
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 4
Pulmonary embolization of cyanoacrylate following endoscopic therapy for gastric variceal bleeding: A case report
Hanen Jaziri1*; Ines Lassoued1; Amani Derbel1; Nawress Boudguiga1; Amira Ben Afia2; Wafa Dahmani1; Aya Hammami1; Aida Ben Slama1; Ahlem Brahem1; Nour Eleuch1; Mehdi Ksiaa1
1Department, Sahloul Hospital, Sousse, Tunisia.
2Department, Sahloul Hospital, Sousse, Tunisia.
*Corresponding Author : Hanen Jaziri
Gastroenterologiy Department, Sahloul Hospital, Sousse, Tunisia.
Tel: 0021623895030;
Email: jazirihanen@yahoo.fr
Received : Sep 18, 2024
Accepted : Oct 17, 2024
Published : Oct 24, 2024
Archived : www.jjgastro.com
Copyright : © Jaziri H (2024).
Abstract
Upper Gastrointestinal Hemorrhage (UGIH) due to bleeding from gastric varices is a rare but life-threatening complication of portal hypertension. We present a case of a 48-year-old female who developed massive pulmonary embolism following endoscopic injection therapy with N-butyl-2-cyanoacrylate for bleeding gastric varices. Despite successful initial hemostasis, the patient experienced sudden respiratory distress post-procedure, leading to the diagnosis of bilateral non-thrombotic pulmonary embolism. Management included intravenous steroids and supportive care, resulting in gradual clinical improvement and eventual discharge. This case underscores the importance of recognizing and managing rare complications associated with cyanoacrylate therapy in portal hypertension patients.
Citation: Jaziri H, Lassoued I, Derbel A, Boudguiga N, Afia AB, et al. Pulmonary embolization of cyanoacrylate following endoscopic therapy for gastric variceal bleeding: A case report. J Gastroenterol Res Pract. 2024; 4(9): 1220.
Introduction
Upper Gastrointestinal Hemorrhage (UGIH) resulting from bleeding gastric fundal varices is a rare and life-threatening complication of portal hypertension. Although gastric varices bleed less frequently than esophageal varices, bleeding from Gastric fundal Varices (GV) tends to be more severe and is associated with a high mortality rate [1].
Endoscopic variceal ligation has become a well-established treatment for esophageal varices. In contrast, for gastric varices, many clinicians consider endoscopic therapy with the tissue adhesive cyanoacrylate (N-butyl-2-cyanoacrylate) to be the optimal initial treatment due to its efficacy [2,3]. However, glue embolization, a rare complication with reported incidences ranging from 0.5% to 4.3% [4], remains relatively unfamiliar to many physicians.
We present a case involving pulmonary embolization of N-butyl-2-cyanoacrylate following endoscopic injection therapy for gastric variceal bleeding.
Case report
A 48-year-old female, with no significant medical or surgical history, presented to the emergency department with a 2-day history of coffee-colored vomiting and melena.
Upon admission, her vital signs were stable, and both her respiratory and cardiovascular systems were normal. Physical examination revealed she was conscious, cooperative, with normal lung findings and mild splenomegaly.
Laboratory testing revealed a hemoglobin level of 10 g/dl, a leukocyte count of 4.5x109/l, a platelet count of 90x109/l, a prothrombin ratio of 75%, a serum creatinine level of 55 μmol/l, urea levels of 6.4 mmol/L, albumin levels of 32 g/L, bilirubin levels of 15 μmol/L, alkaline phosphatase levels of 100 μ/L and alanine transaminase levels of 70 μ/L.
The electrocardiogram and chest radiography were normal.
The patient received intravenous Sandostatin and proton pump inhibitors. Upper GI endoscopy revealed mild portal hypertensive gastropathy and a large gastric varix with red signs in the fundus, extending to involve esophageal varices (GOV 2), as per Sarin classification (Figure 1) [3]. Endoscopic sclerotherapy was performed with an injection of 1.5 ml N-Butyl-2-cyanoacrylate (Glubran®) diluted (50/50) with lipiodol into the fundic varix with red signs, under general balanced anesthesia. Airway management and intubation were uneventful. Injection sclerotherapy achieved successful hemostasis, maintaining stable hemodynamic and respiratory status throughout the procedure.
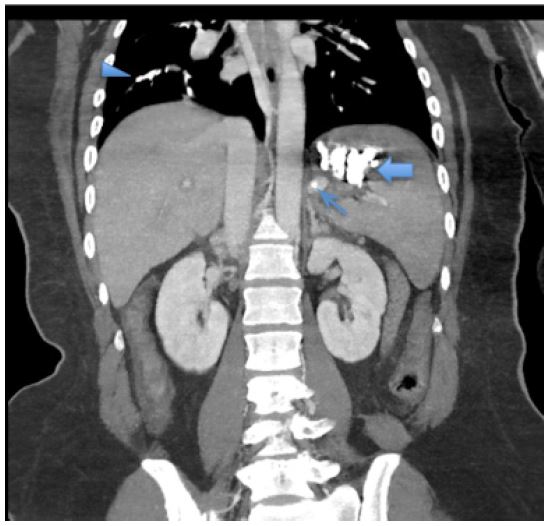
Following the procedure, there was a drop in oxygen saturation and development of tachycardia. The patient was subsequently intubated, ventilated, and transferred to a monitored setting. Thoracic CT angiography revealed bilateral massive non-thrombotic pulmonary embolism with dense infiltrates in pulmonary arterial areas affecting all segmental arterial branches. Embolization material was noted in the splenic vein (Figure 2). Intravenous steroids (dexamethasone 6 mg/day for 2 days, then gradually decrease by 2 mg every 2 days) and supportive management were initiated. Over the next two days, the patient’s oxygen requirements gradually decreased. She was successfully weaned off ventilation, extubated, and discharged home.

Discussion
Gastrointestinal bleeding is a common and serious complication among patients with portal hypertension, affecting approximately twenty percent who develop gastric or fundic varices. Although these varices generally pose a low bleeding risk, hemorrhage from ruptured gastric varices can be more severe due to the intensity of bleeding at this site. Moreover, achieving hemostasis in such cases with procedures like band ligation or sclerotherapy is notably challenging and often less effective [4].
N-butyl-2-cyanoacrylate, a biological adhesive, rapidly polymerizes upon contact with ionized materials such as blood, plasma proteins, or endothelial surfaces, forming a local vessel clot. Radiopaque substances like lipiodol are mixed with the adhesive to monitor and visualize the injection site, thereby slowing down its polymerization process [5].
The use of N-acetyl cyanoacrylate glue for gastric variceal obliteration has been standardized since its initial description in 1986 [6]. Complications associated with Fundal Varix Obturation (FVO) procedures include fever, recurrent bleeding, chest pain, and ulceration. More severe complications, such as embolization to cerebral arteries, portal vein, lung, and splenic arteries, have also been documented [7].
Systemic embolization is believed to primarily occur via the gastrorenal and splenorenal veins, as observed in this patient. Another potential pathway for paradoxical glue embolization is through an atrial septal defect. Involvement of the splenic vasculature with histoacryl (NBC) compromises splenic perfusion, potentially leading to splenic infarction [8].
The manifestations of pulmonary glue embolism vary widely, ranging from asymptomatic cases to symptoms such as dyspnea, pleuritic chest pain, coughing, tachycardia, hypoxia, and in severe cases, cardiorespiratory arrest or sudden death. Onset of symptoms can vary greatly, occurring anywhere from minutes to days after the injection. Pulmonary edema and chemical acute respiratory distress syndrome can also result from this condition [9,10].
CT pulmonary angiography is the preferred imaging method for diagnosing this condition, effectively visualizing foreign material within the branches of the pulmonary artery with the aid of iodine-containing contrast agents [10].
The risk of embolization is associated with factors including variceal size, injection speed, presence of perisplenic portosystemic shunts, total volume injected, and the ratio of sclerosant components [11]. Strategies to prevent glue embolization include using rapidly polymerizing pure glue or employing coil placement guided by endoscopic ultrasound before administering the glue injection [12].
Treatment primarily involves supportive care, as most emboli typically resolve spontaneously on radiographic imaging over time. Current evidence does not support the use of anticoagulation or thrombolysis in these cases [12].
Steroids may be considered for treating lipiodol pneumonitis, as lipiodol is thought to induce pneumonitis by breaking down into free fatty acids, triggering an inflammatory response that leads to capillary leakage and pulmonary edema [13].
Conclusion
Gastric variceal bleeding remains a critical issue in patients with portal hypertension, often necessitating complex interventions such as endoscopic cyanoacrylate therapy. While effective in achieving hemostasis, this treatment carries risks, including rare but serious complications like pulmonary embolization. Awareness among clinicians of these potential complications and strategies for prevention and management is crucial for optimizing patient outcomes. Further studies are warranted to refine treatment protocols and enhance safety in managing gastrointestinal bleeding associated with portal hypertension.
Funding: No funding support.
Conflicts of interest: No conflict of interest.
References
- Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: A long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992; 16: 1343-9.
- Park WG, Yeh RW, Triadafilopoulos G. Injection therapies for variceal bleeding disorders of the GI tract. Gastrointest Endosc. 2008; 67: 313-23.
- Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: A long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992; 16: 1343-9.
- Saraswat VA, Verma A. Gluing gastric varices in 2012: Lessons learnt over 25 years. J Clin Exp Hepatol. 2012; 2: 55-69.
- Kazi S, Spanger M, Lubel J. Gastrointestinal: Pulmonary embolism of cyanoacrylate glue following endoscopic injection of gastric varices.J Gastroenterol Hepatol. 2012; 27: 1874.
- Soehendra N, Nam VC, Grimm H, et al. Endoscopic obliteration of large esophagogastric varices with bucrylate. Endoscopy. 1986; 18: 25-26.
- Tan YM, Goh KL, Kamarulzaman A, Tan PS, Ranjeev P, et al. Multiple systemic embolisms with septicemia after gastric variceal obliteration with cyanoacrylate. Gastrointest Endosc. 2002; 55: 276-8.
- Kurt M, Onal IK, Ibis M, Tas A, Ozderin YO, Okten RS. Splenic infarction: rare complication of N-butyl-2-cyanoacrylate injection for gastric varices. Dig Endosc. 2010; 22: 74-75.
- Michael P, Antoniades G, Staicu A, Seedat A. Pulmonary glue embolism complication following endoscopic slerotherapy for gastric varices. Sultan Quaboos Univ Med J. 2018; 18: 231‑5.
- Embolism and pulmonary oedema as a rare complication after endovascular embolization of oesophageal varices. BMJ Case Report. 2020; 13: e233654.
- Alexander S, Korman MG, Sievert W. Cyanoacrylate in the treatment of gastric varices complicated by multiple pulmonary emboli. Intern Med J. 2006; 36: 462-5.
- Hameed F, Pepperell J, Sidney J. A rare complication of endoscopic intervention. Breathe (Sheff). 2018; 14(2): e40-e42
- Parthiv Amin, Tania Pannu. Nonthrombotic pulmonary embolism secondary to cyanoacrylate embolization of gastric varices. CMAJ. 2022; 194: E336-7.