
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 4
Gastric mucormycosis post COVID-19
Heullys F Silva1*; Erb G Cambrainha Monteiro1; Bruna R Nascimento Silva2; Osmundo B Xavier2; Romualdo C Lins Filho3
1Endoscopy, Hospital Mestre Vitalino, Caruaru, Brazil.
2Internal Medicine, Hospital Mestre Vitalino, Caruaru, Brazil.
3Pathology, Hospital Mestre Vitalino, Caruaru, Brazil.
*Corresponding Author : Heullys F Silva
Endoscopy, Hospital Mestre Vitalino, Caruaru, Brazil.
Email: heullys3@hotmail.com
Received : Sep 02, 2024
Accepted : Oct 01, 2024
Published : Oct 08, 2024
Archived : www.jjgastro.com
Copyright : © Silva HF (2023).
Abstract
Mucormycosis is a serious disease caused by fungi of the Mucorales order Mucorales. The main risk factors of mucormycosis include diabetes mellitus, phagocyte deficiency, corticosteroid use and organ or stem cell transplantation. More recently, COVID-19 has become a risk factor described in some case reports, increasing the importance of diagnostic suspicion in patients with COVID-19 and clinical signs compatible with mucormycosis. We report a case of a 32-year-old man, an active alcoholic for approximately 20 years, with signs of malnutrition, without other previous comorbidities, that was admitted to the emergency room with respiratory failure, associated with flu-like symptoms, requiring orotracheal intubation and admission to the intensive care unit. During his stay in the intensive care unit, the patient developed upper gastrointestinal bleeding, with melena and a drop in hemoglobin. An upper digestive endoscopy was requested, which showed an ulceroinfiltrative lesion in the fundus and gastric body. Biopsies of the lesion were performed, which demonstrated active, ulcerated chronic inflammation, with numerous short and irregular segments of hyphae amidst necrotic debris, without cellular atypicality, findings characteristic of mucormycosis. Treatment with Amphotericin B was chosen for 14 days. After the end of treatment, a new upper gastrointestinal endoscopy demonstrated healing of the gastric lesion, without new episodes of upper gastrointestinal bleeding or other gastrointestinal symptoms.
Citation: Silva HF, Monteiro EGC, Silva BRN, Xavier OB, Filho RCL. Gastric mucormycosis post COVID-19. J Gastroenterol Res Pract. 2024; 4(8): 1217.
Introduction
Mucormycosis is a serious disease caused by fungi of the Mucorales order Mucorales [1]. The main risk factors of mucormycosis include diabetes mellitus, phagocyte deficiency, hematological malignancies, corticosteroid use and organ or stem cell transplantation [2]. More recently, COVID-19 has emerged a risk factor described in some case reports, increasing the importance of diagnostic suspicion in patients with COVID-19 and clinical signs compatible with mucormycosis [3-7].
Mucormycosis can affect any organ system, although the nasal sinuses, orbit, and brain (rhino-orbitalcerebral) or the lung are the most commonly affected. The stomach is the most common site of gastrointestinal mucormycosis, followed by the colon and ileum. Symptoms of gastrointestinal mucormycosis vary depending on the afflicted location [8]. The most prevalent symptoms are nonspecific abdominal discomfort and distention accompanied by nausea and vomiting. Fever and hematochezia are also possible. The patient is frequently misdiagnosed with an intra-abdominal abscess.
Case presentation
A 32-year-old man, an active alcoholic, with consumption of around 150 grams of alcohol per day for approximately 20 years, with signs of malnutrition, body mass index of 15, without comorbidities, was admitted to the emergency room with respiratory failure, oxygen saturation of 88% in non-rebreathing oxygen mask, associated with flu-like symptoms, requiring orotracheal intubation and admission to the Intensive Care Unit (ICU). After admission, a RT-PCR for COVI19 was carried out, which was positive. Chest tomography demonstrated the presence of a diffuse ground-glass infiltrate, bilaterally, affecting >50% of the lung area. The patient had not previously been vaccinated for COVID-19.
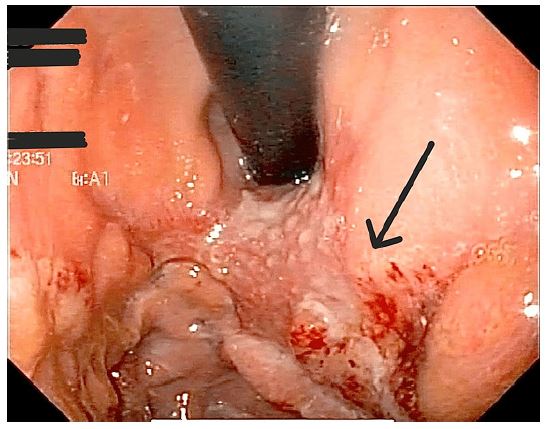
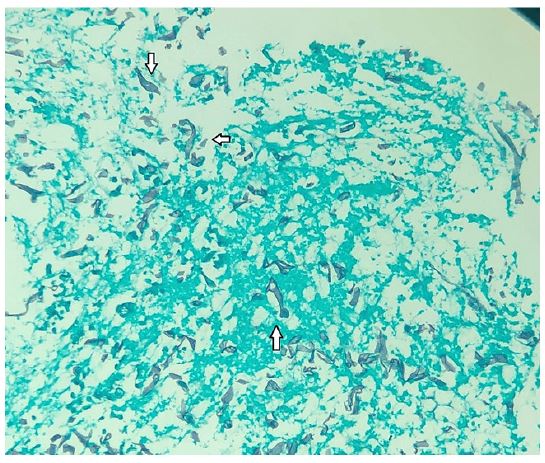
During his stay in the intensive care unit, he was treated with ceftriaxone and azithromycin, however his white blood cell count increased (Table 1), and clinical condition worsened, requiring an escalation of the antimicrobial spectrum to piperacillin and tazobactam (4,5 g qid) over the following two weeks, and later meropenem (1G tid) associated with teicoplanin (400 mg sid). In addition, the patient developed oliguria and renal dysfunction secondary to septic shock, requiring renal replacement therapy with hemodialysis. After 2 weeks in ICU, the patient developed upper gastrointestinal bleeding, with melena and a drop in hemoglobin. An upper digestive endoscopy was requested, which showed an ulceroinfiltrative lesion in the fundus and gastric body, measuring approximately 70 mm, and no signs of active bleeding and no need for endoscopic therapy (Figure 1). Biopsies of the lesion were performed, which demonstrated active, chronic ulcerated inflammation, with numerous short and irregular segments of hyphae amidst necrotic debris, without cellular atypicality, findings suggestive of mucormycosis (Figure 2).
Table 1: Laboratory data during hospitalization.
| Reference range | ICU admission | 7days after admission | 14days after admission | 60 days afteradmission | |
|---|---|---|---|---|---|
| Hemoglobin (g/dl) | 13-17 | 11 | 9.8 | 6.3 | 8.8 |
| White blood cells(per ul) | 4.000-10.00 | 8,789 | 21.853 | 12.456 | 7.231 |
| Neutrophils (%) | 40-60% | 76% | 88% | 81% | 60% |
| Eosinophils (%) | 1-4% | 4% | 3% | 4% | 3% |
| Lymphocytes (%) | 20 - 40 % | 10% | 6% | 9% | 25% |
| Platelets | 150-450 x 109/L | 221 x 109/L | 101 x 109/L | 115 x 109/L | 280 x 109/L |
| Creatinine (mg/dl ) | 0.5-1.2 | 0.8 | 7.6 | 4.7 | 1.8 |
| Blood urea nitrogen (mg/dl) | 7 -20 | 18 | 120 | 32 | 25 |
| AST (U/I) | 12-37 | 159 | 164 | 141 | 78 |
| ALT ( U/I ) | 15-65 | 125 | 132 | 108 | 53 |
| C-reactive protein (mg/dl) | 0.5 - 1.0 | 8.4 | 18.3 | 9.8 | 1.6 |

After the diagnosis of mucormycosis, by histopathological analysis, treatment with Amphotericin B liposomal (3 mg/kg/day) was chosen for 14 days. After the end of treatment, a new upper gastrointestinal endoscopy demonstrated marked improvement of the gastric lesion (Figure 3), without new episodes of upper gastrointestinal bleeding or other gastrointestinal symptoms. The patient improved clinically from COVID-19, with extubation after 12 days, and discharge from the ICU, with hospital discharge approximately 2 months after admission. Currently, he remains well clinically, undergoing outpatient follow-up.
Discussion
Due to the rarity of the diagnosis of gastric mucormycosis, we had several difficulties in reaching the final diagnosis, with the need to rule out the numerous differential diagnoses, such as gastrointestinal tuberculosis, which has a significant incidence in Brazil. Fortunately, the histopathological finding of irregular and short segments of hyphae, amidst necrotic tissue, and absence of other findings, caught the attention of the pathology team and medical team. With consideration of the diagnosis of gastric mucormycosis, given the risk factors presented by our patient. Enabling the start of specific treatment and subsequent patient improvement.
Cases of mucormycosis associated with COVID-19 have attracted attention since the beginning of the pandemic, although the gastrointestinal form is not the most common, some cases have already been reported in the literature. Our case demonstrates a patient with some risk factors classically associated with mucormycosis, alcoholism, malnutrition and prolonged ICU stay, these are factors that appear to have contributed to the development of gastric mucormycosis [9].
COVID-19 patients may have significantly increased levels of inflammatory cytokines (such as IL-2R, IL-6, IL-10, and tumor necrosis factor-alpha), which is associated with poor cell-mediated immune response, affecting both CD4 + T and CD8 + T cells. As a result, there is an increased propensity to fungal coinfections [10].
Gastric mucormycosis typically presents on endoscopy as a large ulcer with necrosis that later develops into an adherent, thick, green exudate [11]. Diagnosis is confirmed by histopathologic identification based on the biopsy of the suspected area during surgery or endoscopy, specifically in borders and central part of the lesions [6]. The disease has a high fatality rate (up to 85%) related to late or no diagnosis [12].
Because serologic exams are non-specific, a biopsy of the lesions suspect or the affected area is the gold standard for obtaining a histologic diagnosis of mucormycosis [13,14]. On occasion, a positive culture or Polymerase Chain Reaction (PCR) result on a biopsy specimen is needed to confirm the diagnosis. The major choice for treating gastrointestinal mucormycosis is treatment with antifungal medication, such as lipid formulations of amphotericin B, posaconazole, and newer drugs isavuconazole or triazole [14].
Our case demonstrates the need to be alert to common complications in critically ill patients, with risk factors for uncommon diseases, such as mucormycosis, which, if not diagnosed and treated in time, almost always has a fatal outcome. GI mucormycosis is an uncommon condition that should be explored if a COVID-19 patient develops an unusual stomach ulcer. As a result, if symptoms like, digestive hemorrhage with the presence of large gastric ulcerations on endoscopy, in a patient with risk factors, suggestive of mucormycosis, preemptive medication should be considered. More research is needed to discover whether these two illnesses are connected.
Conclusion
Mucormycosis is a serious disease caused by fungi, and COVID-19 has emerged as a significant risk factor. It is critical to be aware of the risk factors for mucormycosis and to evaluate this diagnosis in the presence of clinical symptoms and unusual imaging results. Because serologic tests are non-specific, a biopsy of the suspected lesions or afflicted area is the gold standard for achieving a histologic diagnosis of mucormycosis. Antifungal medications, such as lipid formulations of amphotericin B, posaconazole, and newer medications; isavuconazole or triazole, are the primary therapeutic options for gastrointestinal mucormycosis.
Declarations
Human subjects: Consent was obtained by all participants in this study.
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work.
Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
References
- Hibbett DS, Binder M, Bischoff JF, et al. A higher-level phylogenetic classification of the Fungi. Mycol Res. 2007; 111: 509-547. 10.1016/j.mycres.2007.03.004
- Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin Infect Dis. 2005; 41: 634-653. 10.1086/432579
- Sayan Malakar, Anshuman Elhence1, Pallavi Prasad, et al. Primary gastric mucormycosis presenting with post‑Coronavirus disease ‑ 19 upper gastrointestinal bleed. Indian J Surg. 2022; 84: 545-547. 10.1007/s12664022-01298-5
- Brad Spellberg. Gastrointestinal Mucormycosis: An Evolving Disease. Gastroenterol Hepatol (N Y. 2012; 8: 140-142.
- Verma V, Acharya S, Kumar S, et al. Rhinocerebral Mucormycosis With Brain Abscess Presenting as Status Epileptucus in a COVID-19-Infected Male: A Calamitous Complication. Cureus. 2022; 14: 21061. 10.7759/cureus.21061
- Patel M, Talwar D, Kumar S, Acharya S, Dubey A, et al. Cutaneous mucormycosis with maxillary sinus fistula as a presenting feature of COVID- 19: A rare case report. Medical Science. 2021;25: 1507-1512.
- Kumar S, Acharya S, Jain S, et al. Role of Zinc and Clinicopathological Factors for COVID-19-Associated Mucormycosis (CAM) in a Rural Hospital of Central India: A Case-Control Study. Cureus. 2022; 14: 22528. 10.7759/cureus.22528
- Song G, Liang G, Liu W. Fungal co-infections associated with global COVID-19 pandemic: A clinical and diagnostic perspective from China. Mycopathologia. 2020; 185: 599-606. 10.1007/s11046-020-00462-9
- Shah D, Talwar D, Kumar S, Acharya S, Dubey A. Mucormycosis as a complication of LONG COVID: A case series. Medical Science. 2021; 25: 1331-1337.
- Monte ESD, Santos MELD, Ribeiro IB, et al. Rare and fatal gastrointestinal mucormycosis (Zygomycosis) in a COVID19 patient: A case report. Clin Endosc. 2020; 53: 746-9. 10.5946/ce.2020.180
- Ayushi Sharma, Anjana Goel. Mucormycosis: risk factors, diagnosis, treatments, and challenges during COVID-19 pandemic. Folia Microbiol Praha. 2022; 67: 363-387. 10.1007/s12223-021-00934-5
- Dimitrios P Kontoyiannis, Russell E Lewis. How I treat mucormycosis. Blood. 2011; 118: 5. 10.1182/blood-2011-03-316430
- Meshram V, Jadhav D, Kanchan T, et al. Autopsy Approach in diagnosis of mucormycosis. J Indian Forensic Med. 2022; 44: 44-7. 10.5958/0974-0848.2022.00014.8
- FM Marty, L Ostrosky-Zeichner. Isavuconazole treatment for mucormycosis: A single-arm open-label trial and case-control analysis. The Lancet Infectious Diseases. 2016; 16: 837. 10.1016/S1473-3099(16)000712