
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 6
Spontaneous pneumomediastinum secondary to hyperemesis gravidarum: A case report of management and narrative review of literature
Yanan Wang1#; Shenghua Zhang1#; Shenghong Xu1; Ru Zhao2; Yurong Song1*
1Department of Obstetrics and Gynecology, The Second Affiliated Hospital of Anhui Medical University, China.
2Department of Radiology, The Second Affiliated Hospital of Anhui Medical University, China.
#These authors have been contributed to this article.
*Corresponding Author : Yurong Song
Department of Obstetrics and Gynecology, No. 678,
Furong Road, Economic Development Zone, Hefei City,
Anhui Province, China.
Email: efy102404@fy.ahmu.edu.cn
Received : Dec 04, 2025
Accepted : Jan 19, 2026
Published : Jan 26, 2026
Archived : www.jjgastro.com
Copyright : © Song Y (2026).
Abstract
Third-trimester Hyperemesis Gravidarum (HG) induced Spontaneous Pneumomediastinum (SPM) is extremely rare, with occult symptoms. Progressive deterioration may threaten maternal and fetal safety. Comprehensive imaging, timely identification, and diagnosis are crucial, necessitating this case report to enhance clinical awareness. This case report describes a 32-year-old Chinese woman with persistent HG who developed acute facial swelling and severe abdominal pain at GA 34+4, with no history of digestive and respiratory system disease. A computed tomography examination of the chest confirmed extensive air be found beneath the skin of the anterior chest, within the mediastinum and even within the spinal canal. Then, a diagnosis of SPM was made based on these findings. Considering the critical condition of worsening vomiting and abdominal pain, a surgical termination of pregnancy was performed after completing the administration of Dexamethasone to promote fetal lung maturity. Subsequently, conservative management was given, multiple computed tomography examinations indicated that the emphysema was gradually resolving and disappearing, the final outcome for both the mother and the fetus was favorable. This case given an awareness and inform diagnostic & management strategies for SPM secondary to HG. It’s important that clinician should keep in mind in pregnant patients with persistent HG.
Keywords: Late pregnancy; Spontaneous pneumomediastinum (SPM); Hyperemesis gravidarum (HG); Clinical management.
Citation: Wang Y, Zhang S, Xu S, Zhao R, Song Y. Spontaneous pneumomediastinum secondary to hyperemesis gravidarum: A case report of management and narrative review of literature. J Gastroenterol Res Pract. 2026; 6(1): 1244.
Introduction
Spontaneous Pneumomediastinum (SPM)—idiopathic air accumulation in the mediastinum—is extremely rare in preg nancy (incidence< 1/100,000), caused by sudden intrathoracic pressure surges that rupture alveoli, with air dissecting into the mediastinum and potentially progressing to subcutaneous em physema [1,2]. Hyperemesis Gravidarum (HG), a severe preg nancy-associated nausea and vomiting disorder characterized by intractable vomiting, weight loss, electrolyte disturbances, and ketosis, predominantly affects the first trimester with spon taneous resolution by 16-20 weeks of gestation. However, rare cases may persist or recur into the third trimester, often associ ated with multiple pregnancies, molar gestation, or unresolved metabolic abnormalities, conferring increased maternal and fetal risks [3,4]. Third-trimester HG-induced SPM is particularly rare: advanced gestation amplifies physiological stress and in tra-abdominal pressure, worsening vomiting-related intratho racic pressure surges, while SPM’s symptoms (i.e. chest pain, dyspnea, subcutaneous emphysema) may be masked by preg nancy discomforts, leading to delayed diagnosis [5,6]. This case report aims to boost clinical awareness and inform diagnostic & management strategies for this rare disease.
Case presentation
Patient information
A 32-year-old Chinese woman, gravida 6, para 1, abortus 4, at 34 weeks and 4 days of pregnancy (i.e. Gestational Age [GA] 33+4). Pre-pregnancy weight and Body Mass Index (BMI) were 67.0 kg and 26.8 kg/m2, respectively. On current presentation, the patient’s weight and BMI had decreased to 56.8 kg and 22.7 kg/m2.
This patient had no remarkable medical history and was in good health prior to the current presentation, with no record of gastrointestinal or respiratory diseases. She underwent regular prenatal examinations throughout her pregnancy. In the first trimester, she completed routine blood tests and fetal ultraso nography, with essentially normal results. Serial monitoring of maternal vital signs (including blood pressure) and fetal growth parameters revealed no significant abnormalities. She denied a history of viral infections, exposure to contaminated water from endemic areas, as well as prior use of alcohol, tobacco, or illicit substances.
Clinical findings
Since the 12th week of pregnancy, this patient has repeat edly sought treatment at local clinics and our hospital due to HG for 5 times (GA 12+5, GA 14+5, GA 18+2, GA 24+2, GA 34+4). The primary therapeutic interventions consisted of symptom atic relief and fluid replacement, which were categorized as supportive care. Clinical symptoms ameliorated following each treatment, but then quickly recur after discharge. Starting from GA 18+2, the patient’s urine routine test indicated that the urine protein remained at “++~+++”, proteinuria (1614 mg/24 h), while the blood pressure tests were always within the nor mal range during this gestation. Due to the relatively conserva tive examination methods during pregnancy, the specific cause of the urine protein has not been clearly identified for the time being.
Three days prior to the current hospitalization (GA 34+1), the patient presented with recurrent nausea, vomiting, and upper abdominal pain. Upon admission, she received symptomatic and supportive interventions, including nil per os, antiemetic therapy, gastric mucosal protection, antispasmodic treatment, and intravenous fluid replacement. Approximately 30 min after admission (GA 34+4), the patient developed facial and cervical swelling accompanied by intractable upper abdominal pain. Nevertheless, vital signs were stable: blood pressure 110/90 mmHg, oxygen saturation 97% on room air, respiratory rate 19 breaths per minute, and afebrile. No cyanosis or calf swelling was noted. Physical examination revealed subcutaneous em physema palpable over the clavicular regions, neck, and ante rior thoracic wall, with bilateral symmetric and adequate air entry on lung auscultation.
Diagnostic assessment
An urgent chest X-ray, Electrocardiograph (ECG) and ultra sound examinations (assessing the liver, gallbladder, pancreas, spleen, and urinary system) were requested as well as an ur gent review by the medical support from the departments of Gastrointestinal and Thoracic Surgery on call for the evening. The chest X-ray (Figure 1A) demonstrated clear lung paren chyma without evidence of gastrointestinal tract perforation or other obvious abnormalities. The ECG revealed a regular sinus rhythm. Abdominal ultrasound and laboratory investigations, including measurements of creatine kinase, coagulation pro files, serum amylase, and lactic dehydrogenase, yielded essen tially normal results. Based on these findings, cardiac-related pathologies and gastrointestinal perforation were preliminar ily excluded. However, following a multidisciplinary discussion with the on-call medical team, the clinical manifestations and preliminary results were insufficient to rule out the possibility of SPM. Subsequent to obtaining informed consent from the patient, urgent Computed Tomography (CT) was performed, which confirmed extensive subcutaneous emphysema, pneu momediastinum, and intraspinal emphysema (Figure 1B-C). Key laboratory results are presented in (Table 1).
Clinical intervention
Twelve hours later, the patient continued to experience se vere upper abdominal pain, with no resolution of facial swell ing. After a multidisciplinary consultation and comprehensive deliberation, a diagnosis of acute SPM was confirmed, which was attributed to the patient’s history of prolonged and recur rent HG. Expectant management was deemed to carry a high risk, as it might predispose the patient to maternal respiratory and circulatory disturbances; in the event of disease progres sion, the lives of both the mother and fetus could be endan gered. Following thorough communication with the patient and her family regarding the clinical prognosis, potential risks, and alternative management strategies, surgical termination of pregnancy was proposed as the recommended intervention.
After obtaining informed consent from the patient and her family, the patient underwent a lower uterine segment cesar ean section, with successful delivery of a live male infant (Birth weight: 1980 g; Apgar scores: 9 at 1 min, 10 at 5 min, 10 at 10 min). Neonatology consultation was conducted intraoperative ly, and the infant was transferred to the pediatrics department. Given the patient’s critical condition, postoperative manage ment included NPO, intravenous fluid replacement, antibiotics for anti-infection, and low-molecular-weight heparin sodium for anticoagulation (Postoperative VTE score: 3 points, High risk).
Follow-up and outcomes
The patient had a favorable postoperative recovery, with a significant improvement in subjective facial swelling. A follow up chest CT scan on postoperative day 4 showed a marked re duction in multiple subcutaneous emphysema of the anterior chest wall and mediastinal emphysema compared with four days prior, and the patient was instructed to gradually resume oral intake. Postoperative laboratory results revealed protein uria (459.84 mg/24h) and hemoglobin (102 g/L), while other indicators were unremarkable. The patient was discharged on postoperative day 7.
After discharge, the patient recovered well. A follow-up CT scan performed 2 weeks post-discharge showed that the em physema had completely resolved (Figure 1B-C). The newborn exhibited normal development in all indicators after discharge, and both the mother and infant achieved a favorable pregnancy outcome. At this point, the life-threatening condition was al leviated. However, the challenges for the patient persist. During a recent telephone follow-up, the patient reported persistent strongly positive urine protein at “++~+++”, and the renal bi opsy results indicated IgG nephropathy, marking the onset of another long-lerm journey for the patient.
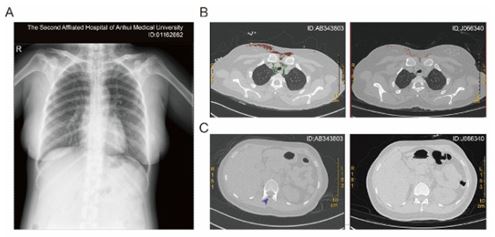
Table 1: Key laboratory results.
| K+ | 4.26 | 3.50-5.30 mmol/L |
| Na+ | 137.9 | 137.0-147.0 mmol/L |
| Cl- | 102.5 | 99.0-110.0 mmol/L |
| Creatine Kinase MB isoenzyme | 19 | 0-24 U/L |
| Lactate Dehydrogenase | 193 | 120-250 U/L |
| Amylase | 53 | 35-135 U/L |
| Creatine Kinase | 212↑ | 40-200 U/L |
| D-Dimer | 1.17↑ | 0.00-0.55 μg/mL |
| C-reactive Protein | 6.8↑ | 0.0-6.0 mg/L |
| White Blood Cell | 10.57↑ | 3.50-9.50×109/L |
| Hemoglobin | 123 | 115-150 g/L |
| Platelet | 241 | 125-350×109/L |
| Total Bile Acid | 0.4 | 0.0-15.0 μmol/L |
Discussion
SPM refers to the accumulation of free air in the mediasti nal cavity without definite traumatic or iatrogenic causes. Chest pain and tightness, dyspnea, and neck tightness are the most common symptoms. Some patients may also have subcutane ous emphysema, which can spread to the face and trunk in severe cases. As a rare clinical condition, SPM is also known as Hamman’s Syndrome when associated with pregnancy and puerperium [7,8]. The earliest reported case was discovered in 1949 by D J MacRAE [9]. Since its symptoms such as chest pain and dyspnea are similar to those of life-threatening con ditions like cardiopathy, pulmonary embolism and aortic dis section, misdiagnosis is likely [10]. SPM in pregnancy has been described in around 200 cases, most of these cases occurred during the second stage of labor, while very few occurred in the third trimester of pregnancy [11,12].
Pregnancy-induced physiological changes increase the risk of SPM. The gradual enlargement of the uterus in the middle and late pregnancy elevates the diaphragm, compressing the thoracic cavity and changing the anatomical structure of the thoracic organs [13]. Very rarely, in this case, the patient had persistent nausea and vomiting from the early to late pregnancy stage. The principle is actually similar to the irregular Valsalva movements [2]. This patient has undergone 6 pregnancies and 4 induced abortions. Although there was no history of vomiting in the previous pregnancies, the history of multiple pregnancies might be one of the reasons for the persistent HG this time [14]. While, SPM due to HG is not common.
Imaging examination is the key to diagnosis. Chest X-ray (posteroanterior and lateral views) is the most commonly used primary examination method, which can clearly show the air shadow in the mediastinal area. For cases with unclear X-ray results, chest CT can more accurately determine the scope of mediastinal air accumulation and rule out other dangerous conditions such as esophageal rupture and pneumothorax. It should be noted that when diagnosing, it is necessary to distin guish SPM from myocardial infarction and pulmonary embolism through electrocardiogram and blood gas analysis to avoid de laying the treatment of critical diseases [15]. Of course, if real time monitoring of oxygen saturation shows poor results, im mediate blood gas analysis is necessary [16]. Here in this case, the relevant laboratory tests showed basically normal (creatine kinase, coagulation profiles, serum amylase, and lactic dehydro genase), which was a favorable sign for her.
Pregnancy-associated SPM is generally a benign self-limiting disease, and conservative treatment is the mainstream plan [1]. The specific measures include bed rest, oxygen inhalation, and close monitoring of vital signs. For patients with secondary in fection risk, broad-spectrum antibiotics can be used appropri ately, however most of them do not require antibiotic use [17]. Most patients can absorb the mediastinal air spontaneously within 1-2 weeks, and the prognosis is good. Surgical treatment is only applicable to extremely rare severe cases [1]. In this case, the patient was in the third trimester of pregnancy (GA 34+4). Given the progressive aggravation of her emphysema, continu ing expectant management would offer no benefit. Therefore, emergency cesarean section was performed to terminate the pregnancy, followed by conservative treatment for the patient herself, resulting in a favorable maternal and fetal outcome. Follow-up studies have shown that pregnancy associated SPM has no long-term adverse effects on maternal health and subse quent fertility, and recurrence is rare.
Delayed recognition of SPM in pregnant women with HG can result in life-threatening complications, including tension pneumomediastinum, pneumothorax, and mediastinitis, which endanger both maternal and fetal lives. Despite its rarity, the as sociation between HG, especially third-trimester HG, and SPM highlights the need for heightened clinical awareness among obstetricians, pulmonologists, and emergency physicians. Early diagnosis via chest CT or chest X-ray, combined with prompt con servative management or surgical intervention in severe cases, is crucial to improving maternal and fetal outcomes. Given the limited literature on third-trimester HG-induced SPM, further research is warranted to elucidate its clinical characteristics, op timal diagnostic strategies, and management protocols.
Declarations
Author contribution: All authors have made substantial contributions to the work: All the authors collected clinical data; Yanan Wang and Shenghua Zhang drafted the manuscript; Ru Zhao reviewed imaging findings; Yurong Zhao revised the manuscript critically for important intellectual content, and all authors have read and approved the final version of the manuscript.
Funding information: This study was not funded.
Conflict of interest statement: All authors have completed the unified competing interest form (available on request from the corresponding author). There was no support from any organization for the submitted work. The authors have no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
References
- Amine NO, et al. Pregnancy-associated spontaneous pneumomediastinum: a contemporary review. Cureus. 2018; 10: e3452.
- Scala R, et al. Spontaneous pneumomediastinum in pregnancy: a case report. Rev Port Pneumol (2006). 2016; 22: 129–31.
- Lee NM, Saha S. Nausea and vomiting of pregnancy. Gastroenterol Clin North Am. 2011; 40: 309–34.
- Florentin M, et al. Hyperemesis gravidarum: a benign condition of pregnancy or a challenging metabolic disorder? Eur J Case Rep Intern Med. 2020; 7: 001979.
- Zonnebeld N, et al. Pneumomediastinum in late pregnancy: a case report and review of the literature. Acta Chir Belg. 2023; 123: 301–4.
- Scarborough A, Kemp O, Scarborough O. Spontaneous pneumomediastinum secondary to hyperemesis gravidarum: a case report and principles of recognition and management. Case Rep Womens Health. 2020; 28: e00257.
- Mohamed W, et al. Spontaneous pneumomediastinum (Hamman’s syndrome): presenting as acute severe asthma. J R Coll Physicians Edinb. 2019; 49: 31–3.
- Grapatsas K, et al. Hamman’s syndrome (spontaneous pneumomediastinum presenting as subcutaneous emphysema): a rare case of the emergency department and review of the literature. Respir Med Case Rep. 2018; 23: 63–5.
- Mac RD. Spontaneous pneumomediastinum in pregnancy. Lancet. 1949; 1: 902–4.
- Bakhos CT, et al. Spontaneous pneumomediastinum: an extensive workup is not required. J Am Coll Surg. 2014; 219: 713–7.
- Oshovskyy V, Poliakova Y. A rare case of spontaneous pneumothorax, pneumomediastinum and subcutaneous emphysema in the second stage of labour. Int J Surg Case Rep. 2020; 70: 130–2.
- Berdai MA, et al. Spontaneous pneumomediastinum in labor. Case Rep Obstet Gynecol. 2017; 2017: 6235076.
- Costantine MM. Physiologic and pharmacokinetic changes in pregnancy. Front Pharmacol. 2014; 5: 65.
- Pont S, et al. Risk factors and recurrence of hyperemesis gravidarum: a population-based record linkage cohort study. Acta Obstet Gynecol Scand. 2024; 103: 2392–400.
- Petrov D, Goranov E. Spontaneous pneumomediastinum: clinic, diagnostics and treatment. Khirurgiia (Sofiia). 2008; 3: 14–7.
- Abid N, et al. Spontaneous pneumomediastinum in patients with COVID-19 pneumonia. Tunis Med. 2023; 101: 313–6.
- Ebina M, et al. Management of spontaneous pneumomediastinum: are hospitalization and prophylactic antibiotics needed? Am J Emerg Med. 2017; 35: 1150–3.