
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 5
Gastric dysmotility associated with untreated celiac disease in adults: A narrative review of measurement techniques and hormones disturbance
Aldisi Dara A, PhD*; Alolayan Rawan A, MSc
Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, Saudi Arabia.
*Corresponding Author : Aldisi Dara A
Assistant Professor in Clinical Nutrition, Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh-11433, Saudi Arabia.
Tel: +966(0)555410595;
Email: Rawanalolayan8@gmail.com
Received : Mar 10, 2025
Accepted : Apr 03, 2025
Published : Apr 10, 2025
Archived : www.jjgastro.com
Copyright : © Dara AA (2025).
Abstract
Gastric dysmotility is frequently present among newly diagnosed and untreated patients with celiac disease. Increasing healthcare providers’ awareness and diagnoses of gastric dysmotility, and examining hormones that play a key role in regulating gastric motility, can contribute to increasing the rate of patient detection, diagnosis, and treatment of CD. This review aims to provides an overview of the presence of gastric dysmotility using different techniques, and explores the impact of some hormone disturbances on gastric motility in adults with CD. A literature search for gastric dysmotility in celiac disease was conducted using the internet databases PubMed, Science Direct, Web of Science, Google Scholar, Cochrane, and Medline. Significant gastric motility delays were found in untreated patients with celiac disease using techniques such as ultrasound, C-octanoic acid breath test, and electrogastrography. In contrast, an insignificant delay in gastric motility was found using Echo-Planar MRI, Antro-duodenal manometry, and PillCam techniques. Studies showed that high levels of neurotensin, serotonin, and pancreatic polypeptide plasma hormones could explain the delayed gastric motility in patients with celiac disease. Conflicting results were found regarding ghrelin levels and their effect on delayed gastric motility. Further studies are needed to assess gastric motility using standardized, nutritionally balanced test meals, using more convenient and less invasive techniques in patients with celiac disease. Additionally, high-quality studies are required to resolve the conflicting results on ghrelin levels and their impact on gastric dysmotility. The inclusion of other hormones such as gastrin and irisin, that affect gastric motility should also be considered.
Keywords: Gastric emptying; Gastric motility; Gastric dysmotility; Gastroparesis; Dyspepsia; Functional Dyspepsia; Celiac disease; Hormone.
Abbreviations: CD: Celiac Disease; GI: Gastrointestinal; MRI: Magnetic Resonance Imaging; EGG: Electrogastrography.
Citation: Dara AA, Rawan AA. Gastric dysmotility associated with untreated celiac disease in adults: A narrative review of measurement techniques and hormones disturbance. J Gastroenterol Res Pract. 2025; 5(1): 1225.
Introduction
Celiac Disease (CD) is one of the most prevalent worldwide genetic diseases. Over the last two decades, CD diagnosis rates have tripled globally [1]. The seroprevalence and prevalence of CD are 1.4% and 0.7%, correspondingly [2]. CD is a permanent autoimmune enteropathy triggered by the ingestion of dietary gluten in individuals with specific genetic makeup and resolves with the exclusion of gluten from the diet [3]. The only management for CD is strict compliance with a gluten-free diet.
The high rates of CD globally result from the interplay between environmental factors: microbiome makeup [4], enteric viral infections [5], high wheat consumption [6], genetic factors: the presence of human leukocyte antigen HLA-DQ2 and/or HLA-DQ8holotypes, and other genes [7]. However, the trigger for CD is unknown. Almost the whole body may get affected by CD, with more than 200 different signs and symptoms.
Dysmotility-like dyspeptic symptoms are one of the most common complaints among patients with CD. In a systematic review and meta-analysis study conducted on patients complaining of dyspepsia, around 1.5% of them were diagnosed with CD [8]. When an endoscopy investigation shows no pathological cause, it is called functional dyspepsia. Functional dyspepsia was defined by the European Society for Neurogastroenterology and Motility as a long-lasting complaint of one or more symptoms, including heartburn, distressing upper abdomen distention, early satiety after meals, and post-prandial fullness [9]. Following a strict gluten-free diet can be potent in normalizing and improving gastric mobility among patients with CD [10].
The presence of gastric dysmotility in newly diagnosed patients with celiac disease is still a matter of debate [11-17]. In this review, we investigate the potential reasons behind the different outcomes regarding the presence or absence of gastric dysmotility in untreated patients with celiac disease. It has been hypothesized that different hormones such as neurotensin, serotonin, pancreatic polypeptide plasma, and ghrelin could play a key role in the etiology of gastric dysmotility. However, research in this field is still emerging, and additional research is required. We reviewed the association between neurotensin, pancreatic polypeptide plasma, serotonin and the presence of gastric dysmotility in untreated patients with celiac disease [11,17,18]. Moreover, we investigate the conflicting results regarding ghrelin levels and its effect on gastric dysmotility among the same patient’s population [14,17,19,20,21,22]. This review aims to provides an overview of the presence of gastric dysmotility using different techniques, and explores the impact of some hormone disturbances on gastric motility in newly diagnosed, untreated adults with CD.
Materials and methods
A comprehensive literature search was carried out on gastric motility in patients with CD was performed using internetdatabases: PubMed, Science Direct, Web of Science, Google Scholar, Cochrane, and Medline. All types of original research and reviews were included in the search. All articles were published in English, and in human adult populations, published between 2000 and Nov 2022. The references in the reviews published were also examined for extra articles. A total of 13 papers have been found and discussed. Figure 1 illustrates the flow chart of searched results. This review included gastric myoelectrical activity/ delayed gastric emptying; gastric motility/ gastric dysmotility, gastroparesis/ gastric stasis/ dyspepsia/ functional dyspepsia, celiac disease/ coeliac disease/ gluten enteropathy/ celiac Sprue, and hormones. Beside all the validated gastric motility techniques: Antro-duodenal manometry, C-octanoic acid breath test, ultrasound, Echo-Planar MRI, PillCam, and Electrogastrography. Additionally, all the hormones that affect gastric motility among patients with CD: neurotensin, ghrelin, pancreatic polypeptide plasma, and serotonin.To reduce selection bias and limit the heterogeneity of this review, we decided to exclude (1) animal studies; (2) children; (3) gastrointestinal disorders other than CD; (4) diabetes mellitus; (5) tobacco smoking; (6) alcohol abuse; (7) Intake of medications with known interference with gastric myoelectric activity and autonomic function (prokinetics and antiemetics drugs, narcotic agents, anticholinergic drugs, and nonsteroidal anti-inflammatory agents); (8) patients with a history of abdominal surgeries or chronic disorders.
Techniques that measure gastric motility disorders among patients with CD in different studies
Over the past few decades, the delayed gastric emptyingdisorder in adults with CD has been studied using a variety of techniques. In 2000, Bardella et al. [11] used ultrasound to assess the gastric activity in 9 newly diagnosed CD patients with positive duodenal biopsy and 9 controls with negative CD serology tests. The participants ate a high-fat trial meal after midnight fasting. The antral area of the stomach activity was determined using ultrasound 30 minutes before, immediately after, and then every 30 minutes. The researchers found a significant delay in gastric activity in patients with CD compared to the healthy controls (203±32 versus 133±15 min, P=0.0117). In 2005,Marciani et al. [12] used Echo-Planar MRI to study the gastric emptying rate among 15 untreated adults with CD and 15 healthy controls. After midnight fasting, they ate a trial thin liquid meal, a validated dyspepsia questionnaire was applied, and a Single-shot modulus-blipped echo-planar single-pulse technique was performed. In-evident delayed gastric emptying was found (P=0.142). Similar results were observed by Bassotti et al. in 2008, [13] where Antro-duodenal manometry was used to assess the antro duodenojejunal motility in CD patients and controls, including 11 newly diagnosed patients with celiac disease, 12 treated CD patients with a gluten-free diet for at least one year and a half, and 33 healthy control groups. All patients performed a duodenal biopsy, and an unvalidated symptoms questionnaire was completed. After midnight fasting, antroduodenojejunal activity was registered for 6 hours, after which the participants ate a balanced gluten-free trial meal and registered 3 hours of antro duodenojejunal activity. No significant delayed antroduodenal manometry activity was found in CD patients who abstained from food status (P=0.18) and post-prandial status (P=0.12). In the same year, 2008, Rocco et al. [14] used a C-octanoic acid breath test to study the gastric transit times for solids in 20 newly diagnosed CD patients and 10 controls with reflux symptoms. A validated dyspepsia questionnaire was administered, and a duodenal biopsy was obtained from all study subjects. The participants ate the high-fat test meal, and the respiratory samples were collected pre-prandial and then every 15 minutes for 4 hours post-prandial. They found gastric emptying was significantly delayed in all patients with CD (t1/2=252±101 min; P<0.005). In another study of a larger group of CD patients in 2013, Urgesi et al. [15 used PillCam to study the gastric emptying rate in 30 newly diagnosed adults with CD and 30 healthy matched control. Duodenal biopsies were obtained from all study subjects; after a bowel preparation and overnight fasting, they took the capsule endoscopy pill; 4 hours later, those patients ate a snack and 8 hours later, the data were downloaded. The gastric emptying rate was measured using RAPID 4 Software. No significant variations in gastric emptying rates were seen among CD patients. Pearson’s correlation test showed a significant correlation between the gastric emptying rate in CD (r=0.1706). Similarly, Usai-Satta et al. (2016) [16] also used a C-octanoic acid breath test to study the gastric transit time in 12 newly diagnosed adult patients with CD and 30 healthy controls with reflux symptoms. A unvalidated symptom assessment tool was used to measure dyspepsia symptoms, and a duodenal biopsy was obtained from all subjects. They ate a balanced trial meal after midnight fasting, and breath tests were taken two times before and every 15 minutes post-prandial for four hours. The gastric transit time of newly diagnosed adults with CD was significantly longer than controls (t1⁄2: 2056134 versus 91621 min, p=0.01). After following a gluten-free diet for 12 months, a second C-octanoic acid breath test was conducted in CD patients, and they ate the same trial meal but with a gluten-free ingredient. No significant improvement in the gastric transit time was found, but dyspepsia symptoms improved significantly (p=0.0002). In line with this, in 2016, Przybylska-Feluś et al. [17] used Electrogastrography (EGG) to measure gastric motility in 25 newly diagnosed adult patients with CD and 30 controls without GI complaints. A duodenal biopsy was obtained from patients with CD, and a blood sample was collected from all study subjects. After midnight fasting (12 hs), 30 minutes registration of gastric myoelectric activity using EGG at baseline and 1 hour after drinking oral nutritional supplements (Nutridrink, 300 kcal/300 ml, Nutricia). They found among patients with CD at baseline (fasting) a lower percentage of normogastria (54.8±24.5 vs. 86±12.3%, p=0.02) and steady wave coupling (52.7±13.4 vs. 77.4±11.9%; p=0.00001) with enlarged dominant power (11.6±1.5 vs. 11.1±1.1). In opposition to the controls, they did not manifest an improvement in the percentage of normogastria, slow wave coupling, and dominant power when examined post-prandial (p<0.05), (Table 1).
Pathophysiological mechanisms of gastric motility disorders in patients with CD
As demonstrated earlier, gastric motility disorders are more frequently present among patients with CD. Several hypotheses may help explain these phenomena. Gastric activity results from systematic interactions between the different tissues in the gastrointestinal tract, enteric nervous system, interstitial cells of Cajal involuntary muscle, and gut-associated lymphoid tissue. The gastrointestinal tract produces voluntary contractile and electrical enterprise regulated by signals from the immune system, the cerebrospinal nervous system, and the hormone system [23]. These are two-way enterprises. A low-grade tissue inflammation (early cytokine release) and mastocyte infiltration may alter gastric motility [24]. Dysfunction of the vegetative nervous system is hypothesized to be another cause of delayed gastric motility [25]. In addition, gluten malabsorption is thought to be an important factor affecting the neuromuscular function of the gastrointestinal tract. Another possible cause is gut microbiome imbalance [26]. Different psychological morbidity is a common complaint among patients with CD [27], a well-known crosstalk between gastric motility dysfunction and psychological dysfunction [28]. Other mechanisms involve autoimmunity that activates antineuronal antibodies in patients with celiac disease and evokes neurodegeneration via neuronal cell apoptosis in the central or peripheral nervous system [29,30]. As well as anti-actin IgA antibodies may contribute in the development of gastric dysmotility through structural and functional alterations in the gastric smooth muscle cells and enteric nervous system [31]. Finally, numerous studies investigate the changes in various hormone secretion in CD patients and how those changes may alter gastric motility (Figure 2).
Hormones and gastric motility disorders among CD patients in different studies
In 2000, Bardella et al. [11] studied the neurotens in hormone, which inhabits gastric activity. Nine newly diagnosed patients with CD had positive duodenal biopsy, and nine controls had negative CD serology tests. The participants ate a high-fat trial meal after midnight fasting; serum blood test was collected in fasting status immediately after the meal, then at 30, 60, 75, 90 minutes, and 2 hours post-prandial. The researchers found significantly higher fasting neurotensin levels in CD patients than in healthy controls (41.6±23.9 versus 18.2±5.5 pg/ml, P=0.0214). Additionally, Nicholas et al. [18] studied the novel role of serotonin (5-hydroxytryptamine) on gastric motility among patients with CD, including 18 adults with positive IgA anti-endomysia antibodies and duodenal biopsy; 10 patients group complain of irritable bowel syndrome or dyspepsia and8 control patients group complain of anemia without gastrointestinal complain. The third group included 18 healthy control participants. The fourth control group included 12 patients who went for a duodenal biopsy investigation due to asymptomatic hemolytic anemia. A blood sample was obtained after midnight fast to measure platelet and plasma 5-hydroxytryptamine concentrations. Participants ate a high carbohydrate trial meal for 15 minutes; then, blood samples were collected directly and frequently seven times over 3 hours at 30-minute intervals. The intensity of the gastrointestinal symptoms was measured using a validated questionnaire 30 minutes premeal and frequently six times post-meal at 30-minute intervals. At the end of the trial, a duodenal biopsy was performed to measure the intestine content of 5-hydroxyindoleacetic acid and 5-hydroxytryptamine. This study shows a higher plasma serotonin level among patients with CD compared to control (P 0.0006) and higher duodenal serotonin levels (P 0.007). A significant association between maximum serotonin level and the severity of dyspepsia symptoms (P 0.005) was also reported. In 2003, Peracchi et al. [19] studied ghrelin hormone by including 30 newly diagnosed CD patients, 13 treated CD patients with gluten-free diets for at least two years with negative duodenal biopsy results, and 30 healthy controls. After midnight, fasting serum level of ghrelin was measured. They found significantly higher ghrelin levels among the newly diagnosed patients with CD in comparison to the other two groups: patients with CD on a gluten-free diet (p<0.05) and the healthy controls (p<0.01). Another interesting finding was that serum ghrelin level was significantly correlated with the degree of intestinal mucosal damage (rs=0.444, p<0.02). In 2005, Capristo et al. [20] studied ghrelin hormone levels in 18 adult women diagnosed with CD and 22 healthy controls, and a blood sample was collected retrospectively. They found an insignificant difference between the two groups in non-fasting serum ghrelin levels. However, limitations related to the methodology were identified, suggesting that the results should be cautiously taken. On the other hand, in 2006, Lanzini et al. [21] also studied the ghrelin hormone in patients with dyspepsia and patients with CD. A positive histology sample confirmed the CD diagnosis in 44 adults. Thirty-nine patients were diagnosed with dyspepsia by using validated diagnostic criteria; all of them had negative histology samples and 53 healthy controls. Serum blood ghrelin levels were taken from all participants. A significantly higher level of ghrelin in patients with CD (531±29 pg/mL, P<0.05) was recorded and similar results among patients with dyspepsia (526±14 pg/mL, P<0.01) in comparison to the healthy control group (451±8 pg/mL) were seen. Contrary to the previous study, no association was seen between ghrelin hormone level and the severity of intestinal mucosal damage. The measurement of non-fasting serum ghrelin levels, could affect the accuracy of the result. In 2008, Rocco et al. [14] as mentioned earlier in this review also studied the ghrelin hormone. Twenty adults were newly diagnosed with CD and 10 controls with reflux symptoms; a validated dyspepsia questionnaire was administered; a duodenal biopsy was done to confirm CD diagnosis and a gastric biopsy to measure ghrelin level was obtained from all study subjects. They found signifi cantly higher tissue ghrelin levels (P<0.0001) among patients with CD compared to healthy control subjects. However, no association was found between tissue ghrelin and gastric activity levels. Przybylska-Feluś et al. (2016) [17] also studied ghrelin and pancreatic polypeptide plasma, the latest found to impair gastric motility in 25 newly diagnosed adult patients with CD and 30 controls without GI complaints. A duodenal biopsy was obtained from patients with CD. After midnight fasting (12 hs), blood samples were collected from all study subjects to measure ghrelin and pancreatic polypeptide plasma levels. They found patients with CD have a lower level of ghrelin after 12 hours of food abstinence in comparison to healthy controls, 156.8±86.7 vs 260.2±87.6 pg/ml (p=0.0002). And higher pancreatic polypeptide plasma in comparison to healthy controls 265.2±306.3 vs. 54.1±54.6 pg/ml (p=0.0005). A more recent study byVitaglione et al. [22] in 2019 studied ghrelin hormone levels in 9 newly diagnosed women with CD, 13 women with CD treated with a gluten-free diet for at least one year, and 10 healthy controls. After overnight fasting, a blood sample was collected, and then the participants ate a gluten-free trial meal for 15 minutes; after that, the blood sample was collected directly and then four times at 30-minute intervals. They found a significantly lower level of ghrelin hormone among patients with CD compared to the healthy control subjects (p<0.05). However, a limitation of this study is that gherlin hormone levels were studied in only women, (Table 2).
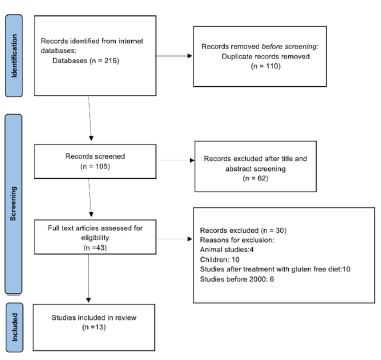
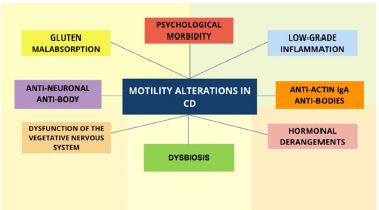
Table 1: Summary of the studies on gut motility in celiac disease using different technics.
| First authors,year | Title | Subjects | Study type | Technic | Findings |
|---|---|---|---|---|---|
| Bardella 2000 | Gastric Emptying and Plasma Neurotensin Levels in Untreated Celiac Patients | 9 NewCD adult9 Healthycontrols | Case- control | Ultrasound | Delay gastricemptying |
| Marciani 2005 | Gallbladder Contraction, Gastric Emptying and Antral Motility: SingleVisit Assessment of Upper GI Function in Untreated CeliacDisease Using Echo-Planar MRI | 15 New CD adult 15 Healthycontrols | Case- control | Echo-Planar MRI | No delay ingastric emptying |
| Bassotti 2008 | Antroduodenojejunal motor activity in untreated andtreated celiac diseasepatients | 11 NewCD adult12 CD Treated33 Healthycontrols | Case- control | Antro-duodenal manometry | No delay ingastric emptying |
| Rocco 2008 | Tissue ghrelinlevel and gastricemptying rate in adult patientswith celiacdisease | 20 New CD adult 10 Controls withreflux symptoms | Case- control | C-octanoic acid breath test | Delay gastricemptying |
| Urgesi 2013 | Evaluation of gastric and small bowel transit times in coeliac disease with the small bowel PillCam: asingle center study in a non-gluten-free dietadult Italian population with coeliac disease | 30 New CD adult 30 HealthyControls | Case- control | PillCam | No delay ingastric emptying |
| Usai-Satta2016 | Delayed gastricemptying does not normalize afterglutenwithdrawal in adult celiacdisease. | 12 New CD adult 30 HealthyControls | Case- control | C-octanoic acid breath test | Delay gastricemptying |
| Przybylska- Feluś 2016 | Ghrelin, pancreatic polypeptide plasma concentrations andgastric myoelectric activityin celiac disease | 25 New CD adult 30 HealthyControls | Case- control | Electrogastrography | Delay gastricemptying |
CD: Celiac disease; GI: Gastrointestinal; MRI: Magnetic resonance imaging.
Table 2: Summary of the studies on gastric motility disordersin celiac disease and different hormones.
| First authors,year | Title | Subjects | Study type | Hormone | Finding |
|---|---|---|---|---|---|
| Bardella 2000 | Gastric Emptying and Plasma NeurotensinLevels in Untreated CeliacPatients | 9 NewCD adult9 Healthycontrols | Case-control | Neurotensin | High fastingneurotensin level |
| Nicholas 2006 | Abnormalities of Serotonin Metabolism and TheirRelation to Symptoms in Untreated CeliacDisease | 18 NewCD adults,10 with IBS or dyspepsia15 Healthy controls with anemia 18 Healthy controls12 patients with a duodenal biopsy for asymptomatic hemolytic anemia | Case-control | Serotonin | High fastingserotonin level |
| Peracchi 2003 | Circulating Ghrelin Levelsin Celiac Patients | 30 New CD adult 13 CD Treated30 Healthy controls | Case-control | Ghrelin | High fasting ghrelinlevel |
| Capristo 2005 | Reduced plasma ghrelin concentration in celiacdisease after gluten-free diet treatment | 18 NewCD adult22 Healthy controls women | Case-controlretrospective | Ghrelin | No difference in non-fasting ghrelin level |
| Lanzini2006 | Circulating ghrelin level is increased in coeliac diseaseas in functional dyspepsia and reverts to normal duringgluten-free diet | 44 NewCD adult39 non-CD withdyspepsia 53 HealthyControls | Case-control | Ghrelin | High non-fasting ghrelinlevel |
| Rocco 2008 | Ghrelin, pancreatic polypeptide plasma concentrations and gastric myoelectric activity in celiac disease | 20 NewCD adult10 HealthyControls with refluxSymptoms | Case-control | Ghrelin | High numberoftissue ghrelinlevel |
| Przybylska- Feluś2016 | Ghrelin, pancreatic polypeptide plasma concentrations and gastric myoelectric activity in celiacdisease | 25 New CD adult 30 HealthyControls | Case-control | Ghrelin &pancreatic polypeptide plasma | A lower levelof ghrelin. High level of pancreatic polypeptide |
| Vitaglione 2019 | Appetite and Gastrointestinal Hormone Response to a Gluten-Free Mealin Patients with Coeliac Disease | 9 New CD women 13 CD Treated10 Healthy Controls | Case-control | Ghrelin | Nodifference in post-prandial ghrelin level |
CD: Celiac disease
Conclusion
In conclusion, following a strict gluten-free diet can be potent in normalizing and improving gastric mobility among patients newly diagnosed with CD [10]. The previously mentioned studies showed that neurotensin, serotonin, pancreatic polypeptide plasm hormones disturbance could explain the delayed gastric motility in patients with untreated celiac disease. Further high-quality studies using standardized, nutritionally balanced test meals are needed to support the conflicting results of ghrelin levels and its effect on gastric dysmotility. Moreover, conducting studies with the inclusion of other hormones that affect gastric motility, like gastrin and irisin are crucial.
Nonetheless, significant gastric motility delay was found in patients with celiac disease, using different techniques: ultrasound, C-octanoic acid breath test, and electrogastrography. In contrast insignificant delay in gastric motility was found using Echo-Planar MRI, Antro-duodenal manometry, PillCam techniques. Further studies are needed to assess gastric motility using standardized, nutritionally balanced test meals. Moreover, we encourage the health care providers to perform medical diagnosis of delayed gastric emptying using more convenient and less invasive techniques. Eventually, we recommend medical screening for CD among patients with compliant of delayed gastric emptying to increase the detection of CD.
References
- Stroud C, Almilaji O, Nicholas D, Kirkham S, Surgenor SL, Williams I, et al. Evolving patterns in the presentation of coeliac disease over the last 25 years. Frontline Gastroenterol. 2019; 11: 98-103.
- Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, et al. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018; 16: 823-836.e2.
- Ludvigsson JF, Leffler DA, Bai JC, Biagi F, Fasano A, Green PH, et al. The Oslo definitions for coeliac disease and related terms. Gut. 2013; 62: 43-52.
- Petersen J, Ciacchi L, Tran MT, Loh KL, Kooy-Winkelaar Y, Croft NP, et al. T cell receptor cross-reactivity between gliadin and bacterial peptides in celiac disease. Nat Struct Mol Biol. 2020; 27: 49-61.
- Bouziat R, Hinterleitner R, Brown JJ, Stencel-Baerenwald JE, Ikizler M, Mayassi T, et al. Reovirus infection triggers inflammatory responses to dietary antigens and development of celiac disease. Science. 2017; 356: 44-50.
- Ramakrishna BS, Makharia GK, Chetri K, Dutta S, Mathur P, Ahuja V, et al. Prevalence of Adult Celiac Disease in India: Regional Variations and Associations. Am J Gastroenterol. 2016; 111: 115-23.
- Sallese M, Lopetuso LR, Efthymakis K, Neri M. Beyond the HLA Genes in Gluten-Related Disorders. Front Nutr. 2020; 7: 575844.
- Singh AD, Ellias S, Singh P, Ahuja V, Makharia GK. The Prevalence of the Celiac Disease in Patients with Dyspepsia: A Systematic Review and Meta-Analysis. Dig Dis Sci. 2022; 67: 3067-3079.
- Wauters L, Dickman R, Drug V, Mulak A, Serra J, Enck P, et al. United European Gastroenterology (UEG) and European Society for Neurogastroenterology and Motility (ESNM) consensus on functional dyspepsia. United European Gastroenterol J. 2021; 9: 307-331.
- Usai-Satta P, Oppia F, Lai M, Cabras F. Motility Disorders in Celiac Disease and Non-Celiac Gluten Sensitivity: The Impact of a Gluten-Free Diet. Nutrients. 2018; 10: 1705.
- Bardella MT, Fraquelli M, Peracchi M, Cesana BM, Bianchi PA, Conte D. Gastric emptying and plasma neurotensin levels in untreated celiac patients. Scand J Gastroenterol. 2000; 35: 269-273.
- Marciani L, Coleman NS, Dunlop SP, Singh G, Marsden CA, Holmes GK, et al. Gallbladder contraction, gastric emptying and antral motility: single visit assessment of upper GI function in untreated celiac disease using echo-planar MRI. J Magn Reson Imaging. 2005; 22: 634-8.
- Bassotti G, Villanacci V, Mazzocchi A, Mariano M, Incardona P, Clerici C, et al. Antroduodenojejunal motor activity in untreated and treated celiac disease patients. J Gastroenterol Hepatol. 2008; 23: e23-8.
- Rocco A, Sarnelli G, Compare D, de Colibus P, Micheli P, Somma P, Marotti B, et al. Tissue ghrelin level and gastric emptying rate in adult patients with celiac disease. Neurogastroenterol Motil. 2008; 20: 884-90.
- Urgesi R, Cianci R, Bizzotto A, Costamagna G, Riccioni ME. Evaluation of gastric and small bowel transit times in coeliac disease with the small bowel PillCam®: a single centre study in a non-gluten-free diet adult Italian population with coeliac disease. Eur Rev Med Pharmacol Sci. 2013; 17: 1167-73.
- Usai-Satta P, Oppia F, Scarpa M, Giannetti C, Cabras F. Delayed gastric emptying does not normalize after gluten withdrawal in adult celiac disease. Scand J Gastroenterol. 2016; 51: 923-6.
- Przybylska-Feluś M, Furgała A, Kaszuba-Zwoińska J, Thor P, Mach T, Zwolińska-Wcisło M. Ghrelin, pancreatic polypeptide plasma concentrations and gastric myoelectric activity in celiac disease. Folia Med Cracov. 2016; 56: 56-72.
- Coleman NS, Foley S, Dunlop SP, Wheatcroft J, Blackshaw E, Perkins AC, et al. Abnormalities of serotonin metabolism and their relation to symptoms in untreated celiac disease. Clin Gastroenterol Hepatol. 2006; 4: 874-81.
- Peracchi M, Conte D, Terrani C, Pizzinelli S, Gebbia C, Cappiello V, et al. Circulating ghrelin levels in celiac patients. Am J Gastroenterol. 2003; 98: 2474-8.
- Capristo E, Farnetti S, Mingrone G, Certo M, Greco AV, Addolorato G, et al. Reduced plasma ghrelin concentration in celiac disease after gluten-free diet treatment. Scand J Gastroenterol. 2005; 40: 430-6.
- Lanzini A, Magni P, Petroni ML, Motta M, Lanzarotto F, Villanacci V, et al. Circulating ghrelin level is increased in coeliac disease as in functional dyspepsia and reverts to normal during gluten-free diet. Aliment Pharmacol Ther. 2006; 23: 907-13.
- Vitaglione P, Zingone F, Virgilio N, Ciacci C. Appetite and Gastrointestinal Hormone Response to a Gluten-Free Meal in Patients with Coeliac Disease. Nutrients. 2019; 11: 82.
- Pinto-Sanchez MI, Bercik P, Verdu EF. Motility alterations in celiac disease and non-celiac gluten sensitivity. Dig Dis. 2015; 33: 200-207.
- Ohman L, Simrén M. Pathogenesis of IBS: role of inflammation, immunity and neuroimmune interactions. Nat Rev Gastroenterol Hepatol. 2010; 7: 163-73.
- Giorgetti GM, Tursi A, Iani C, Arciprete F, Brandimarte G, Capria A, et al. Assessment of autonomic function in untreated adult coeliac disease. World J Gastroenterol. 2004; 10: 2715-8.
- Chang MS, Green PH. A review of rifaximin and bacterial overgrowth in poorly responsive celiac disease. Therap Adv Gastroenterol. 2012; 5: 31-6.
- Zingone F, Swift GL, Card TR, Sanders DS, Ludvigsson JF, Bai JC. Psychological morbidity of celiac disease: A review of the literature. United European Gastroenterol J. 2015; 3: 136-45.
- Sanchez JMS, McNally JS, Cortez MM, Hemp J, Pace LA, Clardy SL. Neuroimmunogastroenterology: At the Interface of Neuroimmunology and Gastroenterology. Front Neurol. 2020; 11: 787.
- Cervio E, Volta U, Verri M, Boschi F, Pastoris O, Granito A, et al. Sera of patients with celiac disease and neurologic disorders evoke a mitochondrial-dependent apoptosis in vitro. Gastroenterology. 2007; 133: 195-206.
- Volta U, De Giorgio R, Petrolini N, Stangbellini V, Barbara G, Granito A, et al. Clinical findings and anti-neuronal antibodies in coeliac disease with neurological disorders. Scand J Gastroenterol. 2002; 37: 1276-81.
- Granito A, Muratori P, Cassani F, Pappas G, Muratori L, Agostinelli D, et al. Anti-actin IgA antibodies in severe coeliac disease. Clin Exp Immunol. 2004; 137: 386-92.