
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 5
Syphilis mimicking Crohn’s disease: A case report
Freitas Clara RS1; Badaró Pedro FM2; Lisbôa Raísa A, MD3; Silva Nanci F, PhD4; Athanazio Daniel A, MD5; Santana Genoile O, PhD6*
1Medical Doctor, Salvador University, Brazil.
2Medical Student, State University of Bahia, Brazil.
3Medical Gastroenterologist, State University of Bahia, Brazil.
4Medical Infectologist, Aliança Hospital, Brazil.
5Medical Pathologist, Associate Professor, Faculty of Medicine, Federal University of Bahia, IMAGEPAT Laboratory of Pathology, Brazil.
6Medical Gastroenterologist, Associate Professor, State University of Bahia, Brazil.
*Corresponding Author : Santana Genoile Oliveira
State University of Bahia, Salvador 41150-000, Bahia, Brazil.
Tel: +55-71-999572121;
Email: genoile@uol.com.br
Received : Jan 10, 2025
Accepted : Feb 03, 2025
Published : Feb 10, 2025
Archived : www.jjgastro.com
Copyright : © Oliveira SG (2025).
Abstract
Sexually Transmitted Infections (STIs) can often mimic Inflammatory Bowel Disease (IBD) and should always be considered in the differential diagnosis of patients presenting with rectal manifestations. Unfortunately, the symptoms of lower gastrointestinal syphilis are often nonspecific or even absent, making the diagnosis particularly challenging. This case report presents a 35-year-old male patient with anorectal symptoms, highlighting an atypical presentation of syphilis infection.
Keywords: Syphilis; Sexually transmitted infections; Inflammatory bowel disease; Crohn’s disease; Infectious proctitis.
Citation: Clara RSF, Pedro FMB, Raísa AL, Nanci FS, Daniel AA, et al. Syphilis mimicking Crohn’s disease: A case report. J Gastroenterol Res Pract. 2025; 5(1): 1222.
Introduction
Rectal symptoms are frequently associated with Inflammatory Bowel Diseases (IBD) [1]. Since gastrointestinal manifestations of Sexually Transmitted Infections (STI) are common, it is important that clinicians always consider them as differential diagnoses of IBD. However, it is not usually easy to establish it considering nonspecific symptoms or asymptomatic cases [2].
Lower Gastrointestinal Syphilis (LGS) can manifest through a broad spectrum of symptoms, including chancres, proctocolitis with tenesmus and hematochezia, or asymptomatic mucosal abnormalities [4]. The symptomatology of STI commonly mimics IBD with presence of anorectal symptoms including rectal bleeding and mucous discharge, anorectal itching, pain and tenesmus [4]. Therefore, especially when there is a history of receptive anal contact and in IBD cases that do not respond to therapy, exclusion of anorectal infections is indicated as part of standard screening for STIs [1].
Syphilis infection rates have garnered significant attention due to a global rise in incidence, particularly among men who have sex with men [1]. Simultaneously, the epidemiology of IBD has undergone a notable shift, with its prevalence steadily increasing [5]. For instance, Latin America witnessed a rapid rise in IBD incidence in 2020 [6].
Given the growing prevalence of both IBD and syphilis, accurately distinguishing between these conditions is vital for ensuring appropriate patient management. Misdiagnosis of LGS as IBD is not uncommon, often resulting in suboptimal treatment. This challenge is compounded by the rarity of LGS presentations and the absence of pathognomonic symptoms [7].
We present a case of 35-year-old male patient with anorectal ulcers associated with tenesmus, mushy stools mixed with blood and mucus for 2 months. He was being investigated for Crohn’s disease, when anorectal lesions suggestive of syphilis were later observed and investigated. The patient was treated with Benzatinic penicillin and exhibited an excellent response.
Case report
A 35-year-old male was referred for investigation of Crohn’s Disease (CD). He reported changes in bowel habits, including frequent bowel movements, mucus in stool, and hematochezia over the past two months, accompanied by tenesmus. His family history included gastric and rectal cancer, as well as a distant cousin diagnosed with CD.
Physical examination revealed abdominal tenderness in the right lower quadrant and perianal ulcers. At the time of evaluation, the patient was using mesalazine suppositories with no significant improvement in symptoms.
His laboratory results showed normal white blood cell count, normal C-reactive protein level and the lab exams were negative for STIs, including syphilis. A stool analysis identified Blastocystis hominis and fecal calprotectin was high (6679 mg/kg).
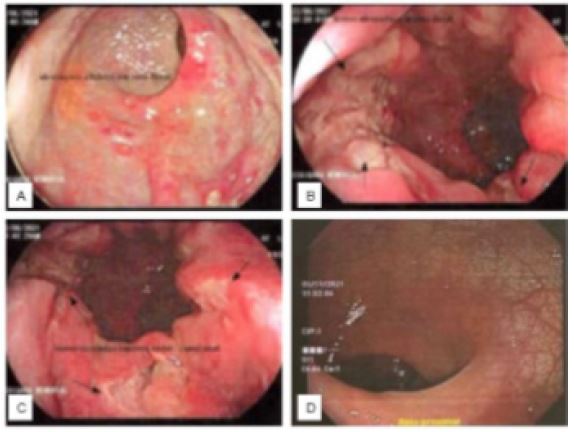
Colonoscopy showed normal appearing mucosa of the terminal ileum and colon, except for anorectal area, which showed ulcerative lesions (Figures 1 A-C). The biopsy showed granulation tissue and neutrophilic exsudate, with fragments of adjacent mucosa with no architecture distortion. Immunohistochemical reactions for cytomegalovirus, herpes I, herpes II and Treponema were negative. A recto sigmoidoscopy performed after two months displayed continuity of the ulcers, in addition to a hyperemic and friable mucosa.
Considering his symptoms and exams results were not suggestive of CD, he was asked about sexual behavior and confirmed having receptive anal contact. More tests for STI were performed: Venereal Disease Research Laboratory (VDRL) title 1/32 and Fluorescent Treponemal Antibody Test Absorption test (FTA-ABS) was positive, while HIV serology was negative.
The patient was treated with two intramuscular Benzatinic penicillin 2.400.000 IU in one week gap and exhibited full regression of all his symptoms plus proctosigmoidoscopy showed a healed mucosa (Figure 1D). A biopsy of this third biopsy showed a normal appearing mucosa with intramucosal hyperplastic lymphoid follicles.
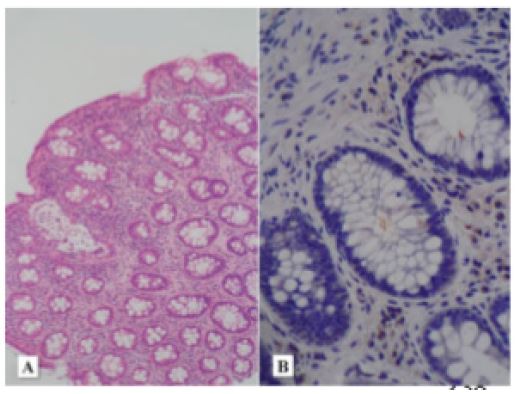
In light of seroconversion and clinical improvement after therapy, we retrospectively performed Treponema immunostain in the second biopsy which was positive for spirochetes (Figures 2A & B).
Discussion
Syphilis, a systemic bacterial infection caused by the spirochete Treponema pallidum, is often called the “great imitator and mimicker” due to its diverse clinical manifestations [8]. In 2022, there was an increase in reported syphilis infections in the United States, with increases over the previous five years reaching 80% [9]. Given its highly varied clinical manifestations, clinicians must remain vigilant for the possibility of syphilis in the differential diagnosis of symptoms involving virtually any organ system and conduct appropriate serologic screening tests.
While investigating IBD it is important to understand the patient’s clinical features, associated signs and symptoms, ask about recent changes of medications, weight loss, dietary habits and recent travels [10]. Detailed sexual history must be obtained at first presentation, while paying attention to risk factors such as HIV seropositive status, other STIs in last 6 months, condomless receptive anal intercourse and history of traumatic sex in last 3 months [3]. These are probably the most powerful tool for estimating the probability of infectious proctitis [3].
Furthermore, it is essential to ask about IBD family history. Physical examination with perianal inspection as well as palpation for adenopathies should not be forgotten during a broad clinical examination [10], for instance, in this case report the inspection of perianal region revealed ulcers, which were essential for diagnosis. If the diagnosis is clearly based on these findings, empirical treatment could be started [2].
Subsequently, analysis of blood sample with specific attention for inflammatory parameters and stool cultures are important [10]. A fecal calprotectin analysis is not usually a screening tool, but in our case, it was performed due investigation of IBD. However, it is not a specific marker, and its high levels are also seen in gastrointestinal infections.
The endoscopic findings of Crohn’s, namely discontinuous distribution of longitudinal ulcers, were not find in this case [11]. Colonoscopy showed normal appearing mucosa of terminal ileum and colon, except for anorectal area, which showed ulcerative lesions. After these findings STI must be investigated, especially when there is a history of receptive anal contact. Additionally, in similar cases reported of syphilitic proctitis, anorectal infections have a varying clinical and endoscopic presentation, making diagnosis difficult [7,10].
While the incidence of syphilis is increasing, anorectal syphilis remains an uncommon presentation with a paucity of cases [12]. Its first appearance can occur after 2-6 weeks of anal sexual intercourse, and in untreated patients. The secondary form can occur 6-8 week after the healing of the initial ulcer. Ulcers are typically located at the anal verge but can also be located more proximally in the rectum [2]. The clinical presentation of syphilitic proctitis can be very atypical, from asymptomatic to mild cases with symptoms like anal pain, tenesmus, itching, anal discharge, rectal bleeding or urgency of defecation. Therefore, syphilitic proctitis is often a missed diagnosis [10].
Anorectal syphilis can be diagnosed by the detection of treponemes in exudate from an ulcerating lesion using darkfield microscopy, or an anorectal mucosal or ulcer swab for Polymerase Chain Reaction (PCR) for Treponema pallidum DNA [1]. However, test can be negative, and it does not exclude syphilis infection. PCR is not widely available. Silver nitrate-based stains (such Warthin-Starry) shows low sensitivity (18%) and Treponema pallidum immunohistochemistry shows a reported sensitivity of 79% [3]. Gummatous lesions are especially likely to stain negative for syphilis, given the paucity of organisms typically found in these late-stage growths, hence the importance of multiple testing modalities [3].
Positive syphilis serological test results support the diagnosis of anorectal syphilis [3], as in this case. A review of 64 cases of Lower Gastrointestinal Syphilis (LGIS) found that 27% of cases were likely primary syphilis, 42% of cases were likely secondary syphilis, and 13% of cases were likely primary or secondary syphilis. These findings suggests that LGIS is most commonly a manifestation of an early infection. It is important to note that signs and symptoms of secondary syphilis may appear before the chancre of primary syphilis has fully healed, and that both stages are known to not infrequently co-occur [3]. This should be investigated and clearly established by physicians, since the stage of this infection has implications in the patient treatment.
Although essential, public health responses to STIs have been inadequate, compounded by challenges such as antimicrobial resistance, drug shortages, and lack of diagnostic tests in low-resource settings. In light of this, WHO has launched a new global strategy for 2022–2030, prioritizing research and innovation to address gaps in the control and prevention of these diseases [13]. As such, differential diagnosis for patients with anorectal diseases is of paramount importance.
While sexually transmitted proctitis represents a small proportion of overall STI cases, it is vital for clinicians to consider STIs as key differential diagnoses in all patients with a new presentation of presumed IBD. Given the absence of definitive diagnostic markers for anorectal syphilis, obtaining a comprehensive sexual history is essential, and empiric treatment may be warranted in complex cases. Failure to diagnose or delays in treatment can significantly impact both individual health and public health outcomes.
Declarations
Conflict of interest: There is no conflict of interest to be declared by the authors.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
References
- de Vries HJC, Nori AV, Kiellberg Larsen H, Kreuter A, Padovese V, Pallawela S, et al. 2021 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. J Eur Acad Dermatol Venereol. 2021; 35: 1434-1443.
- Hoentjen F, Rubin DT. Infectious proctitis: when to suspect it is not inflammatory bowel disease. Dig Dis Sci. 2012; 57: 269-73.
- Ferzacca E, Barbieri A, Barakat L, Olave MC, Dunne D. Lower Gastrointestinal Syphilis: Case Series and Literature Review. Open Forum Infect Dis. 2021; 8: ofab157.
- Zuccati G, Tiradritti L, Lorenzoni E, Giomi B, Mastrolorenzo A. Sexually transmitted diseases syndromic approach: proctitis. G Ital Dermatol Venereol. 2012; 147: 395-406.
- Caron B, Honap S, Peyrin-Biroulet L. Epidemiology of Inflammatory Bowel Disease across the Ages in the Era of Advanced Therapies. J Crohns Colitis. 2024; 18: ii3-ii15.
- Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021; 18: 56-66.
- Vasconcelos P, Borges-Costa J, Loreto H, Marques S. Secondary syphilis mimicking inflammatory bowel disease. Sex Transm Infect. 2013; 89: 98-9.
- Tudor ME, Al Aboud AM, Leslie SW, Gossman W. Syphilis. In StatPearls. StatPearls Publishing. 2024.
- Hufstetler K, Llata E, Miele K, Quilter LAS. Clinical Updates in Sexually Transmitted Infections. J Womens Health (Larchmt). 2024; 33: 827-837.
- Struyve M, Meersseman W, Van Moerkercke W. Primary syphilitic proctitis: case report and literature review. Acta Gastroenterol Belg. 2018; 81: 430-432.
- Lee JM, Lee KM. Endoscopic Diagnosis and Differentiation of Inflammatory Bowel Disease. Clin Endosc. 2016; 49: 370-5.
- Madden Shelby J, Paredes Angelo H, Cho Ryan. The Great Masquerader: Syphilis Presenting as Rectal Ulcer in the Setting of Neurosyphilis. American Journal of Gastroenterology. 2018; 113: S930.
- Gottlieb SL, Spielman E, Abu-Raddad L, Aderoba AK, Bachmann LH, Blondeel K, et al. WHO global research priorities for sexually transmitted infections. Lancet Glob Health. 2024; 12: e1544-e1551.