
Journal of Gastroenterology Research and Practice
Clinical Case - Open Access, Volume 4
Clinical case of a patient with MALT lymphoma not associated with helicobacter pylori
Abilbekova Botakoz Almazovna1*; Khamitova Indira Myktyevna, PhD2; Aliyev Kuanysh Baltashevich3; Umargaliyeva Aigerim Aibekovna4
1Gastroenterologist Consultative and Diagnostic Polyclinic of KGP at the “Pavlodar Regional Hospital named after G.Sultanov”, Pavlodar City.
2Endoscopist, Head of the Endoscopic Centre of the Multidisciplinary Hospital No. 3, Karaganda
3Endoscopist, Head of Endoscopy Department of KGP at the “Pavlodar regional hospital named after G. Sultanov”, Pavlodar city.
4Hematologist Consultative and Diagnostic Polyclinic of KGP at the “Pavlodar Regional Hospital named after G.Sultanov”, Pavlodar city.
*Corresponding Author : Abilbekova B Almazovna
Gastroenterologist, Consultative and Diagnostic Polyclinic of KGP on PCV “G. Sultanov Pavlodar Regional Hospital”, Pavlodar city, Kazakhstan.
Email: botakoz100@inbox.ru
Received : Aug 20, 2024
Accepted : Oct 21, 2024
Published : Oct 28, 2024
Archived : www.jjgastro.com
Copyright : © Almazovna AB (2024).
Abstract
The prevalence of gastric localisation of lymphoma reaches 68-75% of all cases of lesions of the digestive tract. MALT lymphomas develop, as a rule, in people aged 50-60 years, somewhat more often in men, and have a number of specific features.
In 90% of cases, Helicobacter pylori is the factor that stimulates chronic inflammation of the gastric mucosa [1].
Gastric MALT lymphomas have no specific symptoms and in various combinations are manifested by upper abdominal discomfort, anorexia and weight loss, nausea and vomiting, and hidden bleeding [2]. In the described clinical case, the debut of the disease in an 18-year-old female patient was characterised by sideropenic syndrome, and the patient was referred for further investigations to clarify the genesis of anaemia. The final diagnosis of MALT-lymphoma was confirmed by immunohistochemistry (IHC).
Keywords: MALT-lymphoma; Tumour; Anaemia; Stomach; Chemotherapy.
Citation: Almazovna AB, Myktyevna KI, Baltashevich AK, Melnikov VA. Clinical case of a patient with MALT lymphoma not associated with helicobacter pylori. J Gastroenterol Res Pract. 2024; 4(9): 1221.
Introduction
MALT-lymphomas (mucosa-associated lymphoid tissue tumours) are B-cell non-Hodgkin’s lymphomas (NHLs) originating from the marginal zone, along with marginal spleen lymphomas and marginal nodal lymphomas. Moreover, MALT lymphomas are the most common type of marginal zone lymphoma, accounting for 50-70% of all observations [3].
The diagnosis of MALT lymphoma localised in the gastrointestinal tract is usually established by endoscopic examination followed by morphological (histological and immunohistochemical) examination of biopsy material. Macroscopically, 50% of gastrointestinal lymphomas are polyp-like masses, ulcerated forms are somewhat less common, and a very small proportion are ulcerations on an infiltrated base [4].
In terms of treatment, evidence of the etiological role of Helicobacter pylori has radically changed the therapeutic approach to the management of patients, as effective eradication therapy promotes regression of gastric MALT lymphoma. Patients who do not achieve remission after eradication therapy may be treated with chemotherapy using rituximab and oral alkylating agents (chlorambucil, cyclophosphamide) or cytostatics from the group of purine antagonists (cladribine, fludarabine) [5].
We report a clinical case of Helicobacter -negative MALT gastric lymphoma treated with chemotargeted therapy and targeted therapy.
Case presentation
A 19-year-old patient was admitted to the Department of Abdominal Surgery of Multidisciplinary Hospital No. 3 in Karaganda with dyspepsia and asthenia. Gastroduodenoscopy was performed, which revealed lymphoma of the antral region of the stomach complicated by bleeding. Forrest Ib. Emergency hospitalisation.
From anamnesis it is known that the disease debuted 1.5 years ago with the appearance of asthenia, anaemia, sideropenic syndrome and dyspepsia. She adhered to diet, took Omeprazole on an occasional basis.
On examination, blood tests revealed severe iron deficiency anaemia, thrombocytosis (Hv-58 g/l, platelets-440 x 109/l, serum iron 2.5 μmol/l, ferritin-6.80 ng/ml). Long-term continuous ferrotherapy was prescribed.
The patient had no history of chronic diseases, surgical interventions and bad habits. The patient’s mother had peptic ulcer disease.
On physical examination, the temperature is 36.8oC. Skin and visible mucous membranes are pale. Peripheral lymph nodes are not enlarged. No peripheral oedema. Respiratory rate 17 per min.
Heart rate - 93 beats per min. Blood pressure - 110/70 mmHg. Appetite is reduced. The abdomen is regular in shape, soft, slightly painful in the epigastrium. On palpation in the epigastric region, a painful mass of dense consistency of about 5 cm in size is palpated.
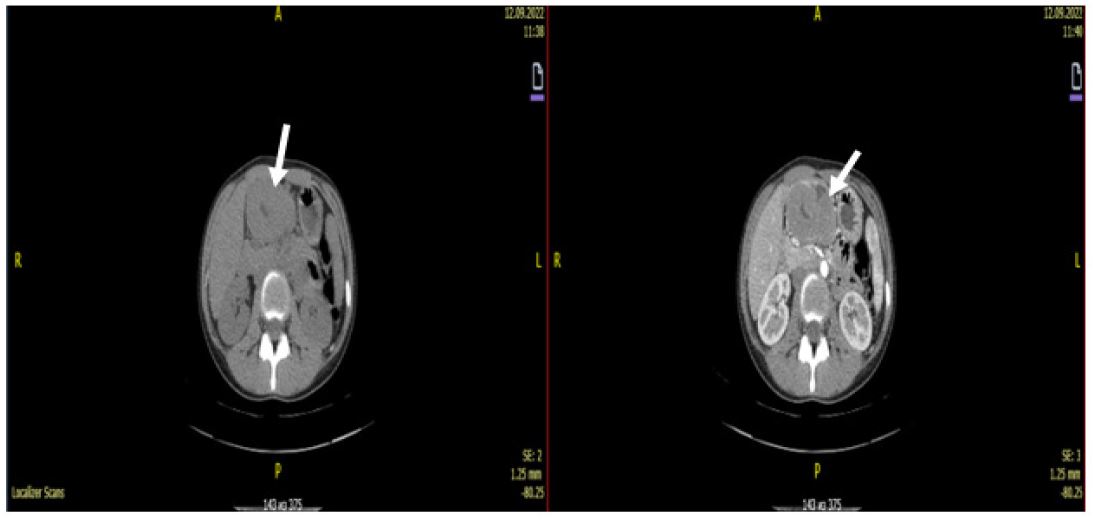
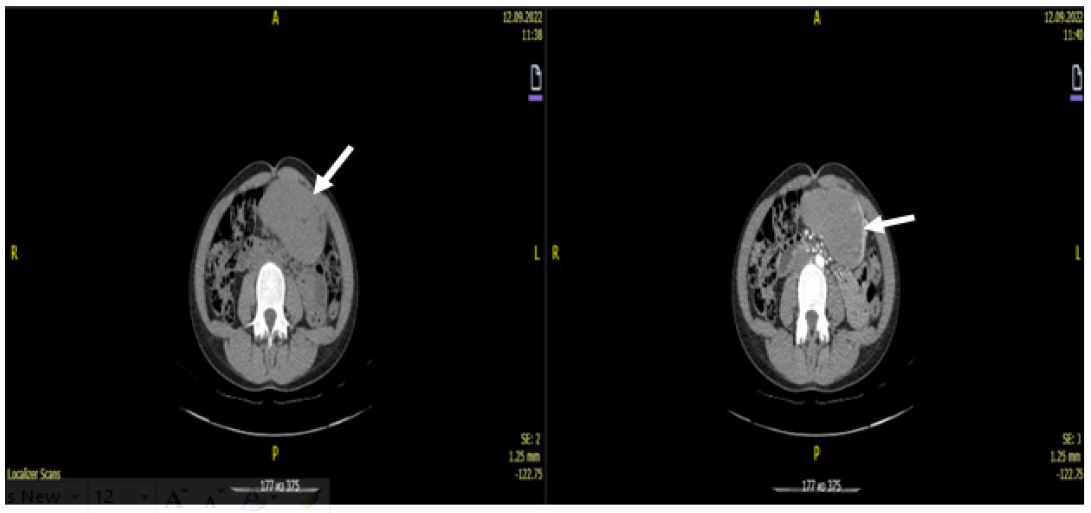
Computed tomography of the abdominal cavity revealed a tumour of the angle and outlet of the stomach (most likely lymphoma), with infiltration of the perigastric tissue (Figures 1,2).
Immunohistochemistry analysis confirmed the diagnosis of MALT lymphoma 9699/3;
AE/AE3 (-). SD-45 (+). SD-20 (+) - 98%.
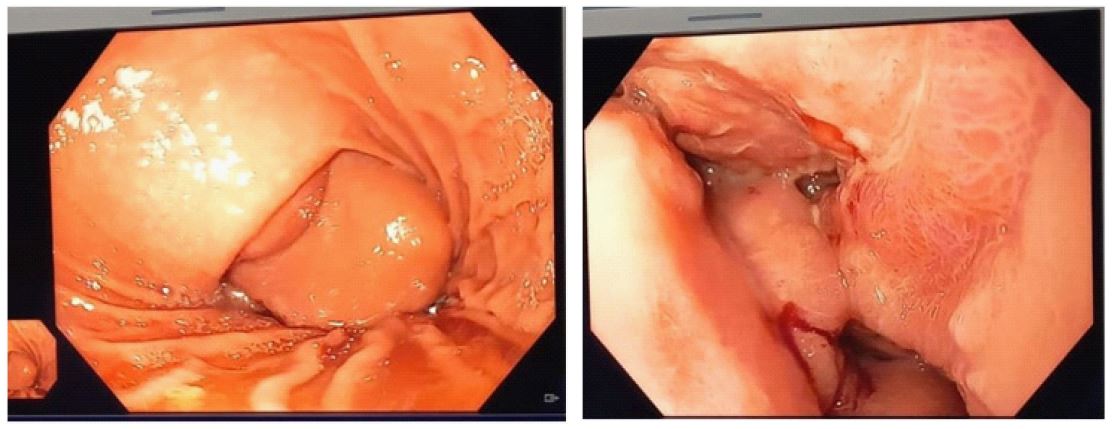
On control gastroduodenoscopy with biopsy: Infiltrative ulcerative lesion of the stomach body and antral region (Figure 3). Helicobacter pylori was not detected.
A consilium was held. Taking into account the stage of the disease and histological findings, it was recommended to carry out chemotherapy in mono-mode with rituximab. 3 courses of target therapy with rituximab were carried out. After the treatment positron emission tomography was performed, according to the data of which negative dynamics and progression were observed. Taking into account the progression of the disease, satisfactory condition, young age, chemotargeted therapy according to the R-CHOP scheme was indicated.
Positive dynamics in the form of increased appetite, weight gain of 4 kg, reduction of tumour size from 18.0 cm to 8.0 cm) were observed during treatment. The patient underwent 7 courses of chemotargeted therapy R-CHOP (Rituximab, Endoxan, Doxilide, Vincristine, Prednisolone). She was discharged with improvement. As a result of the treatment, complete regression of the tumour process was noted. Taking into account the young age, large size of the primary tumour, despite the complete regression of radiopharmaceutical accumulation according to positron emission tomography data, it is recommended to increase the number of cycles of chemotargeted therapy up to 8 with the following maintenance therapy with rituximab once every 2 months.
The patient completed her 12th course of TT with Rituximab.
Conclusion
The etiological connection between the development of gastric MALT-lymphoma and the presence of chronic Helicobacter-associated gastritis was not confirmed by cytological examination. In order to make a more accurate diagnosis, Helicobacter pylori antigen analysis in faeces was recommended.
Tumour diseases of the stomach, in particular those originating from the lymphoid tissue of the organ mucosa, may proceed without specific clinical manifestations even at advanced stages of the disease. Reasons for the appointment of imaging studies of the abdominal cavity organs are changes in the picture of pre-existing chronic gastritis and anaemia as part of the principle of oncological caution of the doctor [4].
References
- Selezneva E.Ya., Shcherbakova N.A., EmbutnieksYu.V., Bystrovskaya E.V. et al. Diagnosing MALT gastric lymphoma in gastroenterologist’s practice, a clinical observation. Russian Journal of Gastroenterology, Hepatology, Coloproctology. 2021; 31(3): 60–7. (in Russian)]. DOI: 10.22416/1382-4376-2021-31-3-60-67
- Izrailov RE, Pomortsev BA, Semenov NE, Pivnik AV. A complicated form of extranodal gastric lymphoma. Modern possibilities of surgical treatment. Rare clinical case. Endoscopic Surgery. 2020; 26(1): 35 39. (In Russ.)
- Dasaev NA, Larin SV, Kurganov IA, Baĭbakova TI. MALT-lymphoma of the small bowel complicated by perforation and peritonitis. Endoscopic Surgery. 2012; 18(4): 36 38. (In Russ.)
- Julai G.S., Julai T.E. MALT-lymphoma of the stomach in a patient with chronic gastritis associated with Helicobacter pylori. Dr.Ru. 2022; 21(6): 45-48. DOI: 10.31550/1727-2378-2022-21-6-45-48
- Thieblemont C, Zucca E. Clinical aspects and therapy of gastrointestinal MALT lymphoma. Best Pract Res Clin Haematol. 2017; 30(1-2): 109-117. doi: 10.1016/j.beha.2017.01.002. Epub 2017 Jan 30. PMID: 28288705.