
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 6
Gongylonemiasis - Literature review with case report of a gastric worm wandering aimlessly in oral epithelium
Jerry E Bouquot, DDS, MSD, DABOMP, DABOM(Hon), FICD, FACD1*; Safia Durab, BDS, BSc, MSc2; Griffin Cross, DDS3; Logan Williams, DDS4
1Emeritus Professor & Past Chair, Department of Diagnostic & Biomedical Sciences, University of Texas School of Dentistry at
Houston, Houston, Texas, USA.
2Assistant Professor, Department of Diagnostic & Biomedical Sciences, University of Texas School of Dentistry at Houston,
Houston, Texas, USA.
3Private Practice of General Dentistry, Roanoke, Virginia.
4Private Practice of Endodontics, Roanoke, Virginia.
*Corresponding Author : Jerry E Bouquot
Emeritus Professor & Past Chair, Department of
Diagnostic & Biomedical Sciences, University of Texas
School of Dentistry at Houston, 212 Tibbs Road,
Morgantown, WV 26508, Houston, Texas, USA.
Tel: 281-745-2330;
Email: bouquot@aol.com
Received : Nov 17, 2025
Accepted : Dec 26, 2025
Published : Jan 07, 2026
Archived : www.jjgastro.com
Copyright : © Bouquot JE (2026).
Abstract
Background: A very rare parasite is popularly called the “stitch worm” because it looks like a piece of thread siting on the mucosa. It is also called the “gullet worm” because of its very strong preference to live its lifetime not just in the mouth, but specifically inside the oral epithelium, feeding off of epithelial cells. It arrives in our stomachs after being swallowed with insect parts ingested with our food. Once there its “eats” through the stomach epithelium, spending weeks or months maturing while crawling submucosally up the esophagus to the nonkeratinized epithelium of the mouth. It is a fascinating creature but seldom causes serious issues for the host.
Methods & materials: We report the 12th case of congylonemiasis of the mouth.
Case: A 70-year-old woman who felt a “weird sensation, like something’s moving” from one commissure to the other commissure of her lower lip mucosa. Her dentist saw an asymptomatic, white, serpiginous, thread-like submucosal structure which was easily removed with a forceps after incision of the mucosal area presumed to be the “head.” When removed, it was seen to be a squirming 13 mm long, worm-like organism less than 0.5 mm in diameter; it wrapped its “tail” around the forceps during removal. After excision there was no recurrence.
Conclusion: We present a very rare example of perhaps the strangest living creature to not only prefer the oral environment, but to selectively choose to live internally within the oral epithelium itself.
Keywords: Oral parasites; Oral nematodes; Gongylonemiasis; Gongylonema pulchrum; Gullet worm; Stitch worm; Roundworm.
Citation: Bouquot JE, Durab S, Cross G, Williams L. Gongylonemiasis - Literature review with case report of a gastric worm wandering aimlessly in oral epithelium. J Gastroenterol Res Pract. 2026; 6(1): 1241.
Introduction
Very occasionally a fascinating oral pathosis comes along that is so odd that it completely fascinates us, even though it is extremely unlikely that a dentist would ever encounter it. We herein present an example of such a lesion, representing the 12th US example reported since its first description in the 1850s [1,2]. This “lesion” is an oral parasite from the genus gongylonema, a thread-like nematode described initially as a “worm taken from the mouth of a child [2-10]. It remains relatively innocuous in humans but can be fatal in other mammals or in birds [11]. Infection by this parasite is called Gongylonemiasis, but lay terms for it are more interesting: stitch worm for its clinical thread-like appearance (Figure 1); gullet worm, for its preference for living in the mouth; and wiggie worm for its serpiginous or snake-like motion, a motion that can often be felt by the patient [3,6].
Seen worldwide, this parasite can be found in all socioeco nomic strata and is far from being limited to underdeveloped countries [3,9,12]. Throughout the world, fewer than 100 oral cases have been reported in humans [1-8]. We present herein an example of Gongylonemiasis in a patient from Virginia. This case has been briefly reported in a newsletter of the American Academy of Oral & Maxillofacial Pathology [13].
Case reports
Patient information
A 70-year-old female who presented to her dentist because of a “weird sensation, like something’s moving” on her lower lip mucosa. The sensation was intermittent and first noticed a month earlier; there were no previous similar incidents. She had no unusual prior dental issues, and her medical history was negative except for an episode of “food poisoning” two months previously.
Clinical findings
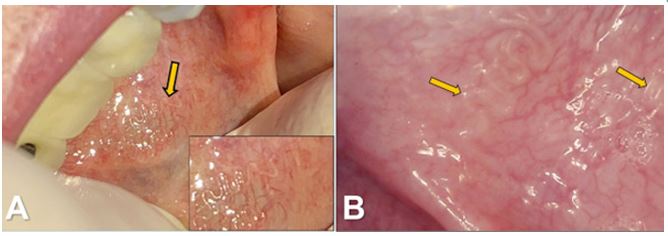
At examination, the patient demonstrated a serpiginous, thin, thread-like structure immediately beneath or within the epithelium, without surrounding erythema or edema, and with out tenderness or pain (Figure 2A). She explained that the area felt “rough” to her tongue and the affected area appeared to move from one labial commissure to the other, usually taking days to do so. Some days it disappeared entirely, returning in a day or two. Occasionally she would feel the same sensation on her buccal mucosae.
Diagnosis and treatment
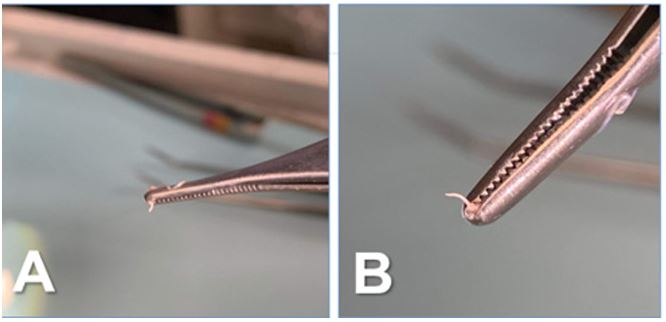
The patient was referred to an oral surgeon, but the lesion was not visible when she arrived at the surgeon’s office, so no treatment was performed. When it became visible and palpa ble again a few days later, she returned to her general dentist, who carefully incised along a portion of the “thread” and, with a forceps, easily removed a squirming 13 mm long, worm-like organism less than 0.5 mm in diameter (Figure 3A). The worm appeared not to have a head on either end, but after removal it wrapped one end around the forceps (Figure 3B); presumably this was the “tail” because it was the end facing away from the direction of submucosal movement.
The parasite was sent to an Infectious Disease laboratory for identification, confirmed by the Centers for Disease Control (CDC): it was diagnosed as a nematode (roundworm), specifi cally referred to as Gongylonemas pulchrum.
After removal of the worm, the affected oral mucosae healed uneventfully, quickly returning to normal. The patient experi enced no recurrence of the worm-like structure or abnormal mucosal sensations. Since removal appeared to be an adequate treatment, she was not treated with albendazole, the broad spectrum antihelmintic suggested for nematodes [14].
Discussion
Oral gongylonemiasis is one of the rarest, and certainly one of the most eerie lesions affecting the mouth [1-8]. As previous ly mentioned, the offending organism is a parasite, a nematode called Gongylonema pulchrum. Of the 47 species thus far iden tified, only Gongylonema pulchrum infects humans. Humans become infected by drinking contaminated water or eating food contaminated by insect parts, especially those of dung beetles and cockroaches [7,10-12].
Eating raw, unwashed vegetables is one means by which to become infected, but this is not a disease unique to regions where food cleansing and water processing are deficient. It is ostensibly impossible to avoid including a small amount of insect parts in our processed foods, and so all countries, in cluding the United States, allow it so long as the amount is below certain set legal limit. For example, the FDA allows 1 or more rodent hairs and up to 30 insect fragments for every 100 grams/3.5 ounces of peanut butter [12,14].
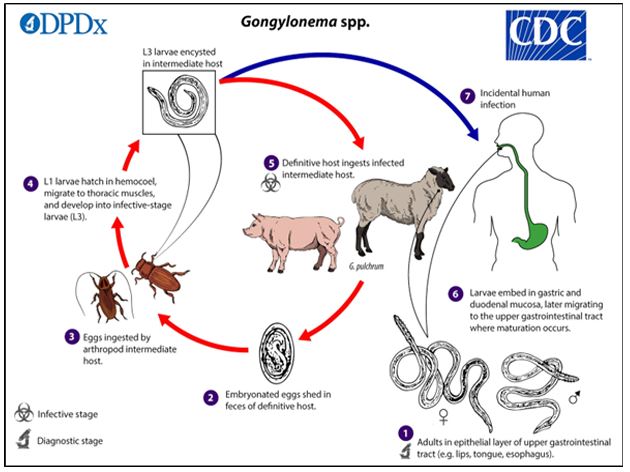
These insect parts are, as mentioned, the vector for the spread of gongylonemiasis. Within a month after a gongylon ema egg is swallowed by an intermediate insect host it develops into an immature, encapsulated larva, in which state it remains until the insect, or parts thereof, are ingested by a final or de finitive host, such as a human. Once ingested, it unencapsulates in the stomach, perforates the stomach lining, and starts its transformation into a mature larva [14].
This larva has a remarkably strong affinity for non-keratinized oral epithelial cells and somehow knows where to find them. While continuing to mature, it begins traveling upward within and beneath gastric and esophageal mucosae, slowly finding its way to the “place where it belongs,” the mouth, as illustrated in Figure 5. This process takes weeks to months, with the para site reaching the mouth as a fully developed adult worm, con tinuous traveling within the oral epithelium itself, occasionally plunging down into underlying stroma, and feeding (Grazing? Foraging?) on squamous cells at it moves about [3,9]. Oral in fections have been reported to last up to a decade, and worms can reproduce within the oral mucosa, leading to the occasional presentation of multiple nematodes in one mouth.
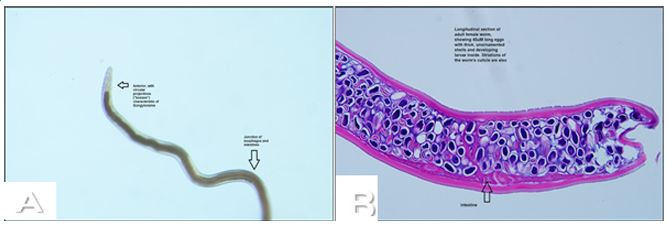
The adult Gongylonema is a whitish, sometimes colorless, unsegmented worm covered by a tough cuticle. It has no ap pendages, no respiratory system, no circulatory system and only the most rudimentary of nervous systems [7,9,11]. For all practical purposes, it is nothing more than a small, moving “intestine,” although the anterior half of the internal tubular structure is called an esophagus and, surprisingly, there seems to be no identifiable excretory structure [10]. While this worm appears to move “forward” in one direction, it has no obvious head and all movement occurs by the activity of several small surface projections or papillae on its ends. No mouth structures are present in the human worms, but a rodent Gongylonema has recently been found to have bilateral “interlabial plates,” a possible mechanism for “chewing” its food [17].
The worm typically manifests itself within labial, buccal and/ or ventral tongue mucosae, but has also been found in the oral floor, tonsils and esophagus, usually as a single worm, but up to 4 have been found in one mouth [6,8,10]. In the esophagus, worms as long as 15 cm. have been reported, always as thin thread-like creatures, although they become slightly thicker as they become longer. In this location, they occasionally become numerous enough to form intertwining-thread plaques admixed with micro-organisms native to the esophagus [6,9,14,15].
A worm will periodically spend a week or more in slightly deeper fibrous stroma, during which time it appears to the patient that the disease has disappeared, only to eventually return [7,8]. This waxing and waning has led to at least a few affected patients being seen by their physicians during a time when the organism was less obvious, or clinically invisible, lead ing to a mistaken diagnosis of delusional parasitosis or parasitic psychosis [9]. There are, in fact, truly psychotic individuals who complain of finding, and removing, imaginary worms from their mouths, and so this diagnostic dilemma is understandable.
• The nematode seldom induces a local inflammatory re sponse, although a few oral examples have appeared with a thin surrounding erythema. Without such an inflammatory change, there is little to see beyond the serpiginous thread like submucosal/intraepithelial structure, but some patients have presented with a few, often intermittent symptoms or signs [4,5,8], A sensation of focal mucosal “roughness” or “dryness” which can be felt by the tongue
• A sensation of actual movement of the nematode, traveling 2-3 cm per day
• Rarely, pruritus, focal pain, pharyngitis or esophagitis
• Rarely, the worm is seen actually above the mucosa
• No systemic signs or symptoms are noted once it is in its oral location, but stomach pain or nausea may accompany the initial ingestion
• Blood values remain normal and an allergic reaction to the worm has not yet been reported.
This organism is easily diagnosed via its unique clinical pre sentation, but biopsy of the worm is recommended for confir mation. Of interest in this regard is the fact that biopsy of the larva as it travels up from the stomach is not recommended since, unlike the adult form in the mouth, the developing or ganism is typically ahead of the clinically visible “track” in the mucosa and so will likely not be seen in the removed tissue sample. A specific genetic profile is available for this worm, but it has been deemed unnecessary in almost all reported cases [9]. Serological testing of the patient is seldom useful, but when performed, 20% of affected individuals show eosinophilia and even fewer show elevated IgE levels [8,10,14].
Gongylonemiasis is usually treated by the expedient removal of the visible nematode, preferably taking the “head” out first; this may require a few hours of observation, to determine in which direction the worm is moving [9,12]. Occasionally, pa tients are treated with albendazole (ivermectin), as previously mentioned, especially if the nematode is found in the esopha gus [6,14]. Thus far, there have been no serious complications reported from an oral worm, and the oral mucosa routinely re turns to normal within hours of removal of the parasite [9].
That being said, at least one case has been reported to be associated with an esophageal carcinoma [16]. Although its bio logical or etiological role could not be determined in that case, it calls to mind an early Danish investigation into this parasite, one that found an association with stomach carcinomas in rats [18]. This association led the investigator, Johannes Fibiger, to name it Gongylonema neoplasticum (also later called Spiroptera car cinoma) and earned him the 1927 Nobel Prize for Physiology or Medicine. Unfortunately, his research was later found to be seriously flawed: 1) the rats were purposely deprived of vitamin A, a deficiency of which has been associated with stomach car cinomas; 2) Review of his cases determined that many, perhaps most, were merely hyperplasias, not malignancies. Ironically, his reputation has been repaired somewhat by recently discovered associations between these cancers and other helmintha [18].
While the present report applies to a rare human infection, the gullet worm is a common parasite in other mammals, es pecially cows, horses and pigs, and has been also reported in bears, skunks, primates, rodents, rabbits and hedgehogs; birds are also often infected [11,17-19]. Altogether, there are 37 dif ferent species found in mammals and 10 in birds, with different species preferring particular types of animals [9,12,17-20].
As with humans, these animals typically acquire the para site by ingesting insects in their drinking water or food. Inves tigations have found gongylonemiasis infection in up to 16% of cattle in Europe, in more than 20% of rats in the U.S., and in approximately 5% of wild animals in India [7,19-21]. Unlike the human experience, moreover, in other animals this infection can be fatal, as the nematode breaks through the stomach or intestinal walls to perforate large blood vessels, cause thrombo sis and induce destructive granulomas [6,12,20].
Conclusion
A case is herein presented of a very rare human parasite, Gongylonema pulchrum, which enters the body through the stomach and routinely “climbs” up the esophagus to live in and move through the epithelial and subepithelial structures of the oral, oropharyngeal, or esophageal mucosae. It creates a serpiginous, thread-like elevation of the mucosa and can be seen, and felt, to slowly move about under the nonkeratinized oral epithelium, possibly for years. It feeds off surrounding or overlying epithelial cells. Serious consequences do not ensue once the parasite has arrived in the mouth, and simple surgical removal of the roundworm typically results in complete cure.
Declarations
Conflict statement: None of the authors have a conflict of any type relative to this manuscript or case.
Funding statement: No funding was provided for this manu script.
References
- Leidy J. A synopsis of entozoa and some of their ecto-congeners, observed by the author. Philadelphia: Merrihew & Thompson; 1856.
- Crusz H, Sivalingam V. A note on the occurrence of Gongylonema pulchrum, Molin, 1857, in man in Ceylon. J Parasitol. 1950; 36: 25.
- Eberhard ML, Busillo C. Human Gongylonema infection in a resident of New York City. Am J Trop Med Hyg. 1999; 6: 51–52.
- Wilson ME, Lorente CA, Allen JE, Eberhard ML. Gongylonema infection of the mouth in a resident of Cambridge, Massachusetts. Clin Infect Dis. 2001; 32: 1378–1380.
- Haruki K, Furuya H, Saito S, Kamiya S, Kagei N. Gongylonema infection in man: a first case of gongylonemiasis in Japan. Helminthologia. 2005; 42: 63–66.
- Ayala MA, Yencha MW. Gongylonema: a parasitic nematode of the oral cavity. Arch Otolaryngol Head Neck Surg. 2012; 138: 1082–1084.
- Allen JD, Esquela-Kerscher A. Gongylonema pulchrum infection in a resident of Williamsburg, Virginia, verified by genetic analysis. Am J Trop Med Hyg. 2013; 89: 755–757.
- Pesson B, Hersant C, Biehler JF, et al. First case of human gongylonemiasis in France. Parasite. 2013; 20: 5.
- Xiaodan L, Zhensheng W, Ying H, Hongwei L, Jianqiu J, Peiru Z, Sha S, Zhimin Y. Gongylonema pulchrum infection in the human oral cavity: a case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018; 125: e49–e53.
- Kramar U, Skvarč M, Logar M, Islamović S, Kolenc M, Šoba B. First case of human Gongylonema pulchrum infection in Slovenia. J Helminthol. 2019; 94: e62.
- Centers for Disease Control and Prevention. Gongylonema infection. Atlanta: CDC; 2022.
- Belluco S, Losasso C, Maggioletti M, Alonzi CC, Paoletti MG, Ricci A. Edible insects in a food safety and nutritional perspective: a critical review. Compr Rev Food Sci Food Saf. 2013; 12: 296–313.
- Bouquot JE, Durab S. A worm wandering inside the oral epithelium. AAOMP Focus. 2024 Dec.
- Bouchaud O, Houzé S, Schiemann R, Durand R, Ralaimazava P, Ruggeri C, Coulaud JP. Cutaneous larva migrans in travelers: a prospective study with assessment of therapy with ivermectin. Clin Infect Dis. 2000; 31: 493–498.
- Huang Q, Wang J, Yang T, Liu Y. Multiple Gongylonema pulchrum worms in a human esophagus. Endoscopy. 2016; 48 Suppl 1: E24–E25.
- Chakraborty A. Occurrence and pathology of Gongylonema infection in captive wild herbivores. Vet Parasitol. 1994; 52: 163–167.
- Modlin IM, Kidd M, Hinoue T. Of Fibiger and fables: a cautionary tale of cockroaches and Helicobacter pylori. J Clin Gastroenterol. 2001; 33: 177–179.
- Parker JC, Holliman RB. Notes on Gongylonema pulchrum Molin, 1857 (Nematoda: Spiruridae) in the gray squirrel in southwestern Virginia. J Parasitol. 1971; 57: 629.
- Kinsella JM, Robles Mdel R, Preisser WC. A review of Gongylonema spp. (Nematoda: Gongylonematidae) in North American rodents with description of a new species from the cotton rat, Sigmodon hispidus. Zootaxa. 2016; 4107: 277–284.
- Wells K, Gibson DI, Clark NJ, Ribas A, Morand S, McCallum HI. Global change in helminth parasite communities of wild mammals. Glob Change Biol. 2018; 24: 1–12.