperative to conduct an MR study to elucidate this correlation.
Materials and methods
In this study, all data were derived from the Genetic Alliance’s publicly available compilation of statistical data from Genome Wide Association Studies (GWAS). All original studies received specific ethical review and informed consent.
Study design
Summary statistics were collected on circulating inflamma tory proteins and AILDs from published GWAS. We aimed to ex plore the causal effect of circulating inflammatory proteins on the risk of AILDs using two-sample MR.
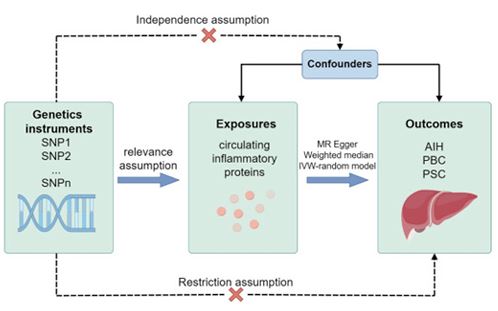
The MR Approach was built on the following three main as sumptions: (1) Genetic variants as Instrumental Variables (IVs) should be robustly associated with the risk factor of interest. (2) The genetic variants used should not be associated with po tential confounding factors. (3) Selected genetic variants affect the risk of outcome only by risk factors and not through other pathways (Figure 1).
This MR study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology using MR guidelines.
Outcome and exposure data source
The pooled data on circulating inflammatory proteins [18] and AILDs (AIH [19], PBC [20], PSC [21]) utilized in this study were obtained from publicly available GWAS datasets, predomi nantly comprising individuals of European ancestry. The GWAS Catalog database is publicly available for download at https:// www.ebi.ac.uk/gwas/. The details of the GWAS outcomes are presented in (Table 1).
Table 1: Characteristics of GWASs on inflammatory factors and AILDs.
| Phenotype | Year | PMID | Discovery ancestry | Sample size |
|---|---|---|---|---|
| Autoimmune hepatitis [19] | 2021 | 34594039 | European, East Asian | 906 cases 650942 control |
| Primary biliary cholangitis [20] | 2012 | 22961000 | European | 2861 case 8514 control |
| Primary sclerosing cholangitis [21] | 2017 | 27992413 | Utah residents with Northern and Western European, African, Han Chinese and Japanese | 2871 case 12019 control |
Genetic variants selection criteria
Genetic instruments for each exposure trait or disease were selected at the genome-wide significance threshold (P<5×10–5) from the corresponding GWASs. Independent SNPs were de fined by R2<0.01 and clump window >5 kb, and correlated SNPs (linkage disequilibrium) with the lowest P-values were retained.
Statistical analysis
In the primary analysis, we employed Inverse Variance Weighted (IVW) MR methods to estimate the association be tween 91 circulating inflammatory proteins and three AILDs along with their potential causal links [22]. Simultaneously, the MR-Egger and weighted median were used to assist in the judg ment of causality. The MR-Egger method was used to determine whether instrumental SNPs exhibited multiple effects [23]. The presence of potential horizontal pleiotropy and heterogeneity was considered and the intercept term in the MR-Egger re gression was used for testing significant horizontal pleiotropy. Additionally, MR-Egger regression was utilized to identify any existing heterogeneity. Furthermore, MR Steiger filtering was employed to examine the causal association between each identified SNP and both the exposure and outcome variables.
Results
Mendelian estimations
The associations between 91 circulating inflammatory pro teins (Supplementary Table 1) and AILDs (AIH, PBC, and PSC; Table 1) were examined using two-sample MR analysis, utiliz ing genetic variants predominantly from European ancestry ob tained from GWAS databases.
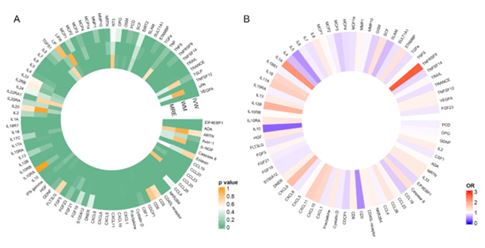
The IVW randomization methods, MR-Egger, and weighted median were used to analyze the causal association between 91 circulating inflammatory proteins and AIH (Figure 2A). The IVW randomization methods result as the primary outcome in dicators (Supplementary Table 1). Outcomes with a P< 0.05 for IVW randomization method outcomes were screened, and an OR was further used to express the association between ex posure and outcome (Figure 2B). The results demonstrated a positive correlation between AIH risk and tumor necrosis fac tor ligand superfamily member (TNFRSF)9 (OR: 2.67), IL1A, IL12B, CXCL9, CXCL11, IL17A, CXCL10, IL18, Caspase8, SCF, STAMBP, IL10RA, C-C motif chemokine (CCL)28, HGF, NRTN, IL33, Fractalkine, IL13, IL8, IL2, T-cell surface glycoprotein CD6 (CD6), DNER, TNFSF12, NKR2B4, VEGFA, fibroblast growth fac tor (FGF)5, CD40L receptor, MMP 1, C-C motif chemokine 23 (CCL23), TRAIL, monocyte chemoattractant protein (MCP)1, IL10RB, ADA, CXCL5, GDNF, and TNFβ levels. Conversely, OPG, MMP10, CCL4, IL15RA, IL18R1, MCP2, IL6, FGF21, Cystatin D, CSF1, FGF23, CXCL1, CXCL6, S100A12, FGF19, MCP1a, SULT1A1, IL7, TRANCE, FLT3LG, TGFα, MCP4, TNFSF14, EIF4EBP1, CUB domain-containing protein 1 (CDCP1), Oncostatin-M (OSM), MCP3, CCL19, IL4, SLAM, IL5, CD5, IL10 (OR: 0.27) were identi fied to be negatively correlated with the risk of AIH. The detailed outcomes of the IVW randomization method are presented in (Supplementary Table 2). The MR-Egger test results indicated the absence of heterogeneity in several SNPs (Supplementary Table 3). Reversal of causality was not observed in any of the analyses conducted using the MR Steiger’s test (Supplementary Table 3).
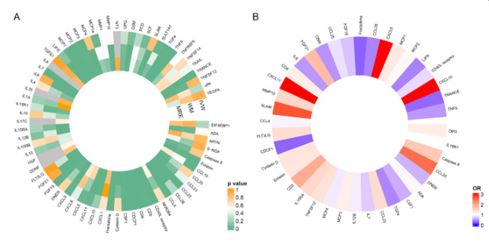
We analyzed the correlation between circulating inflammatory proteins and PBC development risk (Figure 3A). Outcomes with a P<0.05 for IVW randomization method outcomes were screened, and an OR was further used to express the association between exposure and outcome (Figure 3B). The results demonstrated a positive correlation between PBC risk and the levels of CXCL9 (OR: 6.90), CXCL10 (OR: 5.67), CXCL11, SLAM, CCL20, CD5, FGF21, Caspase 8, MMP10, IL15RA, CCL23, FLT3LG, TNFSF12, Cystatin D, Eotaxin, MCP1, CD6, MCP3, MCP2. Conversely, IL18R1, ADA, CCL4, IL12B, MCP4, CCL25, CD40L receptor, IL7, FGF19, DNER, CSF1, TNFβ, IL6, OSM, TGFα, CCL28, LIFR, TRANCE, CDCP1, Fractalkine (OR: 0.27) were identified to be negatively correlated with the PBC risk. The detailed outcomes of the IVW randomization method are presented in (Supplementary Table 4).
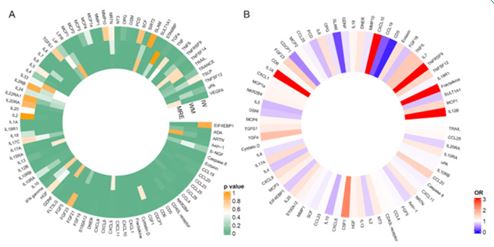
We also examined the association between circulating in flammatory proteins and susceptibility to PSC development (Fig ure 4). The results demonstrated a positive correlation between PSC risk and the levels of TNFRSF9 (OR: 45.16), Fractalkine (OR: 44.80), IL12B (OR: 20.53), CXCL10, IL1A, CSF1, TGFα, TNFβ, IL7, FGF23, CCL20, TNFSF12, MCP1, IL17A, Eotaxin, CXCL9, IL8, IL20, DNER, NRTN, IL10RA, TGFβ1, IL13, NT3, MCP3, NKR2B4, S100A12, HGF, MCP4, IL18, CXCL1, MCP1a, CD6, CCL28, MCP2, CD40L receptor, CCL23, Cystatin D, CCL4. Conversely, IL10RB, FGF5, CXCL6, MMP1, uPA, CXCL11, IL18R1, CCL25, Caspase 8, SCF, MMP10, OPG, GDNF, IL6, Axin-1, IL20RA, IL2, EIF4EBP1, OSM, IL4, SULT1A1, FGF19, PCD, IL5, IL10, CDCP1, CCL19, SLAM, and CD5 (OR: 0.05) were negatively correlated with PSC risk. The detailed outcomes of the IVW randomization method are presented in (Supplementary Table 5).
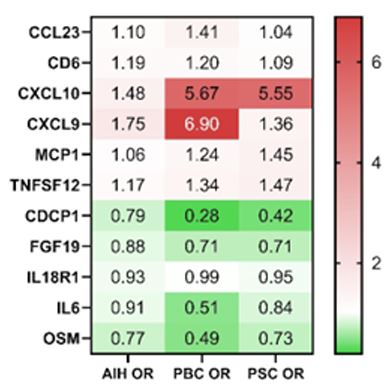
To comprehensively evaluate circulating inflammatory pro teins exhibiting common characteristics in AILDs, we screened for outcomes that were significant for both exposure and out comes using the IVW random method, ensuring consistency across all AILDs. Our findings indicated that CCL23, CD6, CXCL10, CXCL9, MCP1, and TNFSF12 were positively associated with the risk of AILDs, whereas CDCP1, FGF19, interleukin-18 receptor 1 (IL18R1), IL6, and OSM were identified as protective factors (Figure 5).
Discussion
This study represents the first MR investigation to explore potential predictive serum markers by examining the asso ciation between AILDs and circulating inflammatory proteins. Ninety-one circulating inflammatory proteins exhibited dis tinct associations with various AILDs. Screening for circulating inflammatory protein markers in different autoimmune livers was conducted. Moreover, overlapping syndromes between AIH, PBC, or PSC constitute the spectrum of autoimmune liver disease [24]. From our results, we concluded that CCL23, CD6, CXCL10, CXCL9, MCP1, and TNFSF12 were positively associated with the risk of AILDs, whereas CDCP1, FGF19, IL18R1, IL6, and OSM were identified as protective factors.
Macrophages are widely acknowledged as a prominent source of pro-inflammatory cytokines [25]. Th1, Th2, and TH17 cells, along with pro-inflammatory factors including IL2, IL17, IL22, IFN-γ, and TNF-α, have a crucial impact on the hepatic inflammation progression [26]. Regulatory T cells (Tregs) exert a protective role by secreting anti-inflammatory cytokines, in cluding IL10, to inhibit effector T cells (Teff) [27]. Consequently, circulating inflammatory proteins can activate inflammatory pathways, affect various inflammatory cells, and cause a com plex liver inflammatory response, eventually leading to liver tis sue damage and liver disease progression [28].
The macrophages are widely acknowledged as a prominent source of proinflammatory cytokines [25]. TNFSF12, a member of the TNF superfamily, regulates macrophages and induces liv er fibrosis and hepatocyte apoptosis, contributing to the occur rence and development of AIH [29]. Knockout of MCP1 in mice attenuates hepatic damage, indicating the crucial role of liver derived MCP1 in modulating macrophage activation and pro-in flammatory cytokine secretion [30]. A co-stimulatory receptor, CD6, stimulates monocyte antigen presentation and is involved in T-cell development [31]. The CD6 expression is restricted to Teff rather than Tregs, and the CD6/activated leukocyte cell ad hesion molecule pathway plays a crucial role in orchestrating immune processes associated with activation, differentiation, and migration of T cells [32].
CCL23/CCR1 governs the migration of monocytes, neutro phils, and T cells, whereas CXCL9/CXCR3 facilitates the recruit ment of Teff [33]. CXCL9 and CXCL10 play a pivotal role in the pathogenesis of numerous autoimmune and inflammatory disorders, exerting a potent effect on the recruitment and ac cumulation of Th1 cells, and are closely associated with the development of autoimmune liver disease [34,35]. The chemo kines CXCL9 and CXCL10 facilitate the differentiation of CD4+ T cells into effector Th1/Th17 cells [36]. The increase in TH17 cells may result in a concomitant decrease in the Tregs popula tion, leading to a significant elevation in the Tregs/TH17 ratio and compromised tolerance towards autoantigens, thereby contributing to the initiation and persistence of autoimmune liver injury [37]. The induction of chemokines CXCL10 by IFN-γ is closely associated with liver fibrosis. Therefore, mice with ge netic defects in CXCL10 exhibit less hepatic fibrosis induced by CCl4 than wild-type mice [38,39]. Animal experiments also con firmed that the activation of cytokine-induced TH1 and TH17 cells induces the upregulation of CXCL9 and CXCL10 in the liver, thereby facilitating the AIH progression in mice [14]. Therefore, CXCL10, in combination with CXCL9, exhibited a strong potential to identify patients with advanced liver fibrosis [40].
Cytokine IL6 is widely recognized as a pivotal pro-inflam matory and profibrotic factor that drives the progression of liver fibrosis [41]. However, in this study, the opposite results were obtained. The findings demonstrate that IL6 functions in a protective capacity in AILDs. Moreover, emerging evidence suggests that IL6 not only serves as a stimulator of pro-inflam matory cytokines and the acute phase response but also plays a crucial role in liver protection and regeneration. This is sup ported by observations that IL6 knockout mice display compro mised liver regeneration, and inhibition of the IL6 pathway ex acerbates liver injury [42]. Furthermore, the activation of Signal Transducer and Activator of Transcription 3 (STAT3) through IL6 signaling plays a crucial role in glycoprotein 130 (gp130)-medi ated hepatoprotection in the injured liver [43]. A member of the gp130 cytokine family, OSM, exhibits structural and func tional similarities to the IL-6 cytokine family [44]. Therefore, the study revealed that OSM possesses a similar impact on liver function as IL6.
Moreover, IL10 exerts inhibitory effects on macrophages and dendritic cells, leading to the suppression of CD4+ T cell activa tion and cytokine secretion, along with the facilitation of Treg proliferation and immune regulation [45]. Consequently, IL10 plays a pivotal role in dampening the inflammatory response in liver injury while also contributing to the promotion of autoim mune tolerance and mitigation of liver fibrosis [46]. However, in this study, IL10 exhibited a significant protective effect in AIH and PSC but not in PBC. The inhibitory effects of IL4 and IL10 on inflammation are similar, and increasing their levels can effec tively delay the progression of liver fibrosis [47]. A protective ef fect of IL4 was identified in this study for AIH (OR: 0.68, P<0.01) and PSC (OR: 0.72, P<0.01) but not for PBC (OR: 0.61, P=0.08).
An intestinal hormone, FGF19, reduces bile acid synthesis in the liver by activating the hepatic fibroblast growth factor re ceptor 4 [48]. In multidrug resistance protein (MDR2)-deficient mice, increased FGF19 expression reduced liver inflammation, alleviated biliary fibrosis, and reversed liver injury [49]. A con trary view has also been reported: in PBC-AIH OS patients with severe cholestasis and a high degree of severity, serum FGF19 levels increase proportionally [50]. The FGF19 augmented se cretion under these circumstances is regarded as a defensive, negative feedback mechanism aimed at safeguarding hepato cytes against the cytotoxic effects of bile acids [51]. The findings of our study also demonstrated that elevated concentrations of FGF19 significantly reduced susceptibility to AILDs.
This is the first study to investigate the causal relationship between circulating inflammatory proteins and AILDs using pooled GWAS-level statistics. By aggregating substantial genetic data, this study minimized the possible confounding and reverse causality. However, this study has some limitations. The first step was to use independent SNPs (P<5×10-5) that reached a ge nome-wide significance level to prevent weak IVs from reducing the validity of the MR study. Moreover, certain SNPs genotypes did not exhibit significant associations with disease outcomes, resulting in missing data points and a potential selection bias in the choice of markers common to AILDs. Notably, the find ings of this study may not be generalizable to all populations, as the research only focused on individuals of European descent. Therefore, the conclusions drawn should be made carefully.
Conclusion
In this study, we employed a large-scale sample for exposure and outcome GWAS to conduct MR analysis, aiming to infer causal relationships between circulating inflammatory proteins and AILDs. Our findings revealed distinct associations between various circulating inflammation markers and AILDs. CXCL10, in combination with CXCL9, exhibited a strong potential to predict patients with AILDs. However, the relevance of IL6 as a risk fac tor for AILDs remains controversial.
Declarations
Ethics approval and consent to participate
• As per the regulations outlined in People’s Republic of China’s “Notice on the Implementation of Ethical Review Measures for Life Science and Medical Research”, our study falls under the exemption criteria specified in Section 4 of the regulation. Therefore, ethics approval was not required for this research, as it met the following conditions:
• Exemption premise: This study used only publicly available data, especially summary level data from GWAS, did not involve sensitive personal information, did not cause harm to individuals, and did not compromise their privacy.
• Exemption provision: Our research adheres to the exemption circumstances outlined in Section 4 of the regulation: We utilized lawfully obtained publicly available data for our analysis. The data used in this study were fully anonymized, ensuring the privacy and confidentiality of individuals. Our research focuses on analyzing existing data and does not involve interventions, human biological samples, or activities related to reproductive cloning, genetic manipulation, or germ cells.
• Due to the nature of our study and its compliance with the exemption criteria, we did not require explicit ethics approval. And we affirm that this research was conducted in accordance with the applicable laws, regulations, and ethical standards.
Competing interests: The authors declare no competing interests associated with the manuscript.
Funding: No funding.
Acknowledgment: We thank Home for Researchers editorial team (www.home-for-researchers.com) for language editing service.
References
- Gerussi A, et al. Artificial intelligence for precision medicine in autoimmune liver disease. Front Immunol. 2022; 13: 966329.
- Yang L, et al. Shear wave-based sound touch elastography in liver fibrosis assessment for patients with autoimmune liver diseases. Quant Imaging Med Surg. 2021; 11: 1532–42.
- Trivedi PJ, Hirschfield GM. Recent advances in clinical practice: epidemiology of autoimmune liver diseases. Gut. 2021; 70: 1989–2003.
- Terziroli Beretta-Piccoli B, Mieli-Vergani G, Vergani D. Autoimmune hepatitis: serum autoantibodies in clinical practice. Clin Rev Allergy Immunol. 2022; 63: 124–37.
- Wang Y, et al. The enlargement of abdominal lymph nodes is a characteristic of autoimmune liver disease. Mediators Inflamm. 2020; 2020: 3631625.
- Wang Y, et al. Predicting liver disease risk using a combination of common clinical markers: a screening model from routine health check-up. Dis Markers. 2020; 2020: 8460883.
- Peng XG, et al. Evolution of correlation between Helicobacter pylori infection and autoimmune liver disease. Exp Ther Med. 2017; 14: 1487–90.
- Moreira RK, et al. Diagnostic utility of IgG and IgM immunohistochemistry in autoimmune liver disease. World J Gastroenterol. 2010; 16: 453–7.
- Fernández MIC, et al. Diagnosis and treatment of autoimmune liver diseases in a tertiary referral center in Cuba. Curr Ther Res Clin Exp. 2017; 85: 8–14.
- Sirbe C, et al. Pathogenesis of autoimmune hepatitis: cellular and molecular mechanisms. Int J Mol Sci. 2021; 22: 1–20.
- Doherty DG. Immunity, tolerance and autoimmunity in the liver: a comprehensive review. J Autoimmun. 2016; 66: 60–75.
- Xu YF, et al. The proinflammatory cytokines IL-18, IL-21 and IFN-γ differentially regulate liver inflammation and anti-mitochondrial antibody level in a murine model of primary biliary cholangitis. J Immunol Res. 2022; 2022: 7111445.
- Huang YH, et al. Hydrodynamics-based transfection of rat interleukin-10 gene attenuates porcine serum-induced liver fibrosis in rats by inhibiting the activation of hepatic stellate cells. Int J Mol Med. 2014; 34: 677–86.
- Ikeda A, et al. Progression of autoimmune hepatitis is mediated by IL-18-producing dendritic cells and hepatic CXCL9 expression in mice. Hepatology. 2014; 60: 224–36.
- Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary and checklist for clinicians. BMJ. 2018; 362: k601.
- Smith GD, et al. Clustered environments and randomized genes: a fundamental distinction between conventional and genetic epidemiology. PLoS Med. 2007; 4: e352.
- Pingault JB, et al. Using genetic data to strengthen causal inference in observational research. Nat Rev Genet. 2018; 19: 566–80.
- Zhao JH, et al. Genetics of circulating inflammatory proteins identifies drivers of immune-mediated disease risk and therapeutic targets. Nat Immunol. 2023; 24: 1540–51.
- Sakaue S, et al. A cross-population atlas of genetic associations for 220 human phenotypes. Nat Genet. 2021; 53: 1415–24.
- Liu JZ, et al. Dense fine-mapping study identifies new susceptibility loci for primary biliary cirrhosis. Nat Genet. 2012; 44: 1137–41.
- Ji SG, et al. Genome-wide association study of primary sclerosing cholangitis identifies new risk loci and quantifies the genetic relationship with inflammatory bowel disease. Nat Genet. 2017; 49: 269–73.
- Hemani G, Bowden J, Davey Smith G. Evaluating the potential role of pleiotropy in Mendelian randomization studies. Hum Mol Genet. 2018; 27: R195–208.
- Zhu Z, et al. Integration of summary data from GWAS and eQTL studies predicts complex trait gene targets. Nat Genet. 2016; 48: 481–7.
- Invernizzi F, et al. Gender and autoimmune liver diseases: relevant aspects in clinical practice. J Pers Med. 2022; 12: 1–15.
- Coukos A, et al. Systematic comparison with autoimmune liver disease identifies specific histological features of immune checkpoint inhibitor-related adverse events. J Immunother Cancer. 2022; 10: e005321.
- Ferri S, et al. A multifaceted imbalance of T cells with regulatory function characterizes type 1 autoimmune hepatitis. Hepatology. 2010; 52: 999–1007.
- Jeffery HC, et al. Clinical potential of regulatory T cell therapy in liver diseases: an overview and current perspectives. Front Immunol. 2016; 7: 334.
- Radmanić L, et al. The effect of treatment-induced viral eradication on cytokine and growth factor expression in chronic hepatitis C. Viruses. 2022; 14: 1–17.
- Zhang Y, et al. Moscatilin suppresses the inflammation from macrophages and T cells. Open Med (Wars). 2022; 17: 756–67.
- Gao X, et al. Role of donor and host cells in muscle-derived stem cell-mediated bone repair: differentiation vs paracrine effects. FASEB J. 2014; 28: 3792–809.
- Dye CK, et al. Shifts in the immunoepigenomic landscape of monocytes in response to a diabetes-specific social support intervention. Clin Epigenetics. 2022; 14: 91.
- Chalmers SA, et al. The CD6/ALCAM pathway promotes lupus nephritis via T cell-mediated responses. J Clin Invest. 2022; 132: e154489.
- Di L, et al. SNAP25 is a potential prognostic biomarker for prostate cancer. Cancer Cell Int. 2022; 22: 144.
- Tulic MK, et al. Innate lymphocyte-induced CXCR3B-mediated melanocyte apoptosis is a potential initiator of T-cell autoreactivity in vitiligo. Nat Commun. 2019; 10: 2178.
- Jones DEJ, et al. The relationship between disease activity and UDCA response criteria in primary biliary cholangitis: a cohort study. EBioMedicine. 2022; 80: 104068.
- Marques A, et al. Transcriptome assessment of erythema migrans skin lesions in patients with early Lyme disease reveals predominant interferon signaling. J Infect Dis. 2017; 217: 158–67.
- Wang H, et al. The JAK inhibitor tofacitinib ameliorates immune-mediated liver injury in mice. Mol Med Rep. 2019; 20: 4883–92.
- Nagayama K, et al. Overexpression of interferon gamma inducible protein 10 in the liver of patients with type I autoimmune hepatitis. Am J Gastroenterol. 2001; 96: 2211–7.
- Wang C, Sun Y. Induction of collagen I by CXCL10 in ovarian theca stroma cells via the JNK pathway. Front Endocrinol (Lausanne). 2022; 13: 823740.
- Zeremski M, et al. CXCL9 and CXCL10 chemokines as predictors of liver fibrosis in chronic hepatitis C. J Infect Dis. 2011; 204: 832–6.
- Bai YM, et al. Single-cell transcriptomic dissection of triclosan-induced liver fibrosis in mice. Mil Med Res. 2023; 10: 7.
- Knecht S, Eberl HC, Bantscheff M. Interval-based secretomics unravels acute-phase response in hepatocyte model systems. Mol Cell Proteomics. 2022; 21: 100241.
- Dong J, et al. Hepatocyte-specific gp130 signalling underlies APAP-induced liver injury. Int J Mol Sci. 2022; 23: 1–15.
- van Krieken PP, et al. Oncostatin M promotes lipolysis in white adipocytes. Adipocyte. 2022; 11: 315–24.
- Murai M, et al. Interleukin-10 acts on regulatory T cells to maintain Foxp3 expression and suppressive function in mice with colitis. Nat Immunol. 2009; 10: 1178–84.
- Yang ZF, et al. Induction of long-term liver allograft survival by delayed immunosuppression is dependent on interleukin-10. Liver Transpl. 2007; 13: 571–8.
- Gan Y, et al. Anti-obesity effect of Lactobacillus plantarum CQPC01 by modulating lipid metabolism in high-fat diet-induced mice. J Food Biochem. 2020; 44: e13491.
- Yao Y, et al. Cholecystectomy promotes colon carcinogenesis by activating the Wnt signaling pathway via increased deoxycholic acid levels. Cell Commun Signal. 2022; 20: 71.
- Zhou M, et al. Engineered fibroblast growth factor 19 reduces liver injury and resolves sclerosing cholangitis in Mdr2-deficient mice. Hepatology. 2016; 63: 914–29.
- Li Z, et al. Dysregulation of circulating FGF19 and bile acids in primary biliary cholangitis–autoimmune hepatitis overlap syndrome. Biomed Res Int. 2020; 2020: 1934541.
- Mohamed GA, et al. Assessment of fibroblast growth factor 19 as a non-invasive serum marker for hepatocellular carcinoma. World J Hepatol. 2022; 14: 623–33.