
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 5
Unveiling the hidden toll: Disparities in Crohn’s disease mortality – Insights from a CDC WONDER study
Bipneet Singh1*; Muhammad Hashim Faisal2; Inshrah Qureshi3; Musab Maqsood4; Muhammad Shahzaib5; Luqman Munir6; Muhammad Ammar Ur Rahman7; Amna Khalid8; Muhammad Khan Buhadur Ali9
1Henry Ford Jackson Health, Health system located in Jackson, Michigan, USA.
2King Edward Medical University, University in Lahore, Pakistan.
*Corresponding Author : Bipneet Singh
Resident, Internal Medicine, Henry Ford
Jackson, 159 W Michigan Ave, Jackson, Michigan, USA.
Tel: +15174997929;
Email: drbipneetsingh18@gmail.com
Received : Jun 05, 2025
Accepted : Jun 25, 2025
Published : Jul 01, 2025
Archived : www.jjgastro.com
Copyright : © Singh B (2025).
Abstract
Introduction: Crohn’s disease is a chronic inflammatory bowel disease that can affect any part of the gastrointestinal tract, but it most commonly affects the end of the small intestine (ileum) and the beginning of the colon. According to the Centers for Disease Control and Prevention (CDC), Crohn’s disease is more commonly diagnosed among whites compared to African Americans, and our study set out to prove that.
Objectives: This study aims to uncover mortality trends due to Crohn’s disease across different age groups, races, ethnicities, urban and suburban areas, and census regions from 1999 to 2020. By analyzing age-adjusted mortality rates, we seek to identify inconsistencies in these epidemiological groups. While the incidence of Crohn’s disease among whites ranges from 3.1 to 14.6 per 100,000 person-years, it is significantly lower among African Americans, with 0.7 to 6.3 per 100,000 person-years, disparities among which our study aims to identify.
Methods: We analyzed Death Certificates from the Centers for Disease Control and Prevention (CDC) Wide Ranging Online Data for Epidemiological Research (WONDER) database from 1999-2020. AAMR per 1,000,000 people and Annual Percent Change (APC) with a 95% confidence interval were determined. We then used the Joinpoint Regression Program to obtain trends amongst epidemiological (race, ethnicity, gender, age) and demographic (census region, 2013 urbanization status) groups.
Results: From 2018 to 2020, age-adjusted mortality rates (AAMRs) due to Crohn’s disease have significantly increased, with an Annual Percentage Change (APC) of 11.18 (p=0.03). Most deaths occurred in medical inpatient facilities (AAPC=0.228), but home deaths have surged dramatically, showing an AAPC of 5.37 from 1999 to 2020. Both males and females experienced a significant rise in mortality post-2018, with APCs of 13.21 and 10.24, respectively. The Midwest had the highest mortality rates (APC 0.56, p=0.04), while the Northeast saw a decline in AAMRs from 1999 to 2017 (APC -1.25, p=0.000016) followed by a sharp increase from 2017 onward (APC 9.64, p=0.0071). Mortality among Whites was higher compared to African Americans/Blacks, reflecting the higher incidence and prevalence in Whites, but both groups saw remarkable increases in AAMRs after 2018, with APCs of 10.47 for Whites and 20.62 for African Americans. Mortality for Hispanics did not show a statistically significant change.
Conclusions: Crohn’s Disease-related mortality rates have experienced an uprise in the United States since 2018. Persistent demographic and geographic disparities in mortality due to Crohn’s disease especially the extremely wide gap in AAMR among Whites and African Americans underscore the need for further investigation and intervention to improve overall outcomes.
Citation: Singh B, Faisal MH, Qureshi I, Maqsood M, Shahzaib M, et al. Unveiling the hidden toll: Disparities in Crohn’s disease mortality – Insights from a CDC WONDER study. J Gastroenterol Res Pract. 2025; 5(2): 1230.
Introduction
Crohn’s disease is a chronic Inflammatory Bowel Disease (IBD) that can affect any part of the gastrointestinal (GI) tract, though it most frequently targets the end of the small intestine (ileum) and the beginning of the colon [1]. This complex condition is characterized by persistent inflammation that can lead to debilitating symptoms, including abdominal pain, diarrhea, fatigue, weight loss, and malnutrition. While the exact cause of Crohn’s disease remains unknown, a combination of genetic, environmental, and immune-related factors is believed to contribute to its development [2].
Epidemiological patterns reveal disparities in the prevalence and incidence of Crohn’s disease among different demographic groups. According to the Centers for Disease Control and Prevention (CDC), Crohn’s disease is more commonly diagnosed among white populations compared to African Americans [3]. The incidence rates among whites range from 3.1 to 14.6 per 100,000 person-years, whereas the rates among African Americans are significantly lower, estimated at 0.7 to 6.3 per 100,000 person-years [4,5]. These differences suggest underlying racial and ethnic disparities that may be linked to genetic predispositions, environmental exposures, healthcare access, or diagnostic biases.
To better understand these disparities, our study investigates mortality trends associated with Crohn’s disease over a 21-year period, from 1999 to 2020. By analyzing Age-Adjusted Mmortality Rates (AAMRs), we aim to identify patterns and inconsistencies across various demographic groups, including age, race, ethnicity, urban and suburban areas, and census regions. This analysis is critical to uncovering potential inequities in disease outcomes and advancing our understanding of how Crohn’s disease impacts different populations. Our research focuses on examining whether racial and ethnic disparities in the incidence of Crohn’s disease led to differences in mortality. It also explores the impact of geographic factors, such as urban versus suburban residency and regional variations, on disease outcomes. By addressing these issues, we aim to contribute to broader efforts to reduce health disparities and improve care for all individuals affected by Crohn’s disease.
Methodology
Study design
This study employs a retrospective design to conduct a database analysis of mortality trends using data from the CDC. The use of retrospective data enables a comprehensive examination of demographic trends, healthcare implications, and temporal shifts in mortality related to Crohn’s disease.
Data source
We obtained mortality data from the CDC WONDER (Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research) and analyzed Crohn’s disease-related deaths between 1999 and 2020. To identify cases, we utilized International Statistical Classification of Diseases and Related Health Problems-10th Revision (ICD-10) codes, including K50.0 (Crohn’s disease of the small intestine), K50.1 (Crohn’s disease of the large intestine), K50.8 (Other forms of Crohn’s disease), and K50.9 (Unspecified Crohn’s disease). This approach facilitatfacilitated an in-depth examination of mortality trends across different subtypes of Crohn’s disease over the study period.
Study population
This dataset included death certificate information from all 50 states and the District of Columbia. Gender-specific AAMRs (based on biological sex assigned at birth as male or female) were analyzed alongside race-specific data for Whites, African Americans, Hispanics or Latinos, Asian and Pacific Islanders, and Native Americans or Alaskans. The study used predefined ten-year age groups starting at age 15, with older adults classified as those aged 75 and above. The locations of death included medical facilities (such as inpatient, emergency room/outpatient, or death on arrival with status unknown), the decedent’s home, hospice facilities, and nursing homes/long-term care facilities. The population was assessed using the National Center for Health Statistics (NHS) 2013 U.S. census classification system, which categorized areas as urban (large central metropolitan areas with populations of ≥1 million) or rural (micropolitan areas with populations <50,000). Geographic regions were divided into Northeast, Midwest, South, and West, as defined by the U.S. Census Bureau.
Statistical methods
National trends in Crohn’s disease-related mortality were analyzed using crude and age-adjusted mortality rates (AAMRs) per 1,000,000 individuals from 1999 to 2020. Data were stratified by year, sex, race/ethnicity, state, ten-year age groups, place of death, and urban-rural status, with 95% Confidence Intervals (CIs). Only individuals with complete data were included in each analysis, and effective sample sizes are reported in the tables and figures. No adjustments were made for multiple comparisons or for missing data in the analysis.
To quantify annual trends in Crohn’s disease-related mortality, the National Cancer Institute’s (NCI) Joinpoint Regression Program (Joinpoint V 5.2.0.0) was used to determine the Annual Percent Change (APC) with 95% CI in AAMR employing the permutation test with parametric method which sequentially permutates the dataset approximately 4499 times to ensure that the approximate probability of overall Type I error is less than the specified significance level (also called the alpha level, default=.05). This gives a trend of AAMRs over the years with an APC value which is then used to describe the study results. APCs were classified as increasing or decreasing based on whether the slope of the mortality trend was significantly different from zero, determined through two-tailed t-tests. Statistical significance was defined as a p-value of less than 0.05.
We used the IBM Statistical Package for Social Sciences (SPSS V 27.0) to perform a non-parametric analysis of our dataset. The Mann-Whitney U test was employed for bivariate analysis to compare median Crohn’s disease mortality (e.g., gender), and the Kruskal-Wallis test was used for multivariate analysis of various parameters (e.g., race, age groups). We also performed post-hoc analysis using Dunn’s test of significance for each group. The p-values less than 0.05 were considered significant. Lastly, we used the STATA version 14.2 to calculate trends in mortality that we had initially calculated with the Joinpoint regression program and obtained a Z-value indicating an increasing or decreasing trend which was then compared and reported alongside the results. A p-value less than 0.05 was considered statistically significant.
Ethical considerations
This study was exempt from Institutional Review Board (IRB) approval as it utilized de-identified, publicly available data from a government-issued database. Additionally, the study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to ensure transparent and accurate reporting of the observed findings.
Results
Overview of mortality trends
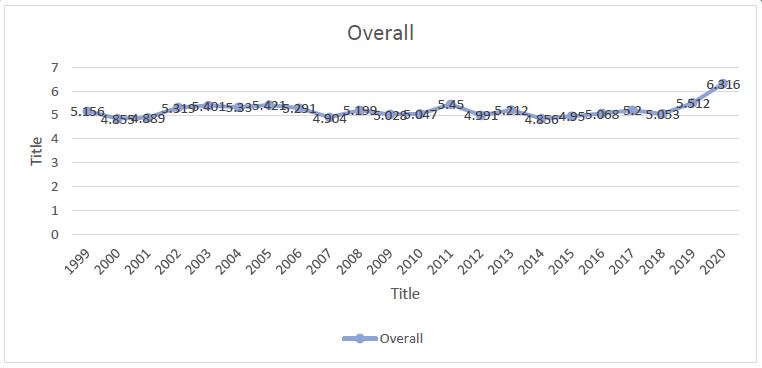
There was a total of 38,242 Crohn’s disease-related deaths from 1999 to 2020 which spiked from 2018 onwards with a significant APC value of 11.18 compared to a mere -0.14 throughout 1999 to 2018. The overall Average Annual Percent Change (AAPC) from 1999 to 2020 for Crohn’s disease mortality was 0.886 with a p-value of 0.05.
Subgroup analysis
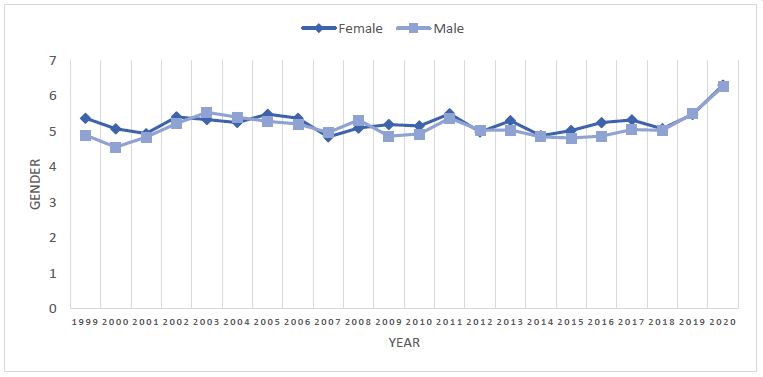
Gender-specific mortality: There were 21,604 deaths among females and 16,638 among males due to Crohn’s disease. The APC for females was -0.145 from 1999 to 2018, rising sharply to 10.238 between 2018 and 2020. For males, the APC showed different trends: 3.353 from 1999 to 2003, -0.573 from 2003 to 2018, and 13.214 from 2018 to 2020. The overall AAPC for the entire period (1999–2020) was 0.800 for females and 1.409 for males. Pairwise comparisons revealed no statistically significant differences.
Trend analysis in STATA indicated a z-value of -1.70 for the AAMRs of females and males, with a p-value of 0.089 (prob>z=0.089). The Mann-Whitney U test supported the null hypothesis that the AAMR distribution is consistent across genders, with a p-value of 0.089.
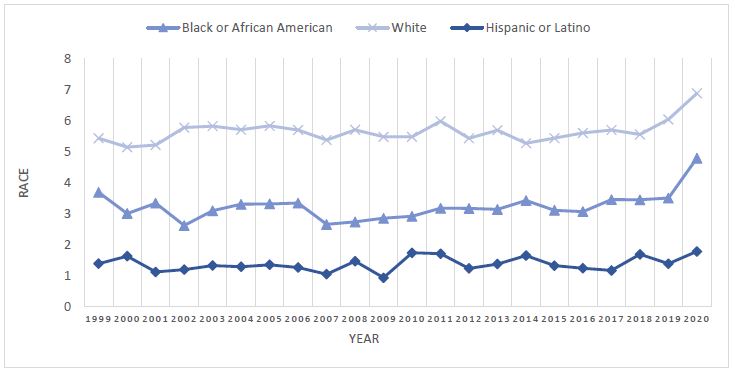
Race and ethnicity-specific mortality: Between 1999 and 2020, there were 127 Crohn’s disease-related deaths among American Indians and Alaskan Natives, 209 among Asians and Pacific Islanders, 2,564 among African Americans, and 35,342 among Whites. Hispanic/Latino deaths totaled 876. Due to unreliable data, the AAMR for American Indians and Alaskan Natives, as well as Asians and Pacific Islanders, was excluded from the analysis. Joinpoint analysis for African Americans showed an APC of 0.148 from 1999 to 2018 and 20.620 from 2018 to 2020. For Whites, the AAMR trend had an APC of 0.037 from 1999 to 2018 and 10.469 from 2018 to 2020. Among Latinos, the AAMR trend was relatively stable, with an APC of 0.903 throughout the period. Pairwise comparisons did not yield significant findings.
STATA trend analysis produced a z-value of 5.68 (p>z=0.000) for AAMRs across African Americans, Whites, and Latinos. The Mann-Whitney U test, comparing African Americans to Whites and Hispanic to Non-Hispanic groups, rejected the null hypothesis of equal AAMR distributions across groups, with a p-value of 0.000 for all comparisons.
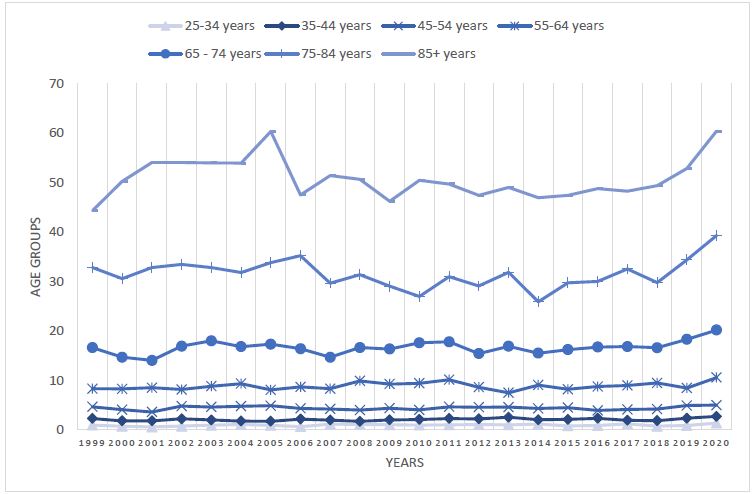
Age groups related mortality: Crude rate data for individuals aged 15 to 24 was inconsistent across most years and was therefore excluded from the analysis. The AAPC values for crude rates across different age groups were as follows: 1.203 for those aged 25 to 34, 0.862 for those aged 35 to 44, 0.117 for those aged 45 to 54, 0.438 for those aged 55 to 64, 1.055 (0.156 from 1999 to 2018 and 10.000 from 2018 to 2020) for those aged 65 to 74, 0.872 (-0.586 from 1999 to 2018 and 15.842 from 2018 to 2020) for those aged 75 to 84, and 0.611 (-0.529 from 1999 to 2018 and 12.127 from 2018 to 2020) for those aged 85 and older. Pairwise comparisons showed non-parallel results between the 25 to 34, 35 to 44, 45 to 54, and 55 to 64 age groups and the 65 to 74, 75 to 84, and 85+ age groups, indicating discrepancies in outcomes between younger to middle-aged adults and older adults. STATA analysis of crude rate trends produced a z-value of 12.24 (p>z=0.000). The Kruskal-Wallis test for independent samples rejected the null hypothesis of similar crude rate distributions across age groups with a p-value of 0.000. Additionally, the post-hoc Dunn’s test further validated the findings.
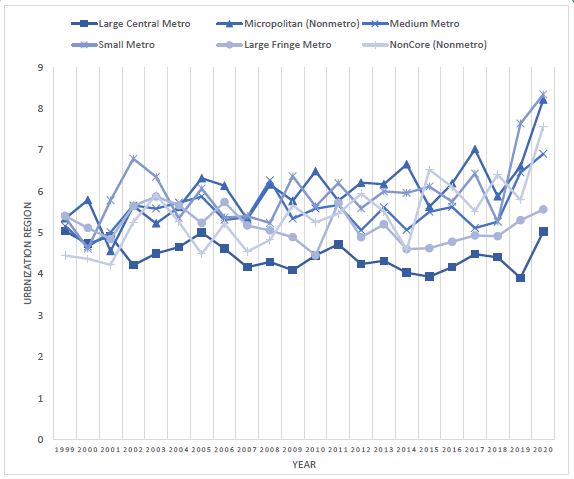
2013 Urbanization-specific mortality: From 1999 to 2020, the number of deaths related to Crohn’s disease were 9,112 in Large Central Metro, 9,091 in Large Fringe Metro, 8,597 in Medium Metro, 4,261 in Small Metro, 4,249 in Micropolitan (non-Metro), and 2,932 in non-Core (non-Metro) areas. AAMR trends from 1999 to 2020 were consistent across Large Central Metros, Large Fringe Metros, Micropolitans, and Non-Core areas, with AAPC values of -0.468, -0.374, 1.335, and 1.726, respectively. The AAPC for Medium Metro was 1.2515 (0.052 from 1999 to 2018 and 13.386 from 2018 to 2020), and for Small Metro, it was 2.0151 (0.327 from 1999 to 2018 and 19.598 from 2018 to 2020). Pairwise comparisons revealed significant (p<0.05) non-parallel trends between these groups: Large Central Metro and Small Metro, Large Central Metro and Micropolitan, Large Central Metro and Non-Core, Large Fringe Metro and Small Metro, Large Fringe Metro and Micropolitan, and Large Fringe Metro and Non-Core areas. The non-parametric trend test in STATA produced a z-value of 6.32 (p>z=0.00). The independent Kruskal-Wallis test with post-hoc Dunn’s test rejected the null hypothesis that “AAMR distribution is the same across Urbanization groups,” with a p-value of 0.000.
Place of death-related mortality: A total of 16,269 deaths occurred in inpatient medical facilities, 1,949 in outpatient/ER settings, 10,513 at the decedents’ homes, 2,057 at hospice facilities, 5,718 in nursing homes, and 1,497 at other or unknown locations. Joinpoint analysis of the death toll over the years showed AAPC values of 0.22 (with a decrease of -1.02 from 1999 to 2018 and an increase of 12.97 from 2018 to 2020) for inpatient medical facilities, 2.25 for outpatient/ER, 5.37 for decedents’ homes, 19.98 (with 66.98 from 2005 to 2007, 23.03 from 2007 to 2012, and 8.75 from 2012 to 2020) for hospice facilities, 1.08 for nursing homes, and 5.37 for other/unknown locations. The non-parametric trend test in STATA showed a z-value of -4.06 (p>z=0.000). The independent Kruskal-Wallis test, followed by post-hoc Dunn’s test, rejected the null hypothesis that “the distribution of AAMRs is the same across all death locations” with a p-value of 0.000.
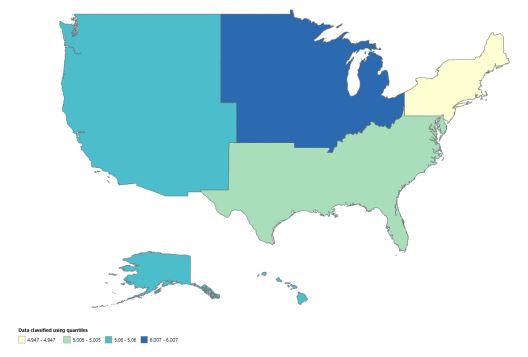
Mortality trends by census regions: The total number of deaths due to Crohn’s Disease from 1999 to 2020 was 7005 in the Northeast, 9792 in the Midwest, 13,372 in the South, and 8073 in the West census regions. AAMR trend with AAPC value in the Northeast was 0.233 (-1.254 from 1999 to 2017 and 9.642 from 2017 to 2020), the Midwest was 0.558, the South was 1.068 (0.094 from 1999 to 2018 and 10.799 from 2018 to 2020), and the West was 0.857 (0.039 from 1999 to 2018 and 8.959 from 2018 to 2020). The pairwise comparison did not yield any significant results.
The non-parametric test in STATA revealed a z-value of -4.33 (p>z=0.00). Independent samples Kruskal Wallis test rejected the null hypothesis “the distribution of AAMRs is same across Census regions” with a p-value of 0.000. Post-hoc Dunn’s test of significance supported the results. The US census regions heatmap based on mortality from Crohn’s disease is given below.
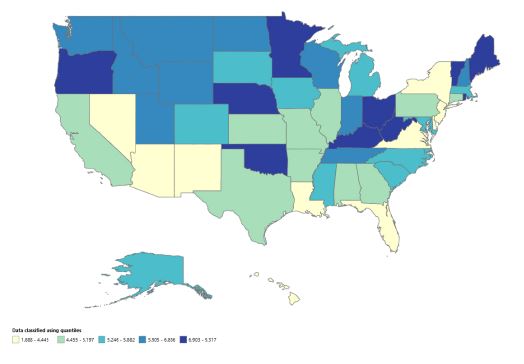
States with the highest mortality: The states with the highest Crohn’s disease-related mortality rates were California, Florida, Texas, Ohio, and New York with 3712, 2351, 2211, 2073, and 1983 deaths from 1999 to 2020, respectively. The US States heatmap based on mortality from Crohn’s disease is given below.
Discussion
The analysis of Crohn’s disease mortality trends from 1999 to 2020 shows a troubling increase in death rates, particularly after 2018, with an APC of 11.18 compared to a minimal -0.14 in the years before. This change prompts important inquiries into the factors behind the rising mortality and suggests the need for a deeper investigation into the underlying causes. A key factor could be the escalating severity of Crohn’s disease among patients. Studies indicate that the disease has become more aggressive over time, possibly influenced by environmental factors, dietary shifts, and lifestyle habits that exacerbate inflammation and complications related to Crohn’s disease [6,7]. For example, complications such as bowel obstructions, fistulas, and colorectal cancer are increasingly seen in long-term patients, which might explain the higher mortality rates [6,8]. Furthermore, the increasing occurrence of intestinal cancers in Crohn’s patients is concerning, as these cancers are commonly linked to higher mortality [8]. The timing of this surge in mortality aligns with the COVID-19 pandemic, which significantly disrupted healthcare services. Many patients with chronic conditions, including those with Crohn’s disease, experienced delays in their routine care. This disruption, combined with the pandemic’s exacerbation of existing health disparities, may have contributed to the rising death rates [7]. Additionally, the mental and emotional strain of the pandemic likely impacted patients’ mental health and their adherence to treatment, possibly further contributing to the increase in mortality.
Our study revealed that Crohn’s disease resulted in more female deaths than male deaths, with 21,604 women dying compared to 16,638 men. This supports broader patterns where female mortality from Crohn’s disease has historically been higher than male mortality [9]. Additionally, we observed a notable rise in mortality rates for both genders after 2018, with an APC of 10.238 for women and 13.214 for men. While the rate of increase is greater in men, the overall number of deaths remains higher for women. Research indicates that gender differences in Crohn’s disease prevalence differ by region, with women being more affected in North America and Europe, whereas men are more frequently affected in Asia [10]. Despite women having higher mortality rates, men tend to have more severe disease at younger ages [6]. Studies show that men are more likely to suffer from complications such as intestinal perforation, which may contribute to the higher mortality among younger men [11]. Conversely, hormonal factors and immune system differences may make women more susceptible to severe autoimmune responses [12]. Women are also more likely to experience extraintestinal manifestations, complicating disease management and increasing their mortality risk [12]. Thus, both genders face unique risks and challenges when managing Crohn’s disease.
The data highlights notable racial differences in Crohn’s disease mortality, with Whites experiencing the highest rates, followed by African Americans and Hispanics/Latinos. This aligns with earlier research indicating higher mortality among White individuals [6]. Whites are also more prone to complications such as structuring and penetrating disease, which are linked to worse outcomes and increased mortality [13,14]. Although African Americans may experience more severe disease in some cases, Whites tend to present with complications that are more challenging to manage [14]. The increasing APC values for both African Americans and Whites after 2018 suggest a negative trend, possibly influenced by changes in healthcare policies, socioeconomic challenges exacerbated by the COVID-19 pandemic, or alterations in disease management [14].
Additionally, the mortality rates associated with Crohn’s disease rise notably with age, with individuals aged 65 and above showing the highest rates [6]. This increase can be linked to the advancement of the disease, the presence of comorbidities, and the emergence of complications that are more prevalent in older individuals. Specifically, adults over 75 are at greater risk for serious complications such as bowel obstructions, perperforations, and colorectal cancer, all of which contribute to an elevated mortality risk [15]. The increase in APC values for this age group after 2018 further underscores this heightened risk.
Mortality rates for Crohn’s disease vary significantly depending on urbanization, with the highest rates found in Large Central and Large Fringe Metro areas. Studies suggest that urban settings are associated with higher incidence rates of IBD, including Crohn’s disease, due to environmental factors like diet, pollution, and lifestyle changes common in cities [16,17]. Urban living has been shown to increase exposure to various risk factors for gastrointestinal diseases, potentially worsening symptoms and complications [18]. Additionally, the environmental changes associated with urbanization may disrupt the gut microbiota, raising the likelihood of developing conditions like Crohn’s disease [18]. Additionally, most of the Crohn’s disease-related deaths occurred in inpatient medical facilities, indicating that many patients experience significant disease progression necessitating hospitalization [19,20]. The reliance on inpatient care underscores the severity of cases and the necessity for intensive medical intervention [19].
Our research reveals that the South experiences the highest number of Crohn’s disease-related deaths, followed by the Midwest, West, and Northeast. The South’s AAPC of 10.799 between 2018 and 2020 points to a concerning rise in mortality, likely linked to worsening disease management and disparities in healthcare access and socioeconomic factors [7]. The higher prevalence of risk factors like obesity and smoking in certain regions may exacerbate health outcomes [21]. Environmental influences such as diet and pollution also contribute to the severity and management of the disease [16]. In contrast, the Midwest and West show stable AAPC values, reflecting significant mortality but without the concerning increases seen in the South and Northeast. The absence of significant pairwise differences implies that similar underlying factors may be affecting mortality trends across these regions.
Limitations
This study has a few limitations, such as its dependence on mortality data, which might not completely reflect the full range of Crohn’s disease-related health complications. The regional data, when grouped together, may obscure local differences in healthcare access and treatment approaches. Additionally, the lack of detailed demographic information and treatment history limits our ability to fully understand the factors affecting mortality. Finally, although trends from 1999 to 2020 provide useful insights, they might not capture the latest changes in healthcare practices or treatment advancements.
Conclusion
In conclusion, Crohn’s disease mortality trends reveal concerning increases in death rates, particularly after 2018, likely due to the escalating severity of the disease, complications like bowel obstructions and colorectal cancer, and healthcare disruptions during the COVID-19 pandemic. Gender and racial disparities were also evident, with women experiencing higher mortality than men and Whites having the highest overall rates. Age and regional differences further influenced mortality, with older adults and those in urban or socioeconomically disadvantaged areas at greater risk. These findings highlight the need for further investigation into the underlying causes of these trends, including environmental, lifestyle, and healthcare factors, to improve disease management and patient outcomes. Future research should focus on addressing disparities in care, enhancing treatment strategies, and exploring the long-term effects of recent healthcare disruptions. Continued advancements in treatment options, including biological therapies and precision medicine, will be vital in improving outcomes for Crohn’s disease patients. Additionally, the collection of comprehensive demographic and treatment data is essential for developing targeted public health policies and interventions to reduce Crohn’s disease mortality in vulnerable populations.
References
- Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010; 105: 289-297.
- Liu JZ, Anderson CA. Genetic studies of Crohn’s disease: past, present and future. Best Pract Res Clin Gastroenterol. 2014; 28: 373-386.
- Dahlhamer JM, Zammitti EP, Ward BW, Wheaton AG, Croft JB. Prevalence of Inflammatory Bowel Disease Among Adults Aged ≥18 Years - United States, 2015. MMWR Morb Mortal Wkly Rep. 2016; 65: 1166-1169.
- Horsthuis K, Stokkers PC, Stoker J. Detection of inflammatory bowel disease: diagnostic performance of cross-sectional imaging modalities. Abdom Imaging. 2008; 33: 407-416.
- Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012; 142: 46-e30.
- Aziz S, Akhlaq A, Owings A, et al. Mortality Trends in Inflammatory Bowel Disease by Age, Sex, and Race in the United States from 1999 to 2020. Inflamm Bowel Dis. 2024.
- Merza N, Dahiya D, Dar SH, et al. S945 Crohn’s Disease Mortality Rates in the United States: Two Decades Analysis Based on US Death Certificates. The American Journal of Gastroenterology. 2023; 118: S709.
- Yasukawa S, Matsui T, Yano Y, et al. Crohn’s disease-specific mortality: a 30-year cohort study at a tertiary referral center in Japan [published correction appears in J Gastroenterol. 2021; 56: 1111-1112.
- Brant SR, Nguyen GC. Is there a gender difference in the prevalence of Crohn’s disease or ulcerative colitis? [published correction appears in Inflamm Bowel Dis. 2009 Sep;15(9):1438-47]. Inflamm Bowel Dis. 2008; 14: S2-S3.
- Park SB, Yoon JY, Cha JM. What Are the Different Phenotypes of Inflammatory Bowel Disease in Asia?. Gut Liver. 2022; 16: 676-685.
- Wagtmans MJ, Verspaget HW, Lamers CB, van Hogezand RA. Gender-related differences in the clinical course of Crohn’s disease. Am J Gastroenterol. 2001; 96: 1541-1546.
- Greuter T, Manser C, Pittet V, Vavricka SR, Biedermann L. on behalf of Swiss IBDnet, an official working group of the Swiss Society of Gastroenterology. Gender Differences in Inflammatory Bowel Disease. Digestion. 2020; 101: 98-104.
- Iqbal H, Haddadin R, Haidary H, et al. Racial and gender disparities in the development of Crohn’s disease complications: A retrospective analysis. Inflammatory Bowel Diseases. 2024; 30: S55.
- Burbage SC, Krupsky KL, Cambron-Mellott MJ, Way N, Patel AA, Liu JJ. Racial and Ethnic Disparities in Health-Related Outcomes in Crohn’s Disease: Results From the National Health and Wellness Survey. Crohns Colitis. 2024; 6: otae021.
- Canavan C, Abrams KR, Mayberry J. Meta-analysis: colorectal and small bowel cancer risk in patients with Crohn’s disease. Aliment Pharmacol Ther. 2006; 23: 1097-1104.
- Soon IS, Molodecky NA, Rabi DM, Ghali WA, Barkema HW, Kaplan GG. The relationship between urban environment and the inflammatory bowel diseases: a systematic review and meta-analysis. BMC Gastroenterol. 2012; 12: 51.
- Benchimol EI, Kaplan GG, Otley AR, et al. Rural and Urban Residence During Early Life is Associated with Risk of Inflammatory Bowel Disease: A Population-Based Inception and Birth Cohort Study published correction appears in Am J Gastroenterol. 2017; 112: 1485.
- Hui L. Quantifying the effects of aging and urbanization on major gastrointestinal diseases to guide preventative strategies. BMC Gastroenterol. 2018; 18: 145.
- Centers for Disease Control and Prevention. Hospitalization rates for Crohn’s disease among Medicare enrollees — United States, 2017. MMWR Morb Mortal Wkly Rep. 2019; 68: 1136-1140.
- Buie MJ, Coward S, Shaheen AA, et al. Hospitalization Rates for Inflammatory Bowel Disease Are Decreasing Over Time: A Population-based Cohort Study. Inflamm Bowel Dis. 2023; 29: 1536-1545.
- Zhou JL, Bao JC, Liao XY, et al. Trends and projections of inflammatory bowel disease at the global, regional and national levels, 1990-2050: a bayesian age-period-cohort modeling study. BMC Public Health. 2023; 23: 2507.