
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 6
Vitamin B12 deficiency in adults and elderly patients: The imperative of distinguishing maldigestion from true malabsorption for precision therapy
Emmanuel Andrès, MD, PhD1*; Jean-Edouard Terrade, MD1; Xavier Jannot, MD1; Thomas Vogel, MD, PhD2; Noel Lorenzo Villalba, MD1
1Departments of Internal Medicine, University Hospitals of Strasbourg, France.
2Geriatrics, Hautepierre Hospital, University Hospitals of Strasbourg, France.
*Corresponding Author : Emmanuel Andrès
Departments of Internal Medicine, University Hospitals
of Strasbourg, 67000 Strasbourg, France.
Email: emmanuel.andres@chru-strasbourg.fr
Received : Nov 17, 2025
Accepted : Jan 02, 2026
Published : Jan 09, 2026
Archived : www.jjgastro.com
Copyright : © Andrès E (2026).
Abstract
Vitamin B12 (cobalamin) deficiency is a common but often underdiagnosed condition, particularly among older adults and patients with gastrointestinal disorders. Absorption of dietary cobalamin requires a complex sequence of gastric, pancreatic, and ileal processes. Disruption at any stage results in maldigestion or malabsorption, with hematologic and neurologic consequences. Biochemical deficiency prevalence ranges from 5–15% in community dwelling older adults to 20–40% in institutionalized populations. Maldigestion of dietary cobalamins accounts for up to 60–70% of vitamin B12 deficiency in adults, often due to age-related gastric atrophy, H. pylori infection, long-term proton-pump inhibitor use, metformin therapy, or small intestinal bacterial overgrowth. Malabsorption arises in pernicious anemia and ileal resections, Crohn’s disease, celiac disease, and congenital transport defects. High-dose oral crystalline cobalamin (≥1000 μg/day) is effective in most FCM cases, while parenteral therapy is indicated for severe neurologic involvement or often in case of severe malabsorption. Early recognition prevents irreversible complications. Identification of at-risk populations and mechanistic understanding enable targeted diagnosis, individualized therapy, and prevention of long-term morbidity.
Keywords: Vitamin B12; Cobalamin; Malabsorption; Maldigestion; Food-cobalamin malabsorption; Pernicious anemia; Biermer’s disease; Gastric atrophy; Crohn’s disease; Celiac disease; Metformin; Proton pump inhibitors; Surgery; Helicobacter pylori
Citation: Andres E, Terrade JE, Jannot X, Vogel T, Villalba NL. Vitamin B12 deficiency in adults and elderly patients: The imperative of distinguishing maldigestion from true malabsorption for precision therapy. J Gastroenterol Res Pract. 2026; 6(1): 1242.
Introduction
Vitamin B12 (cobalamin) is an essential water-soluble vita min required for DNA synthesis, erythropoiesis, and the main tenance of nervous system integrity. Its absorption is a complex, multistep process involving gastric acid-mediated release, sub sequent binding to Intrinsic Factor (IF), and active ileal uptake via the cubam receptor [1]. Deficiency results in severe clinical sequelae, including megaloblastic anemia, peripheral neuropa thy, and potentially irreversible cognitive impairment. Epidemi ological studies estimate prevalence rates ranging from 5–15% in community-dwelling adults over 60, rising significantly in institutionalized populations [2], underscoring its major public health impact. Two principal mechanisms underlie this defi ciency: (1) malabsorption of food- or protein-bound cobalamin (related to impaired digestion and release from dietary pro teins) and (2) malabsorption of free cobalamin (representing true defects at the IF or ileal receptor stages) [3]. Understand ing these distinct mechanisms is crucial for accurate diagnosis, appropriate biomarker interpretation, and targeted therapeutic strategies.
The objective of this narrative review is to synthesize cur rent evidence regarding the pathophysiology and clinical im plications of these two mechanisms of B12 deficiency, with a particular focus on diagnosis and management in older adults.
Pathophysiology of cobalamin absorption and deficiency
Dietary cobalamin is protein-bound, requiring a series of tightly regulated steps for efficient assimilation [1] (Figure 1). In the stomach, HCl and pepsin release the vitamin, which imme diately binds to haptocorrin (R-protein), forming a stable com plex resistant to gastric proteolysis [1]. In the duodenum, pan creatic proteases degrade haptocorrin, enabling cobalamin to bind Intrinsic Factor (IF), secreted by gastric parietal cells. The stable cobalamin–IF complex ensures safe passage to the termi nal ileum where the cubam receptor complex (cubilin and amni onless) facilitates receptor-mediated endocytosis [1]. Once ab sorbed, cobalamin enters the circulation, predominantly bound to Transcobalamin II (TCII), which delivers it to tissues; the liver stores 2–5 mg, sufficient for several years [4]. Disruption at any point—whether impaired gastric acid secretion, reduced IF pro duction, or dysfunctional ileal receptor uptake—can result in deficiency [1]. Intracellularly, B12 is converted into the active coenzyme forms, methylcobalamin and adenosylcobalamin, es sential for DNA synthesis and myelin maintenance [4]. Impair ments in cellular utilization pathways can result in functional B12 deficiency despite normal serum levels, emphasizing the crucial role of intracellular metabolism [4].
Pathophysiology: Maldigestion versus true malabsorption
Cobalamin deficiency in adults and in elderly patients and at risk populations primarily arises from two distinct pathophysi ological mechanisms: maldigestion and true malabsorption [3] (Figure 1). Maldigestion refers to the impaired release of food- or protein-bound cobalamin, known as Food-Cobalamin Malabsorption (FCM), a process dependent on gastric acidity and pepsin activity. Patients with FCM cannot extract cobalamin from food sources but can efficiently absorb crystalline forms of the vitamin. In contrast, true malabsorption of free cobala min occurs when IF-dependent uptake in the ileum is impaired. Historically, the Schilling test was essential for this differentia tion: in FCM, the standard test (free cobalamin) was normal, but the modified test (food-bound cobalamin) was abnormal; conversely, in true malabsorption, both tests were abnormal [3]. Understanding this distinction is crucial for accurate diag nosis and therapy, as patients with FCM typically respond to high-dose oral or sublingual supplementation, whereas those with IF deficiency or ileal pathology usually require parenteral replacement to achieve adequate repletion (Table 1) [2].
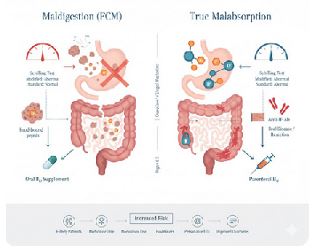
The figure illustrates the two primary pathophysiological pathways leading to B12 deficiency: Maldigestion (food-cobalamin malabsorption, FCM) (left panel) and True Malabsorption (right panel). Maldigestion (FCM): Impaired gastric function (due to hypochlorhydria or PPI/metformin use, often associated with atrophic gastritis) prevents the release of food-bound cobalamin from dietary proteins. The vitamin cannot proceed to the IF binding step. Therapeutic Consequence: Absorption of unbound, crystalline B12 (Oral B12 Supplement) remains intact via passive diffusion. Diagnostic Hint: The Modified Schilling Test (using food bound B12 ) is abnormal, while the Standard Test (using free B12) is normal. True Malabsorption: The defect occurs downstream, typically impairing the IF-dependent uptake in the terminal ileum. Etiologies include Pernicious Anemia (Anti-IF Antibodies destroy IF-producing parietal cells) or Ileal Pathology (surgical resection or Crohn’s disease). Therapeutic Consequence: Standard oral supplementation is generally ineffective, necessitating Parenteral B12 replacement. Diagnostic Hint: Both the Standard and Modified Schilling Tests are abnormal.
Table 1: Comparison of maldigestion versus true malabsorption of Vitamin B12.
| Maldigestion (Food-Cobalamin Malabsorption, FCM) | True Malabsorption (Free Cobalamin Malabsorption) | |
|---|---|---|
| Pathophysiology | Impaired release of cobalamin from dietary proteins or haptocorrin due to reduced gastric acidity or pepsin activity or reduced biliary secretions. | Impaired absorption of free cobalamin–intrinsic factor complex in the terminal ileum. |
| Typical patient profile | Elderly, polymedicated, chronic gastritis, proton pump inhibitors (PPIs) or metformin users. | Patients with autoimmune gastritis, gastric/ileal resections, inflammatory bowel disease, celiac disease. |
| Main causes |
|
|
| Ability to absorb crystalline B12 | Preserved → can absorb free B12 normally. | Impaired → cannot absorb crystalline B12 adequately. |
| Clinical presentation | Often mild, insidious, subclinical; anemia or neurologic symptoms develop gradually. | More severe deficiency; higher risk of megaloblastic anemia, neuropathy, neurocognitive decline. |
| Diagnostic clues | Low serum B12 despite normal diet; responds to oral crystalline B12 supplementation. | Very low B12, presence of intrinsic factor antibodies, history of surgery or ileal disease; poor response to oral therapy. |
| Treatment | High-dose oral, sublingual, or intranasal B12 (≥1000 µg/day). | Parenteral B12 (intramuscular or subcutaneous) usually required for long-term correction. |
Etiologies of food-cobalamin malabsorption
Food-Cobalamin Malabsorption (FCM) is defined by the in ability to release cobalamin from dietary proteins in the stom ach due to impaired gastric acidity or haptocorrin du to biliary or pancreatic secretion deficiencies (Table 1) [8]. In contrast, the absorption of crystalline (unbound) cobalamin remains in tact in FCM, a distinction historically revealed by the modified Schilling test [3]. This mechanism accounts for a substantial majority—50–70% of B12 deficiency cases in older adults—and its causes are diverse: age-related gastric atrophy is the most common cause in the elderly, leading to severe hypochlorhydria and failure to liberate protein-bound cobalamin [2]. Chronic He licobacter pylori infection also drives gastric atrophy and hypo chlorhydria, with eradication therapy often restoring absorption [13]. The widespread use of Proton-Pump Inhibitors (PPIs) and H2 receptor antagonists directly impairs gastric acid secretion, similarly interfering with cobalamin release [12]. Metformin therapy interferes with the calcium-dependent endocytosis of the IF–cobalamin complex at the ileal level [14], representing a cumulative risk with treatment duration. Small intestinal bacte rial overgrowth (SIBO) increases competition for luminal cobal amin, contributing to FCM in patients with motility disorders or chronic PPI use [15]. Exocrine pancreatic insufficiency impairs the necessary degradation of haptocorrin by pancreatic prote ases, a mechanism typically corrected by enzyme replacement [16]. Finally, Bariatric Surgery (e.g., Roux-en-Y gastric bypass) fundamentally alters B12 absorption physiology by drastically reducing gastric acid and bypassing the IF-producing mucosa, mandating lifelong monitoring and replacement [17].
Etiologies of free cobalamin malabsorption
True malabsorption involves impaired uptake of the IF–co balamin complex at the terminal ileum; consequently, both the standard and modified Schilling’s tests are typically abnormal (Table 1). Pernicious Anemia (PA), or Biermer’s disease, is an autoimmune disorder primarily targeting the gastric parietal cells responsible for producing IF and gastric acid [18]. The re sulting autoimmune destruction leads to both IF deficiency and hypochlorhydria, severely impairing cobalamin absorption in the terminal ileum. Although PA accounts for less than 10% of total B12 deficiency cases in older adults, its clinical significance is profound due to the risk of severe neurological complications, including irreversible peripheral neuropathy and cognitive dis turbances; early diagnosis and lifelong parenteral or high-dose oral B12 replacement are crucial to mitigate this damage. Gas tric resections fundamentally reduce the secretion of gastric acid and IF, placing patients at high risk of B12 deficiency within a few years post-surgery [9]. Similarly, the terminal ileum is the exclusive site for IF–cobalamin complex absorption, meaning surgical resection or inflammatory destruction of this region— as seen in Crohn’s disease—results in impaired uptake; stud ies indicate up to 29% of Crohn’s patients with ileal resection develop deficiency [10]. While the primary defect in Celiac dis ease is villous atrophy of the proximal small intestine, exten sive mucosal involvement can lead to generalized malabsorp tion, potentially impairing B12 uptake alongside iron and folate. Rare genetic disorders, such as Imerslund–Gräsbeck syndrome, cause lifelong deficiency due to mutations affecting the cubam receptor (cubilin and amnionless) that mediates ileal uptake of the IF–cobalamin complex [19], requiring parenteral therapy. Beyond PPIs and metformin, several medications interfere with cobalamin status: Nitrous oxide anesthesia directly inactivates B12 through oxidation of its cobalt center [20], and drugs like methotrexate, hydroxyurea, or chloramphenicol indirectly in terfere by targeting DNA synthesis pathways dependent on fo late/B12 .
Epidemiology and global burden
Vitamin B12 deficiency represents a significant and under recognized global health problem, particularly affecting older adults and populations with limited access to animal-derived foods [2]. Prevalence estimates vary based on diagnostic crite ria and cohorts studied [3]. In the United States, NHANES data show that biochemical deficiency (serum B12 <150 pmol/L) af fects approximately 6% of adults younger than 60 years, rising to nearly 20% in individuals older than 60 [6]. European cohorts report similar patterns, with prevalence ranging from 5–15% in community-dwelling elderly and reaching 35–38% in institution alized populations [7]. FCM is the dominant underlying mecha nism, estimated to account for 50–70% of non-PA anemia B12 deficiencies in the elderly [8]. By contrast, PA contributes less than 10% of cases but remains the primary cause of severe de ficiency requiring lifelong parenteral replacement. Surgical in terventions also markedly increase risk: B12 deficiency affects 15–30% of post-bariatric surgery patients within one year [9]. Similarly, ileal resection or inflammatory bowel disease involv ing the terminal ileum significantly increases risk [10]. Medica tions are another major driver; metformin therapy is associated with biochemical B12 deficiency in 10–30% of long-term users [11]. Chronic use of PPIs or H2 -blockers is linked to impaired release of protein-bound B12 , with studies showing up to 40% of elderly adults on long-term PPI therapy exhibiting low serum levels [12]. Beyond high-income countries, the burden is mag nified in low- and middle-income regions where low intake of animal-derived foods is common, with prevalence exceeding 40–50% reported in South Asia, Latin America, and parts of Af rica [6]. These data underscore the public health significance of B12 deficiency worldwide, particularly in aging societies where frailty, multimorbidity, and polypharmacy amplify the clinical impact of malabsorption syndromes. Targeted screening, early detection, and preventive interventions are essential to miti gate morbidity and functional decline.
Other populations and high-risk groups
Recognizing these high-risk groups is essential to guide tar geted screening, early detection, and preventive supplementa tion to mitigate hematologic, neurologic, and cognitive sequel ae (Table 2). Strict vegetarians and vegans are highly vulnerable to B12 deficiency because cobalamin is almost exclusively found in animal-derived foods; without fortified products or supple ments, deficiency can develop within years, posing risks of meg aloblastic anemia, neuropathy, and cognitive impairment [21]. Studies report suboptimal B12 status in 30–80% of long-term vegans and 10–20% of vegetarians, with risks exacerbated by age-related malabsorption and polypharmacy in elderly vegetarians; compared with omnivores, these individuals exhibit lower serum B12 and holotranscobalamin, alongside elevated methylmalonic acid and homocysteine, necessitating routine screening and supplementation [21]. Beyond community dwelling older adults, populations at increased risk extend to those with gastrointestinal disorders, prior gastric or ileal sur gery, chronic medication use, or strict dietary restrictions [2]. Institutionalized elderly populations are particularly vulnerable, with prevalence rates approaching 38%, reflecting the cumu lative effects of multimorbidity, polypharmacy, and limited di etary diversity.
Table 2: Screening, prediction, and prevention of vitamin B12 deficiency in at-risk populations.
| Domain | Strategy | Target population | Methods / Tools | Evidence / Notes |
|---|---|---|---|---|
| Screening | Serum B12 measurement | Elderly (>60 years), vegetarians/vegans, patients with GI surgery, long-term PPI/metformin users | Serum cobalamin, holotranscobalamin, MMA, homocysteine | Routine screening recommended for high-risk groups; serum B12 alone may miss functional deficiency |
| Prediction / Risk Assessment | Identify risk factors | Elderly, patients with autoimmune gastritis, malabsorption syndromes, chronic pancreatic insufficiency | Clinical history, medication review, dietary assessment | Risk stratification helps prioritize screening and early intervention |
| Prevention | Dietary counseling | Vegetarians, vegans, elderly | Encourage B12-rich foods (meat, fish, dairy, fortified foods) | Regular dietary intake may suffice if absorption is intact |
| Prevention | Oral supplementation | Elderly, FCM, limited dietary intake | Daily or weekly oral cyanocobalamin/methylcobalamin (e.g., 250–1000 μg/day) | Effective in mild-to-moderate deficiency and functional malabsorption |
| Prevention | Parenteral supplementation | Severe deficiency, malabsorption (pernicious anemia, post-gastrectomy) | IM or SC B12 injections (1000 μg every 1–3 months) | Rapid correction of hematologic and neurologic deficits |
| Follow-up / Monitoring | Re-assess biochemical and clinical response | All treated patients | Serum B12, MMA, hematology, neurologic evaluation | Ensures efficacy, adjusts dose, prevents relapse |
Clinical presentation
Vitamin B12 deficiency presents a wide clinical spectrum, ranging from asymptomatic biochemical abnormalities to se vere hematologic and neurologic syndromes. Hematologic manifestations classically include macrocytic anemia, hyper segmented neutrophils, pancytopenia, and megaloblastic bone marrow changes. Neurologic features may be equally promi nent, encompassing peripheral neuropathy, posterior column degeneration with impaired proprioception and vibration sense, gait ataxia, cognitive decline, and psychiatric disturbances [2]. Importantly, neurologic signs may precede hematologic abnor malities in up to one-quarter of patients, underscoring the ne cessity for early recognition [2]. The underlying clinical presen tation is often influenced by the mechanism of deficiency: in maldigestion syndromes (FCM), deficiency tends to be gradual and insidious, whereas true malabsorption may cause earlier and more severe manifestations (Table 1). Chronic untreated deficiency, irrespective of the mechanism, may result in irre versible neurologic injury if not corrected within six months. A particular challenge lies in the recognition of subtle or subclini cal cobalamin deficiency, common in the elderly with FCM due to hypochlorhydria or chronic medication use (PPIs, metformin) [22]. While these patients may initially lack overt anemia, they remain at risk for progressive neurologic impairment if unrec ognized, though the FCM syndrome can also lead to true B12 deficiency with clinical manifestations that are indistinguishable from those observed in PA.
Diagnosis and etiologic workup
Initial evaluation for suspected B12 deficiency begins with serum cobalamin measurement, although its sensitivity is limited, particularly when values are near the lower reference range. Functional biomarkers, such as Methylmalonic Acid (MMA) and total homocysteine, rise earlier in the course of deficiency, significantly improving diagnostic accuracy, especially in patients with borderline serum B12 [5]. Measuring holotranscobalamin (HoloTC), which represents the fraction of bioavailable cobalamin, may further aid in detecting subclinical or subtle deficiency before overt hematologic or neurologic manifestations appear. Once B12 deficiency is confirmed, a comprehensive etiologic workup is warranted to guide long term management [2]. This evaluation includes serologic testing for Intrinsic Factor (IF) and parietal cell antibodies to identify PA (IF antibodies are highly specific; parietal cell antibodies are more sensitive but less specific). Serologic testing also includes IgG antibodies against Helicobacter pylori, which may contribute to chronic gastritis and secondary maldigestion, and anti-transglutaminase antibodies when celiac disease is suspected. Structural or functional causes of malabsorption should be evaluated through ileal imaging or endoscopy for Crohn’s disease, surgical resection, or other ileal pathology, as well as assessment of pancreatic exocrine function in cases of suspected insufficiency. A thorough medication review is essential, as long-term use of PPIs, H2 -receptor antagonists, or metformin may impair cobalamin absorption. Together, this integrated approach—combining serologic, functional biomarker, structural, and pharmacologic evaluation— facilitates accurate etiologic diagnosis and guides appropriate long-term management.
Treatment and management
High-dose oral crystalline cobalamin (1000–2000 μg/day) is highly effective for both FCM and many cases of PA, relying on passive diffusion (∼1% absorption) to achieve sufficient sys temic levels. Parenteral therapy is indicated for patients with severe neurologic involvement, extensive true malabsorption, or concerns regarding adherence to oral therapy [5]. Regimens typically involve cyanocobalamin (e.g., 1 mg/day for 7 days, then 1 mg/week for 4 weeks, followed by monthly mainte nance) or hydroxocobalamin (e.g., 1 mg intramuscularly every 2–3 days for two weeks, followed by monthly maintenance). Comparative studies demonstrate equivalent hematologic and neurologic responses between high-dose oral cyanocobalamin and parenteral hydroxocobalamin, although hydroxocobalamin offers the advantage of longer tissue retention. While methylco balamin may confer specific neurotrophic benefits, particularly in peripheral neuropathy, robust clinical evidence supporting its superiority remains limited.
Monitoring response includes assessing the reticulocyte count at 7–10 days, expecting normalization of hemoglobin and Mean Corpuscular Volume (MCV) within 6–8 weeks. Biochemi cal reassessment of serum vitamin B12 , MMA, or homocysteine should occur at 3–6 months. In cases of permanent malabsorp tion, such as Biermer’s disease or extensive ileal resection, life long replacement therapy is mandatory to prevent recurrence and irreversible neurologic damage.
Future directions: AI, multi-omics, and precision medicine
Further research on B12 deficiency increasingly leverages advanced technologies, including Artificial Intelligence (AI), Ma chine Learning (ML), and multi-omics approaches [23]. AI and ML can analyze large, complex datasets to identify subtle pat terns and predict which patients are at highest risk of deficiency. Multi-omics—including genomics, proteomics, and metabolo mics—help uncover novel biomarkers (such as holotranscobala min) and elucidate pathways involved in cobalamin absorption and metabolism. Specifically, integrating microbiome data with metabolomic profiles can reveal how gut flora influence B12 bioavailability [23]. ML models can optimize screening intervals by combining clinical, laboratory, and omics data. Comparative studies utilizing these tools can refine guidelines for oral versus parenteral therapy recommendations in complex populations (e.g., post-surgical or inflammatory bowel disease patients). Longitudinal multi-omics studies hold the potential to link sub clinical deficiency directly to important clinical outcomes, such as cognitive decline, frailty, and cardiovascular events. These integrated approaches allow for precision medicine strategies, enabling clinicians to tailor supplementation and monitoring to individual risk profiles. Ultimately, AI-driven predictive models facilitate early intervention before overt anemia or irreversible neurological damage occurs. Overall, integrating AI, ML, and omics holds great promise to significantly improve the under standing, diagnosis, and management of B12 deficiency [23].
Conclusion and clinical implications for clinicians
Maldigestion and malabsorption of cobalamin are frequent causes of deficiency, many of which are potentially reversible with proper intervention. Elderly patients, those with gastro intestinal disorders, individuals who have undergone bariatric or gastric surgery, and patients on chronic PPIs or metformin are at particularly high risk. Clinicians should maintain a high index of suspicion to identify deficiency early, even before clini cal symptoms appear. Laboratory evaluation, including serum B12 and potentially holotranscobalamin or Methylmalonic Acid (MMA), aids in accurate diagnosis. Prompt initiation of oral or parenteral vitamin B12 therapy is critical to prevent irrevers ible hematologic and neurological complications. Monitoring B12 levels over time ensures treatment efficacy and allows for supplementation adjustment as needed. Personalized strate gies based on patient risk factors enhance prevention and long term outcomes. Awareness of reversible causes allows for tar geted interventions to restore normal cobalamin metabolism. Integration of precision medicine approaches, including AI and omics data, may further refine risk stratification and manage ment. Overall, proactive recognition, tailored supplementation, and vigilant follow-up are essential components of preventive internal medicine in at-risk populations.
Declarations
Conflicts of interest: None declared.
Acknowledgments: The authors thank the clinicians and researchers of the CAREB12 (CAREnces en vitamien B12) group at the Hôpitaux Universitaires de Strasbourg (HUS) for their valuable contributions.
References
- Guéant JL, Guéant-Rodriguez RM, Alpers DH. Vitamin B12 absorption and malabsorption. Vitam Horm. 2022; 119: 241-274.
- Andrès E, Loukili NH, Noel E, Kaltenbach G, Abdelgheni MB, Perrin AE, Noblet-Dick M, Maloisel F, Schlienger JL, Blicklé JF. Vitamin B12 (cobalamin) deficiency in elderly patients. CMAJ. 2004; 171: 251–259.
- Carmel R. Current concepts in cobalamin deficiency. Annu Rev Med. 2000; 51: 357–375.
- Green R, Allen LH, Bjørke-Monsen AL, Brito A, Guéant JL, Miller JW, Molloy AM, Nexo E, Stabler S, Toh BH, Ueland PM, Yajnik C. Vitamin B12 deficiency. Nat Rev Dis Primers. 2017; 3: 17040.
- Obeid R, Andrès E, Češka R, Hooshmand B, Guéant-Rodriguez RM, Prada GI, Sławek J, Traykov L, Ta Van B, Várkonyi T, Reiners K, Vitamin B Consensus Panelists Group. Diagnosis, treatment and long-term management of vitamin B12 deficiency in adults: a Delphi expert consensus. J Clin Med. 2024; 13: 2176.
- Allen LH. How common is vitamin B-12 deficiency? Am J Clin Nutr. 2009; 89: 693S–696S.
- Hvas AM, Nexo E. Diagnosis and treatment of vitamin B12 deficiency—an update. Haematologica. 2006; 91: 1506–1512.
- Andrès E, Affenberger S, Vinzio S, Kurtz JE, Noel E, Kaltenbach G, Maloisel F, Schlienger JL, Blicklé JF. Food-cobalamin malabsorption in elderly patients: clinical manifestations and treatment. Am J Med. 2005; 118: 1154–1159.
- Parrott J, Frank L, Rabena R, Craggs-Dino L, Isom KA, Greiman L. American Society for Metabolic and Bariatric Surgery integrated health nutritional guidelines for the surgical weight loss patient: micronutrients. Surg Obes Relat Dis. 2017; 13: 727–741.
- Battat R, Kopylov U, Szilagyi A, Saxena A, Rosenblatt DS, Warner M, Bessissow T, Seidman E, Bitton A. Vitamin B12 deficiency in inflammatory bowel disease: prevalence, risk factors, evaluation, and management. Inflamm Bowel Dis. 2014; 20: 1120–1128.
- Pautas E, Chérin P, De Jaeger C, Godeau P. Carence en vitamine B12 chez le sujet âgé. Presse Med. 1999; 28: 1767–1770.
- Lam JR, Schneider JL, Zhao W, Corley DA. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. 2013; 310: 2435–2442.
- Kaptan K, Beyan C, Ural AU, Cetin T, Avcu F, Gülşen M, Finci R, Yalçín A. Helicobacter pylori—is it a novel causative agent in vitamin B12 deficiency? Arch Intern Med. 2000; 160: 1349–1353.
- Parsonage I, Wainwright D, Barratt J. Vitamin B12 deficiency in long-term metformin use and clinician awareness: a scoping review protocol. BMJ Open. 2025; 15: e101016.
- Gudan A, Kozłowska-Petriczko K, Wunsch E, Bodnarczuk T, Stachowska E. Small intestinal bacterial overgrowth and non-alcoholic fatty liver disease: what do we know in 2023? Nutrients. 2023; 15: 1323.
- Guéant JL, Champigneulle B, Gaucher P, Nicolas JP. Malabsorption of vitamin B12 in pancreatic insufficiency of the adult and of the child. Pancreas. 1990; 5: 559–567.
- Carvalho IR, Loscalzo IT, Freitas MF, Jordão RE, Friano TC. Incidence of vitamin B12 deficiency in patients submitted to Fobi-Capella Roux-en-Y bariatric surgery. Arq Bras Cir Dig. 2012; 25: 36–40.
- Lahner E, Annibale B. Pernicious anemia: new insights from a gastroenterological point of view. World J Gastroenterol. 2009; 15: 5121–5128.
- Kingma SDK, Neven J, Bael A, Meuwissen MEC, van den Akker M. Imerslund-Gräsbeck syndrome: a comprehensive review of reported cases. Orphanet J Rare Dis. 2023; 18: 291.
- Mohammed H, Sara E, Bouchra O. Acute psychotic and vitamin B12 deficiency in a patient with nitrous oxide misuse: a case report. SAGE Open Med Case Rep. 2024; 12: 2050313X241269577.
- Clemente-Suárez VJ, Redondo-Flórez L, Martín-Rodríguez A, Curiel-Regueros A, Rubio-Zarapuz A, Tornero-Aguilera JF. Impact of vegan and vegetarian diets on neurological health: a critical review. Nutrients. 2025; 17: 884.
- Carmel R. Subtle and atypical cobalamin deficiency states. Am J Hematol. 1990; 34: 108–114.
- Wiedemann A, Oussalah A, Guéant Rodriguez RM, Jeannesson E, Merten M, Rotaru I, et al. Multiomic analysis in fibroblasts of patients with inborn errors of cobalamin metabolism reveals concordance with clinical and metabolic variability. EBioMedicine. 2024; 99: 104911.