
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 5
Hepatocellular carcinoma with bile duct invasion masquerading as obstructive hilar cholangiocarcinoma - diagnosed via spyglass cholangioscopy
Yasamin Rastgar, BS1*; Hari Movva, MD2; Ethan Glass, BS1; Reema Patel, MD2; Mushtaq Muhammad, MD3
1School of Medicine, University of Texas Medical Branch, Galveston, Texas, USA.
2Department of Internal Medicine, University of Texas Medical Branch, Galveston, Texas, USA.
3Divison of Gastroenterology, Division of Internal Medicine, University of Texas Medical Branch, Galveston, Texas, USA.
*Corresponding Author : Yasamin Rastgar
School of Medicine, University of Texas Medical Branch, Galveston, Texas, USA.
Email: yarastga@utmb.edu & yas.ras2000@gmail.com
Received : Sep 24, 2025
Accepted : Nov 03, 2025
Published : Nov 10, 2025
Archived : www.jjgastro.com
Copyright : © Rastgar Y (2025).
Abstract
Hepatocellular Carcinoma (HCC) is a common primary tumor of the liver, but invasion into the biliary tree is rare. We present a case of a 68-year-old male with decompensated cirrhosis who developed obstructive jaundice and was found to have a hilar mass concerning for cholangiocarcinoma. SpyGlass cholangioscopy revealed an intraductal lesion, and SpyBite confirmed HCC. This case presents the diagnostic challenges of Intraductal HCC (IDHCC) given its similarity with cholangiocarcinoma, and SpyGlass and SpyBite technology being utilized for a diagnosis.
Citation: Rastgar Y, Movva H, Glass E, Patel R, Muhammad M. Hepatocellular carcinoma with bile duct invasion masquerading as obstructive hilar cholangiocarcinoma - diagnosed via spyglass cholangioscopy. J Gastroenterol Res Pract. 2025; 5(4): 1237.
Introduction
Hepatocellular Carcinoma (HCC) is a primary tumor of the liver and accounts for approximately 90% of all liver tumors [1]. Risk factors for HCC are well established and include etiologies that result in cirrhosis, such as Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), alcohol abuse, and Metabolic Associated Steatotic Liver Disease (MASLD) [2,3]. In 2024, the American Cancer Society and National Center for Health Statistics estimated 41,630 new cases of liver and bile duct malignancies in the United States (US), which is a marked increase compared to previous decades [4]. Liver and bile duct malignancies are the fifth leading cause of cancer-related deaths in men and the seventh for women in the US [4]. The age distribution of HCC incidence has also shifted, with the greatest proportional increases in the 45-60 year old group [5]. Southern states show higher rates of incidence and mortality, with Texas, Louisiana, and Mississippi having some of the highest rates in the US [5]. HCC typically progresses along an indolent course, with symptoms mostly related to the underlying disease like cirrhosis or hepatitis. Diagnosis based on symptoms is rare since patients are usually asymptomatic until the disease is advanced. As a result, diagnosis relies heavily on screening of high-risk individuals.
HCC presenting as obstructive jaundice is uncommon, with an incidence reported between 1.2 to 9% [1,6] . However, obstructive jaundice due to HCC invasion of the biliary tree is even rarer. A review of 5,000 bile duct brushings over 20 years identified only 17 with HCC, and these are associated with a poor prognosis [ 6-8] . We present such a case of obstructive jaundice due to Intraductal HCC (IDHCC) diagnosed via SpyBite biopsy, with imaging initially suspicious of cholangiocarcinoma.
Case report
A 68-year-old male with a medical history of decompensated cirrhosis due to remote alcohol use disorder with ascites, type 2 diabetes mellitus, and hypertension presented to the emergency department with week-long epigastric pain, jaundice, decreased oral intake, and intermittent nausea and vomiting. Physical exam revealed epigastric tenderness, scleral icterus, and jaundice. Initial labs were significant for lipase 1,439 U/L, alkaline phosphatase 206 U/L, total bilirubin 10.3 mg/dL, conjugated bilirubin 5.0 mg/dL, unconjugated bilirubin 2.4 mg/dL, ALT 85 U/L, AST 109 U/L and AFP 3,150 ng/mL. Imaging including a CT abdomen and pelvis and a right upper quadrant ultrasound demonstrated intrahepatic biliary dilation, cholelithiasis, a cirrhotic liver, and a suspicious underlying liver mass. The common bile duct was dilated to 11 mm, raising concern for possible choledocholithiasis. Of note, the patient had a recent hospital admission 2 months prior for hepatic encephalopathy due to medication noncompliance with a notable AFP level of 2,920 ng/mL, raising concern for HCC. The patient was admitted and treated for possible gallstone pancreatitis with bowel rest, intravenous fluids, and continued on his home regimen of rifaximin. Surgery was consulted for cholecystectomy evaluation, which was deferred pending further evaluation of the unknown liver mass.
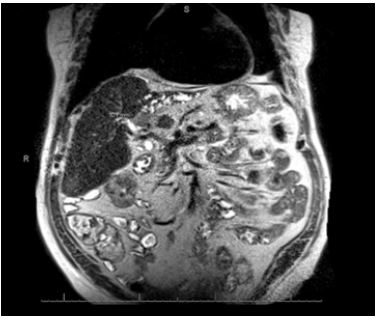
The gastroenterology service was consulted on hospital day 3 for evaluation of cirrhosis and new-onset obstructive jaundice. By this time, the patient’s abdominal pain had resolved, and his conjugated bilirubin had fallen to 2.3 mg/dL, indicating a possible passed stone. Magnetic Resonance Cholangiopancreatography (MRCP) was ordered for further workup of the liver mass and revealed an ill-defined, hypoenhancing mass at the liver hilum, with isolated left intrahepatic biliary dilatation and lobar atrophy (Figure 1).
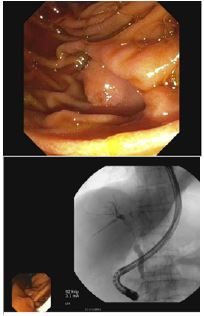
The enhancement characteristics and location were most suspicious for cholangiocarcinoma. The patient was discharged from the hospital and scheduled for Endoscopic Retrograde Cholangiopancreatography (ERCP) the following week. The patient underwent ERCP with Endoscopic Ultrasound (EUS) which demonstrated a 3 cm intraductal hilar mass extending to the right hepatic duct (Figures 2 & 3).
SpyGlass cholangioscopy with SpyBite biopsy was performed to obtain the specimen, which revealed malignant cells consistent with moderately differentiated hepatocellular carcinoma. This patient was discussed with a multidisciplinary tumor board and was deemed a possible candidate for liver transplantation. He was promptly referred to an outside institution that performed liver transplantations. Unfortunately, the patient had an acute decompensation and passed away before his evaluation could be completed.
Discussion/Conclusion
HCC occurs in approximately 85% of patients with cirrhosis. The most common sites of HCC metastasis include the lungs, intra-abdominal lymph nodes, bones, and adrenal glands [1]. Rarely, it can metastasize to a neoplasm of the biliary tract and be termed an icteric HCC, with a subset being IDHCCs.
Icteric HCC presents with most patients experiencing repeated bouts of jaundice and right upper quadrant pain. This mechanical obstruction of the bile duct can be attributed to continuous tumor growth, a fragment of necrotic tumor migrating, or hemorrhage from the primary tumor causing blood clots. In contrast to cholangiosarcoma, icteric HCC cannot solely be treated by biliary drainage [6], which is why their differentiation is imperative. The incidence of icteric HCC ranges from 0.5% to 13% of patients with HCC, with environmental and genetic factors cited for the difference. This complication of HCC is rare in Western countries which makes its diagnosis more difficult [7]. Icteric HCC can be further divided into intrahepatic and extrahepatic types, with an extrahepatic biliary obstruction having a better survival outcome [8].
Diagnosis of IDHCC includes the presence of elevated AFP levels (>20 ng/mL). In conjunction with this value, patients may have a positive hepatitis B surface antigen, elevated GGT levels (>60 U/L), and a rapid rise in bilirubin levels that directly correlate with AFP levels [7]. IDHCC can be detected with abdominal ultrasound, which can be used as an initial diagnostic tool and identify a tumor thrombus of bile ducts. Tumor thrombi can also be identified by an infusion of Lipiodol followed by an abdominal CT. In some cases, the location and cause of the obstruction remain unclear, and other diagnostic tools are adopted. Percutaneous Transhepatic Cholangiography (PCT) and ERCP can be used to categorize cholangiographic features and provide differential diagnoses that include cholangiocarcinoma, intraductal polyps, or mucin-hypersecreting intrahepatic biliary neoplasms [6]. MRCP is a noninvasive method with a sensitivity value of up to 95% for detecting biliary and pancreatic dilations or strictures, and accounts as a diagnostic tool for icteric HCC [6].
IDHCC can present with painless or painful jaundice with elevated liver enzymes [6] . Cytologic or tissue diagnosis by ERCP has limited sensitivity and may fail to differentiate between various etiologies like cholangiocarcinoma and Bile Duct HCC (BDHCC), leading to potential misdiagnoses. Direct biopsy via SpyGlass for cholangiocarcinoma has a sensitivity of 66% and specificity of 97%, with the sensitivity rising to 74% if past brushings or cytology were negative. This method is useful to distinguish benign from malignant disease, especially in cases where prior imaging is equivocal or misleading [9]. Our case highlights a presentation of HCC as obstructive jaundice with invasion of the bile duct, and the utility of direct cholangioscopy with biopsy to confirm the diagnosis of intraductal lesions, especially in the setting of discordance between serum tumor markers and imaging findings with crucial implications for prognosis and treatment.
Prognosis and outcome of this disease is usually poor, with a common cause of death being cholangitis [7]. In intraductal tumors, the fragments should be removed by choledochotomy in addition to a liver resection of the neoplasm [8]. Histology should be reviewed on bile duct debris to confirm metastasis from a hepatic origin [6]. When the tumor is deemed inoperable, efforts turn toward palliative care. If hepatic function is preserved, Transcatheter Arterial Embolization (TACE) should be used as first-line therapy [8]. Ultrasound-guided localized radiotherapy is an adjuvant management to those with poor liver function or those unresponsive to TACE [8].
References
- Asafo-Agyei KO, Samant H. Hepatocellular carcinoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2024.
- Chan WK, Chuah KH, Rajaram RB, Lim LL, Ratnasingam J, Vethakkan SR. Metabolic dysfunction-associated steatotic liver disease (MASLD): a state-of-the-art review. J Obes Metab Syndr. 2023; 32: 197–213.
- Gilles H, Garbutt T, Landrum J. Hepatocellular carcinoma. Crit Care Nurs Clin North Am. 2022; 34: 289–301.
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024; 74: 12–49.
- El-Serag HB, Kanwal F. Epidemiology of hepatocellular carcinoma in the United States: where are we? Where do we go?. Hepatology. 2014; 60: 1767–75.
- Chen MF. Icteric type hepatocellular carcinoma: clinical features, diagnosis and treatment. Chang Gung Med J. 2002; 25: 496–501.
- Huang JF, Wang LY, Lin ZY, Chen SC, Hsieh MY, Chuang WL, et al. Incidence and clinical outcome of icteric type hepatocellular carcinoma. J Gastroenterol Hepatol. 2002; 17: 190–5.
- Chen HW, Wang FJ, Li JY, Lai ECH, Lau WY. Hepatocellular carcinoma presenting with obstructive jaundice during pregnancy. Case Rep Surg. 2014; 2014: 502061.
- Navaneethan U, Hasan MK, Lourdusamy V, Njei B, Varadarajulu S, Hawes RH. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: a systematic review. Gastrointest Endosc. 2015; 82: 608–14.