
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 5
Abdominal erythema nodosum in Crohn’s Disease: A case report
Cyrine Louati1*; Ghada Gharbi1; Asma Ben Mohamed1; Manel Yakoubi1; Ghazi Laamiri2; Moufida Mahmoudi3; Amal Khsiba3; Mouna Medhioub3; Emna Chelbi4; Lamine Hamzaoui3
1University Hospital Assistant, Gastroenterology Department, Faculty of Medicine of Tunis, Taher Maamouri Hospital, Nabeul, Tunisia.
2University Hospital Assistant, General Surgery Department, Faculty of Medicine of Tunis, Taher Maamouri Hospital, Nabeul, Tunisia.
3Associate Professor, Gastroenterology Department, Faculty of Medicine of Tunis, Taher Maamouri Hospital, Nabeul, Tunisia.
4Associate Professor, Department of Anatomy and Pathological Cytology, Faculty of Medicine of Tunis, Taher Maamouri Hospital, Nabeul, Tunisia.
*Corresponding Author :Cyrine Louati
Gastroenterology Department, Faculty of medicine of
Tunis, Taher Maamouri Hospital, Nabeul, Tunisia.
Tel: 0021699536680;
Email: Cyrinelouati94@live.fr
Received : Oct 30, 2025
Accepted : Dec 19, 2025
Published : Dec 26, 2025
Archived : www.jjgastro.com
Copyright : © Louati C (2025).
Abstract
Introduction: Dermatological manifestations are recognized extraintestinal complications of inflammatory bowel disease (IBD). Erythema nodosum (EN) is the most common, typically located on lower-extremity sites. Abdominal localization remains exceptional.
Case presentation: We report the case of an 18-year-old patient with a history of stricturing ileocolonic Crohn’s disease and bilateral sacroiliitis. While receiving infliximab therapy, he developed a painful hypogastric mass, initially suspected to be a soft tissue abscess. Surgical excision followed by histopathological analysis confirmed the diagnosis of abdominal erythema nodosum. Clinical outcome was favorable with no recurrence under ongoing infliximab treatment.
Conclusion: This report underlines an unusual abdominal localization of EN in a Crohn’s disease patient. Biopsy remains crucial to establish the diagnosis and guide management
Keywords: Erythema Nodosum, Crohn, Location.
Citation: Louati C, Gharbi G, Asma Ben M, Yakoubi M, Laamiri G, et al. Abdominal erythema nodosum in Crohn’s disease: A case report. J Gastroenterol Res Pract. 2025; 5(4): 1238.
Introduction
Dermatological manifestations, involving either the skin or mucous membranes, may precede or occur during the course of inflammatory bowel disease (IBD). They may be directly or in directly associated with IBD and display heterogeneous clinical presentations. Although uncommon, they can be particularly misleading due to their marked clinical polymorphism [1]. Ery thema nodosum (EN) is the most frequent cutaneous manifes tation observed in IBD. Its prevalence is higher among patients with Crohn’s disease, affecting 5-15% of them [2], with a female predominance [3]. The most frequent presentation is palpable, subcutaneous nodules on the shins. Involvment of non-lower extremity sites rare and atypical [4]. We report here a case of abdominal erythema nodosum in a patient with Crohn’s dis ease.
Case presentation
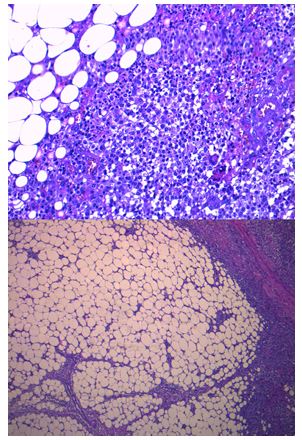
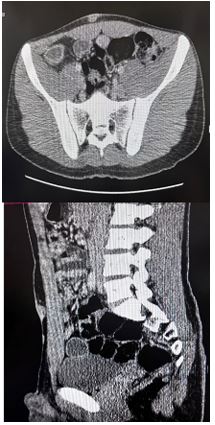
The patient was an 18-year-old male, followed since the age of 12 for stenosing ileocolonic Crohn’s disease associated with extraintestinal manifestations, namely bilateral stage three sac roiliitis. He was receiving infliximab at 5 mg/kg every 8 weeks. Clinically, the patient reported one to two well-formed stools per day. He complained of hypogastric abdominal pain. On ab dominal examination, a 2 cm slightly tender hypogastric soft tissue mass was detected, with normal overlying skin. Soft tis sue ultrasound suggested a localized collection. The abdomi nal CT scan showed diffuse thickening of the subcutaneous adipose tissue of the anterior abdominal wall, associated with ill-defined areas of increased density. The patient underwent surgical excision of the mass. Histopathology showed a dense inflammatory infiltrate composed of histiocytes, lymphocytes, plasma cells, and numerous neutrophils, associated with septal panniculitis. Immunohistochemistry revealed mild to moderate macrophagic (CD68+) and T lymphocytic infiltration, predomi nantly septal. These findings confirmed acute hypodermal in flammatory changes consistent with erythema nodosum. The patient continued his scheduled infliximab infusions. The post operative course was favorable, with complete wound healing and no recurrence.
Table 1: Past reports.
| Site of lesion | Number of cases | Details | Reference |
|---|---|---|---|
| Upper extremities | 4 | Histologically confirmed EN on arms and forearms | Perez-Chua T et al. [6] |
| Trunk | 2 | Lesions on chest and back; classic septal panniculitis | Perez-Chua T, et al. [6] |
| Face | 1 | Extremely rare; confirmed histopathologically | Perez-Chua T, et al. [6] |
| Forearms | Not quantified | Mentioned as atypical site in clinical reviews | Mert el al. [7] |
| Sarcoidosis-associated EN | Not quantified | Atypical distribution in systemic disease | Medina L. D [8] |
Discussion
Erythema nodosum is an extraintestinal manifestation directly related to IBD and represents a subtype of panniculitis [5]. It typically presents as tender, erythematous nodules ranging from deep red to violaceous, symmetrically distributed over the pretibial areas. Less commonly, lesions may appear on non-lower-extremity sites such as the upper limbs, trunk or face. Abdominal localization is exceptional, making diagnosis more challenging. A subsequent literature review of EN in non lower extremity (LE) sites identified some case reports, with histopathology confirmation (Table1). Our case is the first case of Abdominal location of Erythema Nodosum.
Usually, the overlying skin over nodes shows neither suppu ration nor ulceration, and the lesions evolve toward a yellowish, bruise-like discoloration before resolving spontaneously within six weeks. The eruption may be associated with fever, synovitis, or arthritis [4]. The differential diagnosis of EN includes other forms of panniculitis, cutaneous infections, and subcutaneous lymphomas [4]. Histopathological examination is characteristic and essential when diagnostic uncertainty arises, as in our case, where the diagnosis was confirmed by resection histology. It typi cally demonstrates septal panniculitis with subcutaneous septal infiltration by lymphocytes and predominantly neutrophils, lat er evolving toward fibrosis and macrophage predominance [9]. The pathophysiology of EN remains poorly understood. It may involve dysregulated intestinal immune responses extending beyond the gut, altered trafficking of immune cells, and distur bances of the intestinal microbiota. A genetic predisposition may also play a role [10]. EN in IBD usually parallels disease ac tivity. However, in our patient, it occurred despite clinical and endoscopic remission. Given the usually limited nature of le sions, symptomatic management with compression bandages or analgesics is often sufficient [11,12]. In severe or refractory cases, oral corticosteroids (prednisone 20 mg/day for 7–10 days) may be considered [12,13]. For patients with active IBD and treatment-resistant EN, anti-TNF therapy may be effective, with reported response rates of up to 80% [14]. Several case re ports have also highlighted the efficacy of infliximab and adali mumab at standard, non-optimized IBD doses [15,16]. Never theless, in our patient, EN developed despite ongoing infliximab therapy and in the absence of a disease flare. More recently, monoclonal antibodies targeting the IL-12/23p40 subunit have shown efficacy in EN. A multicenter study reported four com plete and one partial remission among five patients treated with ustekinumab [17].
Conclusion
Erythema nodosum is an extraintestinal cutaneous manifes tation directly associated with IBD. It most commonly affects the anterior legs, while non-lower-extremity sites remains ex ceptional. Ou case is the first case report in the literature of abdominal Erythema Nodosum in Crohn’s Disease. This rare presentation should be considered in Crohn’s disease patients, and biopsy of atypical nodules is recommended when diagnos tic uncertainty exists.
References
- Thrash B, Patel M, Shah KR, Boland CR, Menter A. Cutaneous manifestations of gastrointestinal disease: part II. J Am Acad Dermatol. 2013; 68(2): 211.e1-33; quiz 244-6.
- Veloso FT, Carvalho J, Magro F. Immune-related systemic manifestations of inflammatory bowel disease. A prospective study of 792 patients. J Clin Gastroenterol. 1996; 23(1): 29-34.
- Turkcapar N, Toruner M, Soykan I, Aydintug OT, Cetinkaya H, Duzgun N, et al. The prevalence of extraintestinal manifestations and HLA association in patients with inflammatory bowel disease. Rheumatol Int. 2006; 26(7): 663-8.
- Timani S, Mutasim DF. Skin manifestations of inflammatory bowel disease. Clin Dermatol. 2008; 26(3): 265-73.
- Antonelli E, Bassotti G, Tramontana M, Hansel K, Stingeni L, Ardizzone S, et al. Dermatological Manifestations in Inflammatory Bowel Diseases. J Clin Med. 2021; 10(2): 364.
- Perez-Chua T, Miller DD, Mahalingam M. Erythema nodosum of non-lower-extremity sites: a histopathologic reappraisal. G Ital Dermatol Venereol. 2016; 151(6): 710-3.
- Mert A, Ozaras R, Tabak F, Pekmezci S, Demirkesen C, Ozturk R. Erythema nodosum: an experience of 10 years. Scand J Infect Dis. 2004; 36(6-7): 424-7.
- L. D. M, M. J. V, D. C. C, C. E. B. Sarcoidosis presenting as erythema nodosum. International Journal of Case Reports and Images (IJCRI). 2018;9. Available from: http://www.ijcasereportsandimages.com/archive/2018-articles/2018100078Z01MD-medina/index.php
- Requena L, Yus ES. Panniculitis. Part I. Mostly septal panniculitis. J Am Acad Dermatol. 2001; 45(2): 163-83; 184-6.
- Kim JM, Cheon JH. Pathogenesis and clinical perspectives of extraintestinal manifestations in inflammatory bowel diseases. Intest Res. 2020; 18(3): 249-64.
- Blake T, Manahan M, Rodins K. Erythema nodosum - a review of an uncommon panniculitis. Dermatol Online J. 2014; 20(4): 22376.
- Pagani K, Lukac D, Bhukhan A, McGee JS. Cutaneous Manifestations of Inflammatory Bowel Disease: A Basic Overview. Am J Clin Dermatol. 2022; 23(4): 481-97.
- Greuter T, Navarini A, Vavricka SR. Skin Manifestations of Inflammatory Bowel Disease. Clin Rev Allergy Immunol. 2017; 53(3): 413-27.
- Vavricka SR, Gubler M, Gantenbein C, Spoerri M, Froehlich F, Seibold F, et al. Anti-TNF Treatment for Extraintestinal Manifestations of Inflammatory Bowel Disease in the Swiss IBD Cohort Study. Inflamm Bowel Dis. 2017; 23(7): 1174-81.
- Clayton TH, Walker BP, Stables GI. Treatment of chronic erythema nodosum with infliximab. Clin Exp Dermatol. 2006; 31(6): 823-4.
- Ortego-Centeno N, Callejas-Rubio JL, Sanchez-Cano D, Caballero-Morales T. Refractory chronic erythema nodosum successfully treated with adalimumab. J Eur Acad Dermatol Venereol. 2007; 21(3): 408-10.
- Phillips FM, Verstockt B, Sebastian S, Ribaldone D, Vavricka S, Katsanos K, et al. Inflammatory Cutaneous Lesions in Inflammatory Bowel Disease Treated With Vedolizumab or Ustekinumab: An ECCO CONFER Multicentre Case Series. J Crohns Colitis. 2020; 14(10): 1488-93.