
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 5
Secondary fundic gland polyp induced by proton pump inhibitor therapy
Samavati Shayan, BS1*; Lippmann Alec, JBS1; Awan Muhammad, HBS1; Dinparastisaleh Roshan, MD2
1Alabama College of Osteopathic Medicine, USA.
2Department of Internal Medicine, North Alabama Medical Center, USA.
*Corresponding Author : Samavati Shayan
Alabama College of Osteopathic Medicine, 445 Health Sciences Blvd. Dothan, AL, 36303, USA.
Tel: +1 (334) 699-2266;
Email: samavatis@acom.edu
Received : Jan 06, 2025
Accepted : Feb 14, 2025
Published : Feb 21, 2025
Archived : www.jjgastro.com
Copyright : © Samavati S (2025).
Abstract
Proton Pump Inhibitors (PPI) are widely prescribed for managing acid-related gastrointestinal disorders, such as Gastroesophageal Reflux Disease (GERD). While effective, long-term PPI use has been associated with the development of Fundic Gland Polyps (FGPs), benign gastric lesions with significant clinical implications. This case report explores the association between prolonged PPI therapy and the development of FGPs through the clinical course and management of a 57-year-old patient with a 17-year history of GERD and pantoprazole use, who presented with persistent postprandial discomfort. Upper gastrointestinal endoscopy revealed multiple fundic gland polyps in the gastric body and cardia, along with cobblestone-like mucosal changes. Polypectomy and histopathological examination confirmed hyperplastic FGPs without evidence of dysplasia, atrophy, or Helicobacter pylori infection. Proton pump inhibitor therapy was thereupon discontinued, resulting in partial regression of mucosal changes but continued growth in unresected polyps. Subsequent endoscopic interventions demonstrated ongoing FGP progression despite PPI cessation, warranting a discussion regarding the complex relationship between fundic gland polyps and PPIs and the long-term effects of proton pump inhibitors on gastric mucosa. Periodic endoscopic evaluation and careful consideration of the risks and benefits of long-term proton pump inhibitor use are essential for optimizing patient outcomes. Further research is needed to clarify the mechanisms and management of PPI-associated FGPs.
Keywords: Proton pump inhibitors; Gastroesophageal reflux disease; Fundic gland polyps; Gastric polyps; Hypergastrinemia; Long-term therapy; Endoscopy.
Abbreviations: EMR: Endoscopic Mucosal Resection; EGD: Eesophagogastroduodenoscopy; FAP: Familial Adenomatous Polyposis; FGP: Fundic Gland Polyp; GERD: Gastroesophageal Reflux Disease; GI: Gastrointestinal; H. pylori: Helicobacter pylori; PPI: Proton Pump Inhibitor.
Citation: Samavati S, Lippmann AJ, Awan MH, Dinparastisaleh R. Secondary fundic gland polyp induced by proton pump inhibitor therapy. J Gastroenterol Res Pract. 2025; 5(1): 1224.
Introduction
The widespread use of Proton Pump Inhibitors (PPIs) in managing stomach acid-related disorders, particularly Gastroesophageal Reflux Disease (GERD), has significantly increased over recent decades due to their superior efficacy compared to histamine receptor antagonists [1,2]. Despite the clear benefits of PPIs in controlling acid secretion and providing relief for conditions like GERD, long-term PPI therapy has raised concerns due to potential adverse effects, most notably the development of Fundic Gland Polyps (FGPs) [3]. FGPs are benign lesions that occur in the stomach’s lining, and while they are often asymptomatic, their development has been strongly linked to long-term PPI therapy. Most studies suggest that FGPs may resolve after discontinuing PPI treatment, yet their prevalence remains significant, accounting for 16.3% of gastric polyps, according to a five-year study [4-6]. These polyps tend to occur more frequently in women and in individuals over 60 years old. They are typically found in non-atrophic gastric mucosa without evidence of Helicobacter pylori infection or active gastritis [7,8]. For instance, among 186 patients with FGPs, the majority were women aged 51 to 70, and 78% had been using PPIs for over five years [9]. In this case report, we present a patient who developed fundic gland polyps after 17 years of PPI use. Through this case, we explore the clinical implications of prolonged PPI therapy and contribute to the ongoing discussion about the safety of long-term use.
Case presentation
A 57-year-old man was referred to our center with a 17-year history of reflux symptoms and a previous diagnosis of mild gastritis based on an endoscopy performed 16 years earlier. Over the course of 17 years, the patient had been taking Proton Pump Inhibitor (PPI) therapy (pantoprazole 40 mg daily) due to recurrent worsening of reflux symptoms upon attempts to discontinue the medication. His medical history also included hypertriglyceridemia, which was managed with fenofibrate.
At initial presentation, the patient reported persistent postprandial abdominal discomfort and fullness despite ongoing PPI treatment. A follow-up upper Gastrointestinal (GI) endoscopy performed in 2022 revealed multiple gastric polyps of varying sizes located in the body and cardia of the stomach (Figure 1 & Table 1). Additionally, the gastric mucosa exhibited a cobblestone-like appearance and multiple white, flat elevated lesions. The esophagus and duodenum appeared normal.
To address the gastric polyps, a complete cold polypectomy was performed, targeting polyps larger than 7 mm. Histopathological evaluation revealed no evidence of Helicobacter pylori infection, mucosal atrophy, intestinal metaplasia, or dysplasia (Table 2). The findings were consistent with hyperplastic fundic gland polyposis. Subsequent lower gastrointestinal tract evaluation revealed a 5 mm sessile polyp in the transverse colon with mild chronic inflammation limited to the mucosal layer but no other abnormalities.
Following shared decision-making with the patient, a trial of discontinuing PPI therapy was initiated for approximately one year. A repeat upper GI endoscopy in 2023 revealed the partial resolution of the cobblestone-like appearance of the gastric mucosa. However, while the previously resected polyps did not recur, the unresected polyps (smaller than 7 mm in 2022) demonstrated growth, with the largest measuring over 10 mm. Once again, multiple polyps were resected via polypectomy and Endoscopic Mucosal Resection (EMR) (Table 1, Figures 2 & 3), as EMR was required for complete removal of the larger and more complex polyps. Histopathological examination confirmed findings consistent with hyperplastic fundic gland polyposis, with no evidence of Helicobacter pylori, mucosal atrophy, intestinal metaplasia, or dysplasia (Table 2).
This case highlights our consideration of the potential association between long-term PPI use and the development of Fundic Gland Polyps (FGPs), despite the polyps showing no signs of atrophy, dysplasia, or metaplasia. Although we cannot confirm that the FGPs in this patient are PPI-induced, we decided to discontinue PPI therapy to minimize any potential risk. We emphasized to the patient the importance of regular GI follow-up, including periodic upper GI endoscopies, to monitor any progression or recurrence of the polyps. This case underscores the need for careful, individualized management and ongoing evaluation of the risks and benefits of long-term PPI use.
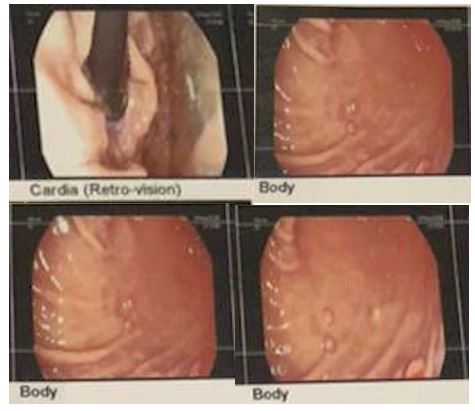
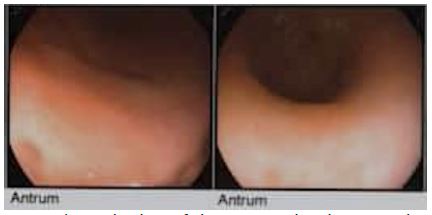

Table 1: Esophagogastroduodenoscopy (EGD) and Colonoscopy comparison for the patient from 2022 vs 2023 showing a decrease in number of polyps in the stomach.
| Parameter | 2022 Findings | 2023 Findings |
|---|---|---|
| Esophagus | Normal crico-pharyngeus, upperthird, middle third,lower third, and loweresophageal sphincter. | Normal crico-pharyngeus, upperthird, middle third,lower third, and lower esophageal sphincter. |
| Stomach | Multiple polyps of varying sizes seen in the bodyand cardia.Cobblestone-like gastricmucosal changes. | Large (>10 mm) and medium(5-10 mm) polypsseen in cardia, fundus, and body. |
| Antrum | Normal. | Normal. |
| Duodenum | Normal bulband second part. | Normal bulband second part. |
| Colon findings | Internal hemorrhoids observed. 5 mm sessilepolyp in transverse colon. Othersegments normal. | Single erosion in rectum, internal hemorrhoids observed. Othersegments normal. |
| Therapeutic operations | Biopsy of antrumand body performed. Polyps > 7 mm resected using a cold snare. Complete polypectomy ofcolon polyp. | Multiple polypsresected using polypectomy EMR. |
| Final diagnosis | Normal esophagus and duodenum. Grade 1 hemorrhoids. Polyp(stomach and transverse colon). | Normal esophagus. Polyp (stomach). |
Table 2: Pathological comparison for the patient from 2022 vs 2023 showing a decrease in number of polyps in the stomach.
| Category | 2022 Findings | 2023 Findings |
|---|---|---|
| Specimen | A) Gastric mucosa biopsy, Antrum B) Gastric mucosa biopsy, Body C) Gastric polyp resection, Body D) Colonic polyp resection, Descending |
A) Gastric mapping biopsy B) Body gastric mucosa biopsy C) Rectal mucosa biopsy |
| Clinical data | Stomach: Multiple polyps of varying sizes in the body and cardia; antrum
normal. Colon: Internal hemorrhoids in rectum; 5 mm sessile polyp in transverse colon. |
Stomach: Large (>10 mm) and medium (5-10 mm) polyps in cardia, fundus, and body; antrum normal. Colon: Anus normal; single erosion and internal hemorrhoids in rectum; other regions normal. |
| Macroscopic | A) Two pieces, 0.3x0.2x0.2 cm B) Two pieces, 0.3x0.2x0.2 cm C) Four pieces, 1.0x0.5x0.5 cm D) One piece, 0.2x0.2x0.1 cm |
A) Three pieces, 0.3x0.3x0.2 cm B) Multiple pieces, 0.5x0.3x0.2 cm C) One piece, 0.2x0.1x0.1 cm |
| Microscopic | A to D) Histological findings support the following diagnoses. | A,B,C) Histological findings support the following diagnoses. |
| Diagnosis (Stomach) | Gastric mucosa biopsy (Antrum): − Compatible with PPI effect − No H. pylori, metaplasia, dysplasia, or atrophy Gastric mucosa biopsy (Body): − Compatible with PPI effect − No H. pylori, metaplasia, dysplasia, or atrophy Gastric polyp resection (Body): − Fundic gland polyp − No H. pylori, metaplasia, dysplasia, or atrophy |
Gastric mapping biopsy: − Reactive gastropathy − No metaplasia, dysplasia, atrophy, or H. pylori Body gastric mucosa biopsy: − Fundic gland polyp − No metaplasia, dysplasia, or H. pylori |
| Diagnosis (Colon) | Colonic polyp resection (Descending): − Mucosal polyp with architecturally preserved mild chronic inflammation |
Rectal mucosa biopsy: − Unremarkable rectal mucosa |
Discussion
In the present case report, fundic gland polyps were identified in a patient with a history of long-term proton pump inhibitor use for the management of gastric reflux symptoms. PPIs are widely recognized for their efficacy in treating acid-related gastrointestinal disorders. However, an increasing body of evidence suggests an association between prolonged PPI use and the development of FGPs [3,10].
Jalving et al. observed that PPI use for more than one year was associated with a fourfold increase in the risk of developing FGPs [11]. This finding aligns with broader literature documenting hypergastrinemia, mucus obstruction of fundic pits, and hypertrophy and hyperplasia of gastric enterochromaffin-like and parietal cells among patients undergoing long-term PPI therapy [12,13]. These physiological changes are believed to contribute to the pathogenesis of FGPs.
The compensatory hypergastrinemia observed in long-term PPI users results from the suppression of gastric acid secretion. This inhibition triggers increased gastrin production, which in turn stimulates gastric cellular proliferation, potentially promoting the development of FGPs [13]. Additionally, the reduction in gastric acid secretion caused by PPIs may lead to decreased gastric secretion flow. This stasis can result in mucus accumulation and blockage of the fundic pits, facilitating the formation of fundic gland cysts, which are considered precursors to FGPs [13]. Epidemiological data further support these findings, demonstrating that long-term PPI use (≥5 years) is associated with a fourfold increased risk of developing FGPs, with an odds ratio of 3.8 (95% CI: 2.2–6.7) [14].
Although a few reports explore the potential protective effect of Helicobacter pylori (H. pylori) against the development of FGPs, it is notable that H. pylori was not detected in the present case. H. pylori infection is known to degrade gastric mucus through enzymatic activity, particularly via protease-mediated mechanisms. This degradation facilitates glandular outflow and prevents cystic dilation, potentially mitigating the risk of FGP formation. However, long-term PPI use has been associated with lower rates of H. pylori colonization, which may reduce this protective effect and increase susceptibility to glandular blockage and FGP development. Supporting evidence highlights a significantly lower prevalence of H. pylori infection among patients with FGPs (18.7%) compared to those with other types of gastric polyps (44.2%) [9,13].
Fundic gland polyps are among the most common types of gastric polyps encountered in clinical practice, and understanding their etiology and characteristics is essential for effective management. These polyps can be broadly categorized into sporadic and syndromic types, with distinct clinical and pathological profiles that guide diagnosis and treatment [15].
Our patient’s presentation aligns with the features of sporadic FGPs, which are closely associated with prolonged Proton Pump Inhibitor (PPI) use [15]. Sporadic FGPs are typically benign and rarely exhibit dysplasia. Nonetheless, low-grade epithelial dysplasia has been observed in about 1% of cases, which helps to differentiate them from syndromic FGPs which are often linked to Familial Adenomatous Polyposis (FAP) [16]. In syndromic cases, the presence of dysplasia significantly heightens the risk of malignant transformation [15]. A study by M.D. Levy et al. reported that follow-up EGD in 42% of cases supported the consensus that polyps originating from sporadic FGPs rarely progress to malignancy. The absence of p53 overexpression in sporadic FGPs likely explains their minimal risk of advancing to high-grade dysplasia or adenocarcinoma, further emphasizing their typically benign nature [16].
At the initial evaluation, our 57-year-old patient presented with multiple gastric polyps of varying sizes located in the cardia and body, with no involvement of the antrum. Histopathological analysis revealed no evidence of dysplasia, metaplasia, atrophy, or H. pylori infection, findings consistent with sporadic fundic gland polyps. Additionally, the lack of a family history of FAP, the absence of dysplasia, antral involvement, or duodenal adenomas further ruled out syndromic etiology.
Although sporadic FGPs are benign and generally carry no risk of malignancy [16,19], the decision to discontinue PPI therapy, in this case, was aimed at preventing the formation of new polyps, limiting the growth of unresected polyps, and evaluating the potential reversibility of existing polyps. This approach aligns with emerging evidence suggesting that stopping PPI therapy can lead to partial regression of FGPs. For instance, Kazantsev et al. reported significant regression of FGPs in a patient following the cessation of PPI therapy combined with anti-reflux surgery [5]. Similarly, Choudhry et al. observed polyp regression within three months of stopping PPIs, although recurrence was noted upon resumption of the medication [4]. Additionally, Kim et al. documented substantial regression of FGPs within a year of discontinuing PPI therapy, indicating that regression may be achievable in certain cases [17]. In our patient’s case, discontinuing PPI therapy for approximately a year led to partial resolution of the cobblestone appearance of the gastric mucosa, demonstrating reversibility of certain PPI-associated alterations upon cessation of therapy.
However, polyp growth persisted in unresected areas in our patient despite PPI cessation. This contrasts with findings in a case study by Brockmeyer et al., where polyps in unresected areas regressed 9 months after discontinuation of PPI therapy in their patient [17]. The continued polyp growth in our patient thus prompts us to consider the argument that PPIs may not be as significant a risk factor for FGP development as proposed. For example, in a retrospective study by Vieth et al., the frequency of FGPs in patients without H. pylori receiving PPI therapy was compared with a control group of patients without H. pylori who did not receive PPI therapy. The researchers found that both groups exhibited an identical frequency of FGPs, inferring an unlikely causal relationship between PPI therapy and progression of FGPs [18]. These differing findings in literature highlight the need for further investigation of the complex relationship between proton pump inhibitors and the progression or regression of fundic gland polyps.
While it cannot be definitively concluded that the observed gastric mucosal abnormalities were directly caused by chronic PPI use or that their resolution was solely due to discontinuing the therapy, this case could provide anecdotal support for a potential link. For patients on long-term PPI therapy who develop sporadic FGPs, periodic endoscopic evaluation may be warranted to monitor the development or progression of these polyps. Polyp size, number, and histopathological characteristics should guide clinical decision-making, particularly when considering polypectomy or ongoing surveillance [5,15].
In conclusion, this case highlights the complex relationship between long-term PPI therapy and the development of sporadic FGPs. The partial regression of the cobblestone-like gastric mucosal changes following PPI discontinuation suggests that some mucosal alterations may be reversible, though not entirely preventable. While sporadic FGPs are typically benign and pose minimal risk of malignancy, the persistence of polyp growth in unresected areas underscores the importance of individualized management strategies.
Conclusion
This case highlights the association between long-term PPI therapy and the development of Fundic Gland Polyps (FGPs), emphasizing the need for regular monitoring in such patients. While discontinuation of PPI therapy may lead to regression of FGPs, the extent of regression varies, and further research is needed to understand long-term outcomes. This case underscores the importance of individualized PPI therapy to balance its benefits against potential risks.
References
- Hess MW, Hoenderop JG, Bindels RJ, Drenth JP. Systematic review: hypomagnesaemia induced by proton pump inhibition. Aliment Pharmacol Ther. 2012; 36: 405-413.
- Gill JM, Player MS, Metz DC. Balancing the risks and benefits of proton pump inhibitors. Ann Fam Med. 2011; 9: 200-202.
- Hongo M, Fujimoto K; Gastric Polyps Study Group. Incidence and risk factor of fundic gland polyp and hyperplastic polyp in long-term proton pump inhibitor therapy: a prospective study in Japan. J Gastroenterol. 2010; 45: 618-624.
- Choudhry U, Boyce HW Jr, Coppola D. Proton pump inhibitor-associated gastric polyps: a retrospective analysis of their frequency, and endoscopic, histologic, and ultrastructural characteristics. Am J Clin Pathol. 1998; 110: 615-621.
- Kazantsev GB, Schwesinger WH, Heim-Hall J. Spontaneous resolution of multiple fundic gland polyps after cessation of treatment with lansoprazole and Nissen fundoplication: a case report. Gastrointest Endosc. 2002; 55: 600-602.
- Morais DJ, Yamanaka A, Zeitune JMR, Andoreollo NA. Gastric polyps: a retrospective analysis of 26,000 digestive endoscopies. Arq Gastroenterol. 2007; 44: 14-17.
- Camack SW, Genta RM, Schuler CM, Saboorian MH. The current spectrum of gastric polyps: a 1-year national study of over 120,000 patients. Am J Gastroenterol. 2009; 104: 1524-1532.
- Genta RM, Schuler CM, Robiou CI, Lash RH. No association between gastric fundic gland polyps and gastrointestinal neoplasia in a study of over 100,000 patients. Clin Gastroenterol Hepatol. 2009; 7: 849-854.
- Gao W, Huang Y, Lu S, Li C. The clinicopathological characteristics of gastric polyps and the relationship between fundic gland polyps, Helicobacter pylori infection, and proton pump inhibitors. BMC Gastroenterol. 2018; 18: 52.
- Choi KE, Kim MJ, et al. Effects of proton pump inhibitors on pediatric inflammatory esophagogastric polyps. Digestion. 2012; 85: 179-184.
- Jalving M, Koornstra JJ, Wesseling J, Boezen HM, De Jong S, Kleibeuker JH. Increased risk of fundic gland polyps during long-term proton pump inhibitor therapy. Aliment Pharmacol Ther. 2006; 24: 1341-1348.
- Brito HLF, Barros C, et al. Gastric fundic gland polyps: can histology be useful to predict proton pump inhibitors use? Arq Gastroenterol. 2018; 55: 380-384.
- Martin FC, Chenevix-Trench G, Yeomans ND. Systematic review with meta-analysis: fundic gland polyps and proton pump inhibitors. Aliment Pharmacol Ther. 2019; 49: 501-507.
- Jalving M, Koornstra JJ, Wesseling J, Boezen HM, De Jong S, Kleibeuker JH. Increased risk of fundic gland polyps during long-term proton pump inhibitor therapy. Aliment Pharmacol Ther. 2006; 24: 1341-1348.
- Niu JC, Qin Y. Fundic gland polyps: Should my patient stop taking PPIs? Cleve Clin J Med. 2021; 88: 150-153.
- Levy MD, Bhattacharya B. Sporadic fundic gland polyps with low-grade dysplasia: A large case series evaluating pathologic and immunohistochemical findings and clinical behavior. Am J Clin Pathol. 2016; 146: 180-189.
- Brockmeyer JR, Connolly EE, Wittchow RJ, Kothari SN. Resolution of fundic gland polyposis following laparoscopic magnetic sphincter augmentation and subsequent cessation of proton pump inhibitors. Case Rep Gastroenterol. 2015; 2015: 576263.
- Vieth M, Stolte M. Fundic gland polyps are not induced by proton pump inhibitor therapy. Am J Clin Pathol. 2001; 116: 716-720.
- Fukuda M, Ishigaki H, Ban H, et al. No transformation of a fundic gland polyp with dysplasia into invasive carcinoma after 14 years of follow-up in a proton pump inhibitor-treated patient: a case report. World J Gastroenterol. 2021; 27: 149-156.