
Journal of Gastroenterology Research and Practice
Clinical Image - Open Access, Volume 5
Gallbladder torsion: Clinical image
Xian-Zheng Tan*; Chong Chen
Department of Radiology, Hunan Provincial People’s Hospital and the First Affiliated Hospital of Hunan Normal University, China.
*Corresponding Author : Xian-Zheng Tan
Department of Radiology, Hunan Provincial People’s Hospital and the First Affiliated Hospital of Hunan Normal University, No. 61 Jiefang West Road, Changsha 410005, Hunan, China.
Email: xianzhengtan@163.com
Received : Sep 22, 2025
Accepted : Oct 27, 2025
Published : Nov 03, 2025
Archived : www.jjgastro.com
Copyright : © Xian-Zheng T (2025).
Keywords: Gallbladder torsion; Computed tomography; Whirlpool sign.
Citation: Xian-Zheng T, Chong C. Gallbladder torsion: Clinical image. J Gastroenterol Res Pract. 2025; 5(3): 1236.
Description
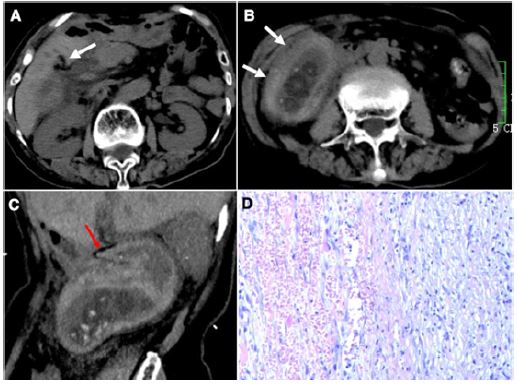
An 85-year-old woman presented with progressive abdominal pain and vomiting for 4 days. Her past medical history was unremarkable. On physical examination, she had tenderness in the right lower quadrant of the abdomen without rebound or guarding. Laboratory test showed a slightly elevated white cell count of 10.5×109/L with 84.3% neutrophils. Urgent non-contrast Computed Tomography (CT) scan of the abdomen revealed a conspicuous “whirl” sign at the the cystic pedicle, a distended and horizontally displaced gallbladder with a thickened, hyperattenuating wall, and an abrupt angulation of gallbladder neck (Figure 1A-1C). At emergency laparotomy, the gallbladder was gangrenous and rotated around its pedicle in a 540° clockwise manner. De-torsion and cholecystectomy were performed. Histologic examination showed extensive transmural hemorrhagic necrosis (Figure 1D). The patient recovered well postoperatively.
Discussion
Gallbladder torsion, usually occurring in elderly women, is a rare abdominal emergency with a reported mortality up to 6% [1]. Early diagnosis is the key to preventing potentially fatal sequelae, such as gallbladder perforation. The clinical presentation is often non-specific, which makes this condition easily confused with acute abdomen. Just like our case, gallbladder torsion mimics the clinical picture of appendicitis owing to the lower position of gallbladder. Although it is rare, clinicians must remain alert to the possibility of gallbladder torsion in those patients with right lower quadrant pain [2]. CT is recommended if this pathology is suspected. This patient portrays classic CT signs: (1) a “whirl sign” pathognomonic for gallbladder torsion; (2) diffusely thickened wall with haemorrhage, indicating gangrenous cholecystitis secondary to vascular compromise [3,4].
Author declarations
Conflict of interest statement: The authors declare no conflicts of interest.
Data availability statement: Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Informed consent: Written informed consent has been obtained from the patient. This is held by the corresponding Author together with the Patient's medical record, and is available upon request.
Acknowledgments: This work is supported by the Youth Medical Key Talents Foundation of Hunan Province (grant 20230508-1034).
References
- Reilly DJ, Kalogeropoulos G, Thiruchelvam D. Torsion of the gallbladder: a systematic review. HPB (Oxford). 2012; 14: 669–72.
- Tian T, Hojman H. Gallbladder volvulus. N Engl J Med. 2022; 387: 640.
- Borde P, Vilgrain V. Gallbladder volvulus. Radiology. 2021; 301: 43.
- Mashayekhi R, Kearns C, Enea M, Avalos F, Paez-Carpio A. Gallbladder torsion. Radiographics. 2024; 44: e240019.