
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 5
Endoscopic retrieval of a foreign body causing gastrojejunostomy obstruction in a patient with previous bariatric surgery
Hari Movva, MD1*; Lucia Soca-Gallego, DO1; Keegan Colletier, MD2; Brooke Corning, MD2
1Department of Internal Medicine, The University of Texas Medical Branch, USA.
2Division of Gastroenterology and Hepatology, The University of Texas Medical Branch, USA.
*Corresponding Author : Hari Mova
Department of Internal Medicine, The University
of Texas Medical Branch, USA.
Email: hamovva@utmb.edu
Received : Nov 06, 2025
Accepted : Dec 22, 2025
Published : Dec 29, 2025
Archived : www.jjgastro.com
Copyright : © Mova H (2025).
Abstract
Introduction: Foreign body ingestion, whether accidental or intentional, may result in serious complications such as impaction, perforation, or obstruction. While most ingestions resolve spontaneously, intentional cases often require endoscopic or surgical intervention. Patients with altered gastrointestinal anatomy—especially those with prior bariatric surgeries like Roux-en-Y gastric bypass—are at increased risk due to anatomical narrowing and altered motility. Although bezoars and strictures are known complications post-bariatric surgery, foreign body obstruction in this population is rarely reported. We describe a rare case of gastric bypass related obstruction caused by a suspected narcotic packet overlain by a food bezoar, managed endoscopically.
Materials and methods: A 49-year-old male with a history of morbid obesity, pernicious anemia, and Roux-en-Y gastric bypass presented with three months of nausea, vomiting, weight loss, and oral intake intolerance. Imaging showed gastric pouch dilation with a collapsed jejunum distal to the gastrojejunostomy, suggesting partial obstruction. The aim was to characterize the etiology and determine appropriate intervention. Esophagogastroduodenoscopy was performed for diagnosis and therapeutic management.
Results: Endoscopy revealed a healthy anastomosis with a large food bezoar obstructing the gastrojejunostomy. Upon removal, a latex balloon— suspected to be a narcotic body packet—was identified and extracted, resulting in complete resolution of obstructive symptoms. The patient’s condition improved post-procedure, and he was discharged without complications.
Discussion: This case highlights an unusual cause of gastrointestinal obstruction in a post-bariatric surgery patient. While bezoars and strictures are recognized complications, foreign body ingestion causing obstruction in this group is underreported. Endoscopic management was effective, though caution is warranted with suspected narcotic packets due to rupture risk. Strengths include diagnostic clarity and successful intervention without surgery. Limitations include lack of toxicological confirmation of packet contents.
Conclusion: This case emphasizes the importance of considering foreign body ingestion in bariatric patients with subacute obstructive symptoms. Endoscopic treatment remains a viable and effective option, potentially avoiding the need for surgical intervention.
Citation: Movva H, Soca-Gallego L, Colletier K, Corning B. Endoscopic retrieval of a foreign body causing gastrojejunostomy obstruction in a patient with previous bariatric surgery. J Gastroenterol Res Pract. 2025; 5(4): 1239.
Introduction
Foreign body ingestion is an endoscopic emergency that can be accidental or intentional. Most reports of foreign body inges tion pass through the Gastrointestinal (GI) tract spontaneously with only 10 percent requiring endoscopic removal and <1 per cent requiring surgery [1-3]. However, the literature suggests that in the case of intentional ingestion, up to 76 percent ne cessitate endoscopic intervention and nearly 16 percent require surgery [4].
Complications associated with foreign body ingestion include impaction, perforation, and obstruction. These complications can occur in any part of the GI tract, although most commonly in areas of angulation and narrowing, leading to increased risk in patients with pre-existing GI tract anatomic abnormalities, functional abnormalities, and prior GI tract surgery [5,6].
We describe the case of a 49-year-old male with a past medi cal history of morbid obesity and a remote history of Roux-en-Y gastric bypass 15-years prior who presented with subacute ob structive symptoms consisting of persistent vomiting and exces sive rapid weight loss. Diagnosis and treatment were performed through an upper Gastrointestinal (GI) endoscopy which re vealed a food bezoar overlying a foreign body, presumed to be a narcotic body packet.
The objective of this case presentation is to contribute to the current literature on endoscopic management and removal of foreign bodies composed of suspected narcotic body packets causing subacute obstructive symptoms in bariatric surgery pa tients. It is important for physicians to consider the different types of gastrointestinal foreign bodies that can cause obstruc tive symptoms in bariatric patients given the rise in morbid obesity and increased number of patients undergoing bariatric procedures.
Case report
This is a 49-year-old male with a past medical history of morbid obesity (Class III, weight 118 kg), pernicious anemia, asthma, seizure disorder, hypertension, and a surgical history remarkable for laparoscopic Roux-en-Y gastric bypass 15-years prior presenting with 3-months of persistent nausea, vomiting, poor oral intake, and 36 kg secondary weight loss. He also com plained of progressive oral intolerance to both solids and liq uids, and intermittent abdominal pain in his right and left upper quadrants.
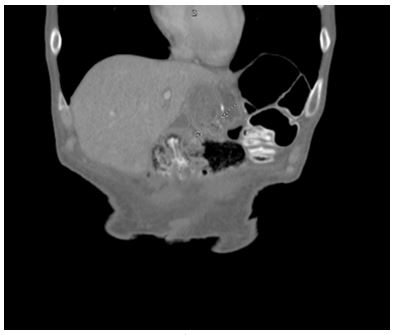
Imaging with CT abdomen pelvis with oral and IV contrast (Figures 1a, 1b) was remarkable for a dilated distal esophagus and gastric pouch with a relatively collapsed jejunum distal to gastrojejunostomy anastomosis suspicious for gastrojejunos tomy stenosis. The Gastroenterology (GI) service was consulted for further evaluation. GI suspected an acute presentation of a late complication of Roux-en-Y bypass causing obstructive symptoms possibly secondary to anastomotic stenosis or mar ginal ulcers and thus recommended further evaluation with en doscopy.

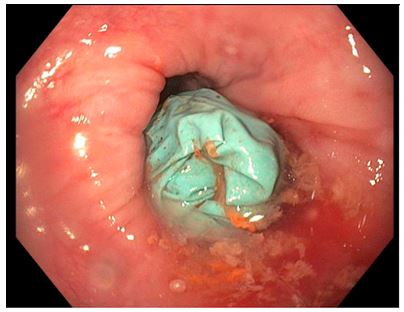
Upper Gastrointestinal (GI) endoscopic evaluation revealed evidence of Los Angeles Grade B esophagitis, gastrojejunal anastomosis with healthy mucosa, intact staple line at anas tomotic site, and what appeared to be a large food bezoar in the gastric body unable to pass the GJ anastomotic narrowing. Attempted retrieval of food residue revealed an underlying for eign body, which appeared to be a blue latex ball located in the gastric body causing the upstream obstruction (Figures 2 & 3). The foreign body was roughly 5 inches and was successfully re moved with a Roth net without complications. The rest of the endoscopic findings were unremarkable. On further interview ing, the patient admitted to having swallowed a foreign body approximately 5 months prior to presenting with these symp toms. Following successful removal of the foreign body (sus pected narcotic body packet), the patient clinically improved with increasing ability to tolerate PO intake and was discharged without complications.

Discussion
In the adult population, foreign body ingestion is a common clinical presentation classified according to the type of object ingested, location of object as determined by imaging, and clinical symptoms. Most ingested foreign bodies have a benign course, with 90% of cases passing through the Gastrointestinal (GI) tract spontaneously, 10% of cases requiring endoscopic re moval, and less than 1% requiring surgical intervention [5-7]. However, in the case of intentional ingestion, the literature sug gests that up to 76% necessitate endoscopic intervention and nearly 16% require surgery, making these cases more challeng ing to treat [4].
Most foreign body ingestions appear to be asymptomatic. Others are associated with complications including impaction, perforation, and obstruction. These complications can occur in any part of the GI tract, although most commonly in areas of angulation and narrowing, leading to increased risk in patients with pre-existing GI tract anatomic abnormalities, functional abnormalities, and prior GI tract surgery [5,6].
Bariatric surgery (e.g., sleeve gastrectomy and Roux-en-Y gastric bypass) is an excellent therapeutic strategy for the treat ment of obesity and metabolic syndrome [8]. These procedures effectively precipitate weight loss through restrictive and mal absorptive strategies or a combination of the two to promote reduction in gastric volume while bypassing portions of the small intestine to precipitate malabsorption of macronutrients [9].
While generally considered a safe and efficacious procedure, bariatric surgery leads to permanent alterations in gut physiolo gy that introduces a unique set of postoperative complications, both in the early postoperative period (<30 days) and the late postoperative period (>30 days), which can present acutely or chronically. Acute presentations of late complications include bleeding, perforations, and obstruction; most commonly sec ondary to anastomotic strictures, marginal ulceration, chronic leaks, fistulas. Other less common causes of obstruction in these patients include bezoars and intussusception [9,10]. For eign body ingestion is not a typical cause of obstruction in pa tients undergoing Roux-en-Y gastric bypass as shown in avail able literature.
Frequent clinical symptoms of obstruction in these patients include abdominal pain, distention, nausea, and vomiting. Oth er less frequent symptoms include weight loss and anorexia.
The management guidelines for most foreign body ingestion also applies to the bariatric patient, with specific indications pertaining to the specific types of ingested material. Endoscop ic removal appears to be the gold standard in management of most cases of foreign bodies and less frequently surgical remov al. In the case of narcotic drug packets, guidelines recommend against endoscopic removal and instead recommend conser vative management with laxatives with escalation to open or minimally invasive surgery to minimize the risk for rupture and leakage of the contents [11,12].
Conclusion
Here, we report a case of an adult patient who underwent laparoscopic bariatric surgery with Roux-en-Y gastric bypass 15 years earlier who presented with a foreign body (suspected narcotic packet) as the sole cause of GJ obstruction with sub acute complains of persistent vomiting, satiety, and weight loss, discovered during upper GI endoscopy and successfully treated with limited endoscopic manipulation. To our knowledge, this is the first reported case of successful endoscopic removal of a foreign object (suspected narcotic body packet) causing ob structive symptoms from the stomach of a bariatric patient.
Declarations
Author contributions: All authors have contributed substantially to the work.
Funding: This study was not supported by any external funding sources.
Competing interests: The authors have no conflicts of interest to report.
References
- Blero D, Devière J. Removing foreign bodies in bariatric patients. Tech Gastrointest Endosc. 2010; 12: 146–152.
- Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess. 2009; 13: 1–iv.
- Lim R, Beekley A, Johnson DC, Davis KA. Early and late complications of bariatric operation. Trauma Surg Acute Care Open. 2018; 3: e000219.
- Arterburn DE, Courcoulas AP. Bariatric surgery for obesity and metabolic conditions in adults. BMJ. 2014; 349: g3961.
- Liu Q, Liu F, Xie H, Dong J, Chen H, Yao L. Emergency removal of ingested foreign bodies in 586 adults at a single hospital in China according to the European Society of Gastrointestinal Endoscopy recommendations: a 10-year retrospective study. Med Sci Monit. 2022; 28: e936463.
- Birk M, Bauerfeind P, Deprez PH, et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy clinical guideline. Endoscopy. 2016; 48: 489–496.
- Blero D, Devière J. Removing foreign bodies in bariatric patient. Tech Gastrointest Endosc. 2010; 12: 146–152.
- Sherman A, Zingler BM. Successful endoscopic retrieval of a cocaine packet from the stomach. Gastrointest Endosc. 1990; 36: 152–154.
- Choudhary AM, Taubin H, Gupta T, Roberts I. Endoscopic removal of a cocaine packet from the stomach. J Clin Gastroenterol. 1998; 27: 155–156.
- Palta R, Sahota A, Bemarki A, Salama P, Simpson N, Laine L. Foreign-body ingestion: characteristics and outcomes in a lower socioeconomic population with predominantly intentional ingestion. Gastrointest Endosc. 2009; 69: 426–433.
- Conners GP, Mohseni M. Pediatric foreign body ingestion. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
- ASGE Standards of Practice Committee, Ikenberry SO, Jue TL, et al. Management of ingested foreign bodies and food impactions. Gastrointest Endosc. 2011; 73: 1085–1091.
- Negoita LM, Ghenea CS, Constantinescu G, Sandru V, Stan-Ilie M, Plotogea O-M, et al. Esophageal food impaction and foreign object ingestion in gastrointestinal tract: a review of clinical and endoscopic management. Gastroenterology Insights. 2023; 14: 131–143.
- Mittal A, Amer K, Manoharan A, Hohenleitner J, Arrigo R. Endoscopic management of ingested narcotic substances: a case report and literature review. Cureus. 2022; 14: e25058.