Journal of Gastroenterology
Research and Practice
Clinical Image - Open Access, Volume 4
Dysphagia lusoria: A rare vascular anomaly
Raakhi Menon1*; Eric Margulies2; Brooke Corning2
1Department of Internal Medicine, Division of General Internal Medicine, University of Texas Medical Branch, USA.
2Department of Internal Medicine, Division of Gastroenterology and Hepatology, University of Texas Medical Branch, USA.
*Corresponding Author : Raakhi Menon
Department of Internal Medicine, Division of General Internal Medicine, University of Texas Medical Branch, USA.
Tel: (409) 747-1883;
Email: rsmenon@utmb.edu
Received : Aug 03, 2024
Accepted : Aug 29, 2024
Published : Sep 05, 2024
Archived : www.jjgastro.com
Copyright : © Menon R (2024).
Citation: Menon R, Margulies E, Corning B. Dysphagia lusoria: A rare vascular anomaly. J Gastroenterol Res Pract. 2024; 4(8): 1213.
Description
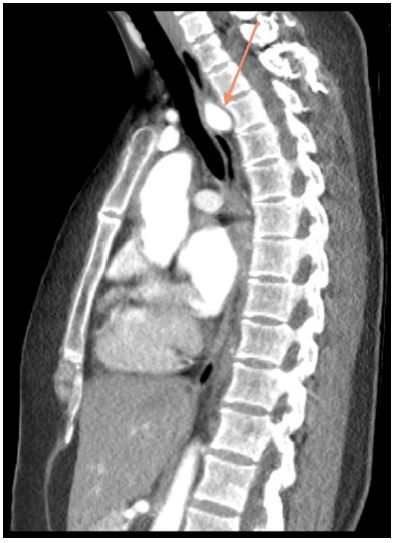
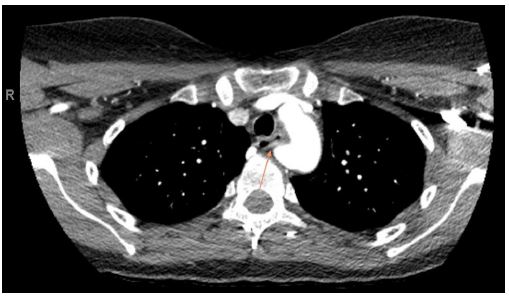
A 39-year-old female with a past medical history of chronic bronchitis presented for evaluation of progressive dysphagia. She reported a long-standing history of difficulty swallowing, often experiencing transient substernal obstruction of solid food and occasionally liquids. Her symptoms subsequently progressed until she was tolerating only minimal oral intake accompanied by unintentional weight loss, prompting her to seek care. A barium esophagram revealed a 2.7 cm extrinsic compression in the upper esophagus. A CT angiogram of the chest identified an aberrant right subclavian artery compressing the esophagus. An Esophagogastroduodenoscopy (EGD) confirmed extrinsic compression in the upper third of the esophagus, consistent with suspected dysphagia lusoria. Esophageal biopsy showed normal mucosa. She underwent right subclavian to carotid transposition and Thoracic Aneurysm Endovascular Repair (TAVER). At a follow-up assessment two weeks postoperatively, she reported complete resolution of dysphagia.
Dysphagia lusoria is a rare condition that occurs secondary to extrinsic esophageal compression by an aberrant right subclavian artery [1]. An aberrant right subclavian artery has a prevalence of 0.16-4.4% [2]. This anomaly is symptomatic in about 30% of cases identified by Figure 2. Dysphagia is the most common related symptom, reported in 90% of cases [1,2]. Other reported symptoms include cough, dyspnea, and chest pain [3].