
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Minimally invasive esophagectomy: Divide the azygos only if you have to!
Athish Shetty; Vageesh BG*; Amit Javed; Anil Agarwal
Department of Gastrointestinal Surgery, GB Pant Hospital and MAM College, Delhi University, New Delhi, India.
*Corresponding Author : Vageesh BG
Department of Gastrointestinal Surgery, GB Pant Hospital and MAM College, Delhi University, New Delhi, India.
Email: bgvageesh@yahoo.com
Received : Sep 11, 2024
Accepted : Oct 07, 2024
Published : Oct 14, 2024
Archived : www.jjgastro.com
Copyright : © Vageesh BG (2024).
Abstract
Background: Esophageal cancer is currently being treated with Minimally Invasive Esophagectomy, and has gained wide popularity in recent years. During the McKeown-MIE procedure, the azygos arch is routinely ligated to facilitate lymph node dissection and esophagus mobilization. In this study, we aim to compare the short-term outcomes of ligation and preservation of azygos vein in minimally invasive esophagectomy.
Methods: We conducted a comprehensive retrospective review of the prospectively maintained clinical data of patients with esophageal cancer who underwent Minimally Invasive Esophagectomy at our institution between January 2011 and December 2023. Patients were assigned to one of two groups depending on whether the azygos arch was preserved or not: 1) Preservation group and 2) Transection group. Post operative outcomes were then compared between the two groups.
Results: There was no significant difference in operative time, intra-operative blood loss, number of lymph nodes dissected and major post-operative complications. Preservation group had relatively lower total post-operative ICD drainage (565 vs 728 ml) and earlier ICD removal (4.1 vs 5.2 days) (p=0.04). However, post-operative hospital stay was similar between the 2 groups.
Conclusion: The results of the study showed that preservation of arch of azygos vein in minimally invasive esophagectomy is safe and feasible with comparable outcomes. It also led to decreased post-operative thoracic drainage which may enhance early recovery of the patients. However, the long-term advantages in the form of reduced dilatation of the gastric tube and better positioning of the conduit will need to be explored in further long-term studies.
Citation: Shetty A, Vageesh BG, Javed A, Agarwal A. Minimally invasive esophagectomy: Divide the azygos only if you have to!. J Gastroenterol Res Pract. 2024; 4(9): 1219.
Introduction
Esophageal cancer is one of the most common gastrointestinal cancers around the world, causing an estimated 5% of all cancer related deaths [1]. Multimodal approaches with surgery as cornerstone have emerged as the treatment of choice for esophageal cancer [2]. Totally Minimally Invasive Esophagectomy and Hybrid esophagectomy are currently being practised as standard of care [3]. Of all the MIE approaches, the McKeown-MIE procedure is one of the most popular among surgeons [4].
The azygos system serves as an important connection between the superior and inferior venae cavae. It also creates a vital collateral pathway that becomes a shunt in cases of obstruction of the major pathways. During the McKeown-MIE procedure, the azygos arch is routinely ligated to facilitate lymph node dissection and esophagus mobilization. Sparing of the azygos arch has the potential benefits of maintaining mediastinal venous reflux and reduces the tubular gastric expansion and malpositioning [5].
In this study, we aim to compare the short-term outcomes of ligation and preservation of azygos vein in minimally invasive esophagectomy.
Materials and methods
A retrospective review was performed of all patients with oesophageal cancer who were managed surgically in the Department of Gastrointestinal Surgery at our centre, which is a tertiary referral institution, between January 2011 and December 2023. The data were extracted from a prospectively maintained oesophageal disease database.
All patients with suspected oesophageal cancer were made to undergo an upper gastro-intestinal endoscopy and biopsy. Staging was routinely done by a contrast-enhanced Computed Tomography (CT) scan of the chest and the abdomen. Positron Emission Tomography (PET) scan was done selectively. Those with metastatic disease underwent palliative treatment. Patients with mid and lower thoracic esophagus tumors who underwent surgery were included in the analysis. Neoadjuvant chemo(radio)therapy was offered to patients prior to surgery after discussion in multidisciplinary meeting.
All patients with resectable tumours and those who were deemed fit to undergo surgery were started on a pulmonary physiotherapy programme that included deep-breathing exercises, steam inhalation and incentive spirometry. In patients who were nutritionally depleted or had complete dysphagia, a pre-operative nasogastric tube was inserted for nutritional build-up.
Surgical approach
The surgical approach included a staged MIE which started with thoracoscopic oesophageal mobilisation, with an en bloc lymph nodal dissection followed by laparoscopic gastric mobilisation and cervical oesophagogastric anastomosis.
Thoracoscopic mobilisation
Each patient was intubated in the supine position and then positioned prone on the operating table. The right hemi-thorax was accessed through one camera port and two working ports for the surgeon. The inferior pulmonary ligament was divided and the inferior pulmonary vein was safeguarded. Peri-oesophageal dissection was begun with an incision on the mediastinal pleura over the lower end of the oesophagus. The oesophagus was mobilised starting from the lower oesophagus and gradually moving upwards. The peri-oesophageal lymph nodes were excised en bloc with the specimen. Moving from below up, the sub-carinal lymph nodes were dissected with the specimen, taking care not to injure the bronchus. Right and the left recurrent laryngeal nerves were identified and preserved. Following completion of the oesophageal mobilisation and lymph nodal dissection, an intercostal chest drain was inserted.
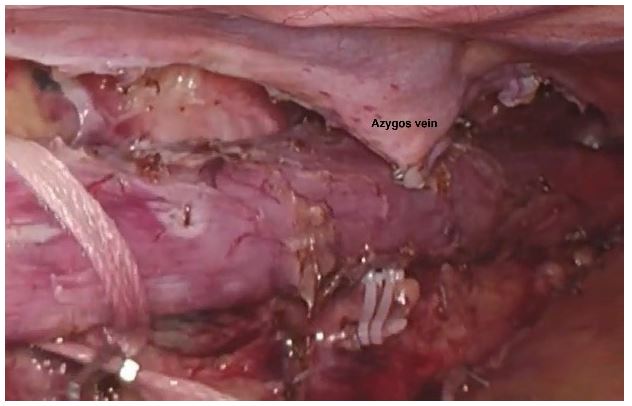
The patients were divided into two groups based on whether the arch of azygos vein was preserved (Preservation group/AVP) (Figure 1) or transected (Transected group/AVT) (Figure 2). During esophageal mobilisation, the azygos vein was either suture-ligated, clipped (using a hem-o-lok) or divided using a laparoscopic stapler with a vascular cartridge in the Transected group.

Laparoscopic mobilisation and cervical esophagogastric anastomosis
After completion of the thoracoscopic phase, the patients were positioned supine. The stomach was mobilised with preservation of the right gastro-epiploic vessel and the right gastric vascular arcade. Lymph nodes along the hepatic artery and left gastric artery were dissected. The specimen was retrieved either through a small abdominal incision or via the cervical incision. An approximately 5 cm portion of the stomach in the region of the the fundus was left undivided. This facilitated the delivery of the specimen and the conduit into the neck by applying gentle traction on the divided upper oesophageal end. Once the specimen had been delivered out through the cervical incision, the gastric conduit formation was completed by dividing the attached cardiac portion of the stomach using a linear cutting stapler. The gastric tube was pulled up into the neck via the posterior mediastinal route. A side-to-side, stapled or hand-sewn cervical oesophagogastric anastomosis was performed. A feeding jejunostomy was inserted.
The post-operative analgesia included epidural, intravenous opioids and Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). Patients were started on a physiotherapy programme. Chest tube outputs were monitored and were removed when the lung was fully expanded and the output decreased to ≤100 mL/day. Enteral feeds were started via the feeding jejunostomy catheter on day 2 and the oral diet was initiated by day 3-4. Patients were kept under follow up for a minimum period of 3 months.
Observation indexes
Perioperative observation indexes included operative time, intraoperative blood loss, tumor size, and the number of lymph nodes dissected. Postoperative indicators included postoperative thoracic drainage volume, chest drainage time, postoperative hospital stay time, the incidence of postoperative complications (swallowing dysfunction, cervical oesophagogastric anastomotic leaks, thoracic duct injury, hoarseness of voice); and histopathology (type of tumour, stage of disease and number of lymph nodes harvested).
Statistical analysis
IBM SPSS Statistics v29.0 statistical software was used. Categorical variables were compared using Fisher’s exact test and continuous variables were compared using the Mann-Whitney test. The statistics for all the variables were analyzed. A P value of < 0.05 was considered to be statistically significant.
Results
During the study period, between January 2011 and December 2023, 145 patients were planned for Minimally Invasive Esophagectomy. In 14 patients a laparoscopic transhiatal oesophagectomy was done, and these were excluded from the study. In 10 patients, the procedure was converted to open in view of adherence to carina and left bronchus and were excluded from the analysis. Out of the 121 patients who underwent McKeown-MIE, 32 patients were in the Azygos Vein Preservation group (AVP group) and 89 patients were in the Azygos Vein Transected group (AVT group).
The median age of the study population was 54 (24-79) years and was comparable in the two groups (P=0.8). There were 65 males and 56 females. 45 patients had tumours located in the middle third of the oesophagus, 60 in the lower third, and 16 in the gastro-oesophageal junction. The most commonly observed histology was squamous cell cancer (75.2%). The location of the tumour, histology, and the number of patients who received neo-adjuvant treatment were similar in the two groups (Table 1). The median duration of surgery and intra-operative blood loss was similar in the two groups. The incidence of other post-operative complications, including cervical oesophagogastric anastomotic leak, swallowing dysfunction, hoarseness of voice and chylothorax, was not different in the two groups. No mortality was noted in the follow up period of 3 months.
A median of 14 lymph nodes (range 4-34) were retrieved in Preservation group, and 16 (range 6-39) lymph nodes were retrieved in the Transected group (p=0.12).
Preservation group had relatively lower total post-operative ICD drainage (565 vs 728 ml) and earlier ICD removal (4.1 vs 5.2 days) (p=0.04). However, post-operative hospital stay was similar between the 2 groups (Table 2).
Table 1: Demographic and tumor profile.
| Parameter | Preservationgroup (AVP) (32) | Transectiongroup (AVT) (89) | P value |
|---|---|---|---|
| Age | 53±8.2 yrs | 55±9.1 yrs | 0.8 |
| Tumor site | |||
| Upper third | - | - | |
| Middle third | 10 | 35 | 0.62 |
| Lower third | 18 | 42 | 0.51 |
| G E junction (type1/2) | 4 | 12 | 0.13 |
| Histological type | |||
| Adenocarcinoma | 9 | 21 | 0.64 |
| Squamous cellcarcinoma | 23 | 68 | 0.77 |
| Tstage | 0.34 | ||
| T1 | 4 | 8 | |
| T2 | 14 | 31 | |
| T3 | 14 | 49 | |
| T4 | 0 | 1 | |
| Nstage | 0.22 | ||
| N0 | 12 | 37 | |
| N1 | 18 | 43 | |
| N2 | 2 | 9 | |
| N3 | 0 | 0 | |
| Neo-adjuvant therapy | 29 | 74 | 0.35 |
Table 2: Intra and post-operative outcomes.
| Parameter(Mean) | Preservationgroup (AVP) (32) | Transectiongroup (AVT) (89) | P value |
|---|---|---|---|
| Duration of surgery (mins) | 321±46 mins | 308±42mins | 0.68 |
| Intra-operative bloodloss | 112±34 ml | 96±33 ml | 0.14 |
| Lymph node yield | 14±9.1 | 16±10.3 | 0.12 |
| Positive lymph nodes | 2±1.2 | 3±1.5 | 0.31 |
| Complications | |||
| Swallowing dysfunction | 3 | 09 | 0.82 |
| Anastomotic leak | 4 | 11 | 0.78 |
| Hoarseness of voice | 5 | 13 | 0.67 |
| Thoracic ductinjury | 5 | 7 | 0.22 |
| SSI | 10 | 19 | 0.24 |
| Post-op thoracic drainage | 565±185 ml | 728±225 ml | 0.04 |
| ICDremoval (Post op day) | 4.1±2.1 days | 5.2±3.2 days | 0.04 |
| Post-op Hospital stay | 8.1±3.2 days | 8.4±3.8 days | 0.66 |
Discussion
In the current era, multidisciplinary assessment and planning of treatment are mandatory for esophageal cancer. Treatment is determined together with the patient based on histological subtype, clinical TNM stage, tumour location and the patient’s predicted treatment tolerance, which considers performance status and comorbidities [6].
The azygos arch is an important structure in the vicinity of esophagus. It is formed from the junction of the right subcostal veins and the ascending lumbar veins. In addition to receiving the right posterior intercostal veins, the azygos vein also communicates with the vertebral venous plexus that drains the back, vertebrae, and structures in the vertebral canal. It also receives the mediastinal, esophageal, and bronchial veins, the hemi-azygos vein, and the accessory hemi-azygos vein [7].
The arch of azygos is routinely transected during the McKeown-MIE procedure as it was believed to assist with the esophageal dissociation and lymphatic clearance. However, this may hinder the mediastinal venous reflux, increase the volume of pleural effusion and aggravate tissue oedema [8]. In addition, the venous arch provides an anatomical “banding” effect on the esophagus, which is lost after transection. After being pulled upward from the abdomen to the neck, the denervation of the vagus nerve and the negative pressure of the thoracic cavity, the tubular stomach usually has varying degrees of expansion or dilation, which may cause gastric retention and respiratory aspiration. Further, the expanded conduit may affect the blood supply of the gastric surgical margin with the potential risk of gastric fistula [9].
In most of the cases, the amount of intra operative bleeding is small and can be controlled with energy devices and gauze packing. In cases with more severe bleeding, conversion to thoracotomy can be life-saving and should be done immediately when indicated. According to the previous studies, the incidence of azygos vein injury is reported to be about 0.45% to 0.87% during open surgery for esophageal cancer [10]. For patients with large tumors located near the azygos arch, the vein arch should be transected routinely. There was no azygos vein injury noted in any of the patients during gastric pull-up in our study. Transection of azygos vein does not necessarily provide a safe passage during pull-up.
In the present study, the thoracic drainage volume in the preservation group was significantly less than that in the transection group, which may be attributable to the sparing of the azygos arch. However, there are other multiple factors which also play an important role in determining the ICD output like the size of the tumor, thoracic duct injury during surgery, pulmonary function etc which were similar between the two groups.
The preservation of azygos arch did not reduce the lymph node yield as there was no statistical difference between the number of lymph nodes retrieved. Patients who had their azygos arch preserved, had relatively earlier ICD removal. However, there is no significant difference in short term outcomes in terms of post-operative stay, post-operative complications and intraoperative or post operative bleed due to preservation of azygos vein.
Patients who undergo esophagectomy with gastric conduit reconstruction are at risk of complications such as delayed gastric emptying, reflux, and dysphagia, which sometimes can seriously affect patients’ quality of life. The diameter and malposition rate of the gastric conduit may have a role to play in determining these outcomes. Thus, more research needs to be conducted in the future to further analyse the significance of the azygos arch-sparing technique on the long-term postoperative course.
Conclusion
The results of the study showed that preservation of arch of azygos vein in minimally invasive esophagectomy is safe and feasible with comparable outcomes. It also led to decreased post-operative thoracic drainage which may enhance early recovery of the patients. However, the long-term advantages in the form of reduced dilatation of the gastric tube and better positioning of the conduit will need to be explored in further long-term studies.
References
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68: 394-424. 10.3322/caac.21492
- Nguyen NT, Follette DM, Wolfe BM, Schneider PD, Roberts P, et al. Comparison of minimally invasive esophagectomy with transthoracic and transhiatal esophagectomy. Arch Surg. 2000; 135: 920-5.
- Low DE, Kuppusamy MK, Alderson D, Cecconello I, Chang AC, et al. Benchmarking Complications Associated with Esophagectomy. Ann Surg. 2019; 269(2): 291-298.
- Deng J, Su Q, Ren Z, et al. Comparison of short-term outcomes between minimally invasive McKeown and Ivor Lewis esophagectomy for esophageal or junctional cancer: A systematic review and meta-analysis. Onco Targets Ther. 2018; 11: 6057-69. 10.2147/OTT.S169488
- Li H, Lin J, Zhang H, Wu B, Chen Y, et al. A propensity score matching study of the short-term efficacy of azygos arch-sparing McKeown minimally invasive esophagectomy. Journal of gastrointestinal oncology. 2021; 12(1): 28-37.
- Obermannová R, Alsina M, Cervantes A, Leong T, Lordick F, et al. Oesophageal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Annals of Oncology. 2022; 33(10): 992-1004.
- Donohue JR, Daly DT. Anatomy, Thorax, Azygos Veins [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing. 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554430/
- Cui X, He Y, Chen L, et al. Clinical Analysis of Azygos Vein Preservation Under Thoracoscope in the Operation of Type III Esophageal Atresia. J Laparoendosc Adv Surg Tech A. 2020; 30: 448-52.
- Meyerson SL, Mehta CK. Managing complications II: conduit failure and conduit airway fistulas. J Thorac Dis. 2014; 6 Suppl 3: S364-71.
- Zhang X, Li D, Luo J, et al. Management of accidents during operation of esophageal or cardiac cancer. The Practical Journal of Cancer. 2003; 18: 195-7.