
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 4
Diagnosis and management of type III gastric neuroendocrine tumor: Recent advances
Tan Minh Le1,2; Jin Woong Cho3*
1Department of Biomedical Science, Graduate School, Kyungpook National University, Daegu, Republic of Korea.
2BK21 Four Program, School of Medicine, Kyungpook National University, Daegu, Republic of Korea.
3Department of Internal Medicine, Presbyterian Medical Center, Jeonju, Republic of Korea.
*Corresponding Author : Jin Woong Cho
Department of Internal Medicine, Presbyterian Medical
Center, Jeonju, Republic of Korea.
Email: jeja-1004@daum.net
Received : May 08, 2024
Accepted : May 28, 2024
Published : Jun 04, 2024
Archived : www.jjgastro.com
Copyright : © Woong Cho J (2024).
Abstract
Gastric Neuroendocrine Tumors (NETs) encompass a heterogeneous group of neoplasms arising from enterochromaffin-like cells in the gastric mucosa. Among the various subtypes, type III gastric NETs represent a clinically and biologically distinct entity characterized by their aggressive behavior and unique histopathological features. This review aims to provide an overview and update on diagnosis and management of type III gastric NETs. In general, type III gastric NETs present diagnostic and therapeutic challenges due to their nonspecific clinical manifestations and heterogeneous biological behavior. Advances in diagnostic modalities, including endoscopic techniques, and molecular profiling, have improved our understanding of the pathogenesis and classification of type III gastric NETs, facilitating more accurate diagnosis and risk stratification. Treatment strategies for type III gastric NETs encompass a multimodal approach, including endoscopic/surgical resection, medical therapy, peptide receptor radionuclide therapy, and chemotherapy, tailored to the individual patient’s tumor characteristics and stage of disease. Endoscopic resection has emerged as a valuable therapeutic option for select cases of well-differentiated lesions confined to the mucosal or submucosal layers, offering the advantages of minimal invasiveness and preservation of gastric function.
Keywords: Neuroendocrine tumor; Carcinoid; Type III; Stomach.
Citation: Minh Le T, Woong Cho. Diagnosis and management of type III Gastric neuroendocrine tumor: Recent advances. J Gastroenterol Res Pract. 2024; 4(6): 1204.
Introduction
Gastric Neuroendocrine Tumors (NETs) arise from Enterochromaffin-Like (ECL) cells in the stomach, representing a subset of rare tumors that make up 5-15% of all gastrointestinal NETs, less than 2% of all gastric neoplasms [1,2]. Notably, their incidence has exhibited an upward trend in recent years, largely attributed to the widespread adoption of endoscopic techniques [3,4].
Type III gastric NETs constitute a minority within this subgroup, accounting for approximately 15-25% of cases [1]. These tumors are classified according to the International Agency for Research on Cancer and World Health Organization (WHO) classification, which stratifies them into grades based on the proliferative index assessed by mitotic count and/or Ki-67 [5]. Additionally, Rindi et al. introduced a classification system that further refines these tumors based on clinical, pathological, and biological characteristics [6,7].
Among the subcategories, types I, II, and III are the most commonly use in clinical practice. Type I gastric NETs often accompany chronic atrophic gastritis, characterized by elevated serum gastrin levels and achlorhydria, typically presenting as multiple lesions with a relatively benign course. Type II NETs are commonly associated with Multiple Endocrine Neoplasia type 1 (MEN1) syndrome, marked by hypergastrinemia and heightened gastric acid secretion. While less aggressive than type III, they still pose a moderate risk of distant metastases [1,6,7].
Type III tumors represent the most aggressive subtype, and distinct from types I and II by their lack of association with hypergastrinemia, atrophic gastritis, or MEN1 syndrome [1]. Typically solitary and sporadic, type III lesions are characterized by larger sizes and a more aggressive biological behavior, featuring deeper invasion into the stomach wall, lymphovascular infiltration, and a heightened risk of metastasis at diagnosis [6,7].
Given their aggressive nature, consensus guidelines advocate for robust management strategies for type III gastric NETs. While North American guidelines advocate for partial gastrectomy and lymphadenectomy irrespective of grade or size, European Neuroendocrine Tumor Society (ENETS) recommendations allow for endoscopic resection in select cases, particularly for small, superficial lesions [1,8].
This review aims to consolidate current knowledge and recent advancements in type III gastric NETs, offering insights into their diagnostic approaches and therapeutic modalities. By synthesizing existing literature, we endeavor to enhance comprehension and refine management strategies for this challenging malignancy.
Classification
The most widely used classification systems for type III gastric NETs include the WHO classification and the Rindi et al. classification, which provide valuable frameworks for understanding the heterogeneity of gastric NETs [5,6].
WHO classification [5]: Categorizes gastric NETs into three grades based on mitotic rate and Ki-67 proliferative index: Grade 1 (<2 mitoses per 10 high-power fields, <3% Ki-67), Grade 2 (2-20 mitoses, 3-20% Ki-67), Grade 3 (>20 mitoses or >20% Ki67), indicating aggressiveness and prognosis.
Rindi et al. classification [1,6]: Further subdivides gastric NETs into three types based on clinical and pathological features (Table 1). Type I: Associated with autoimmune atrophic gastritis and hypergastrinemia. These tumors are typically multiple, small, and indolent, with a low risk of metastasis. Type II: Associated with MEN1 syndrome and hypergastrinemia due to a gastrinoma. These tumors are usually larger and have a higher risk of metastasis compared to type I tumors. Type III: Represent the most aggressive subtype of gastric NETs, characterized by solitary, sporadic lesions with a high mitotic rate, deep invasion, lymphovascular infiltration, and an increased risk of metastasis. Type III gastric NETs are not associated with hypergastrinemia or autoimmune gastritis.
Table 1: Gastric neuroendocrine tumor types.
| Characteristic | Type I | Type II | Type III |
|---|---|---|---|
| Prevalence | 70-80% | 5-10% | 15-25% |
| Etiology | Associated with chronic atrophic gastritis or autoimmune gastritis |
Associated with Zollinger-Ellison syndrome, MEN-1 |
Sporadic occurrence |
| Gastrin levels | Elevated | Elevated | Normal |
| Gastric pH | Low | high | Normal |
| Number of lesions | Multiple lesions | Multiple lesions | Sporadic lesion |
| Prognosis | Very good, often indolent progres- sion |
Limited data. May involve aggressive behavior than Type I. Overall survival is likely influenced by the underlying MEN1 syndrome |
Often deep gastric layer invasion and high meta- static potential at diagnosis. Generally, survival outcomes are poor except for early stages. |
While the current classifications of gastric NETs has been valuable for diagnosing and stratifying patients, further subclassification of type III gastric NETs is essential to accurately characterize these tumors and tailor treatment strategies to individual patients. Recent studies have identified potential factors for this purpose.
Circulating tumor mRNA and microRNAs present promising avenues for improved diagnosis and stratification of gastric NET type III. The NETest, a liquid biopsy method, demonstrates high sensitivity and specificity in diagnosing gastric NETs, including type III tumor, potentially aiding in surveillance with further validation [9]. MicroRNAs, notably miR-222, show promise as tissue-specific biomarkers, offering insights into treatment response, particularly to gastrin/CCK2R antagonist therapy [10]. Moreover, immunohistochemical biomarkers like PD-L1 and MSI emerge as predictors of response to immune checkpoint inhibitor therapy, with high PD-L1 expression observed in gastric NECs, suggesting immunotherapy as a potential treatment avenue [11,12].
Recent investigations into long-term PPI use shed light on type III gastric NETs characteristics [13]. According to Trinh et al., patients with prolonged PPI usage tend to develop less aggressive gastric NETs with a better prognosis compared to sporadic type III tumors. Notably, tumors in long-term PPI users were confined to mucosal or submucosal layers, with reduced invasion, lymph vascular involvement, metastasis, or mortality risks [13]. This underscores the role of long-term PPI factor in the stratification and management of Type III gastric NETs.
Diagnosis
The clinical presentation of type III gastric NETs is diverse and often nonspecific, posing challenges in diagnosis and differentiation from other gastric neoplasms. Patients with type III tumors may present with a wide range of symptoms, including abdominal pain, dyspepsia, gastrointestinal bleeding, weight loss, and obstructive symptoms such as nausea and vomiting. Furthermore, the clinical manifestations of type III gastric NETs can vary depending on tumor size, location, and extent of local invasion or metastasis [14]. Therefore, the diagnostic process typically involves a comprehensive approach that includes clinical evaluation, endoscopic assessment, radiological imaging, and biochemical testing.
Endoscopic assessment
Endoscopy serves as a cornerstone in the initial assessment of patients suspected of harboring gastric NETs, facilitating visual inspection of the tumor and acquisition of biopsy specimens for subsequent histological evaluation [1]. Type III tumors tend to emerge as solitary, larger lesions, distinguishing them from the multifocal distribution and smaller size characteristic of type I and II gastric NETs. Moreover, type III gastric NETs may appear as hard, yellow and hypoechoic subepithelial lesions (Figure 1), ulcerated masses, or polypoid lesions on endoscopic examination [15]. Their features frequently mimic other gastric neoplasms like adenocarcinomas or gastrointestinal stromal tumors [14].
In addition to standard esophagogastroduodenoscopy, Endoscopic Ultrasound (EUS) may be employed for a more detailed assessment of tumor depth [1,8] (Figure 1), although there is currently no universally defined size threshold prompting this procedure. Typically, lesions smaller than 8-10 mm may not be suitable for fine needle biopsy during EUS, and those smaller than 5 mm might pose challenges for endosonographic visualization. EUS offers the potential advantages of identifying muscularis propria invasion, which could preclude complete endoscopic resection, as well as assessing lymphadenopathy. While EUS is recommended for type I and II disease as dictated by clinical need, the ENETS suggests EUS for type III disease to assess lymphadenopathy and tumor depth. If deemed resectable, the preferred approach is either endoscopic or surgical resection, though international guidelines lean toward endoscopic resection, particularly for superficial lesions measuring less than one centimeter with “low-grade” histology [1,8].

Histopathological diagnosis
Type III gastric NETs, classified as well-differentiated neuroendocrine carcinomas, exhibit distinctive histopathological features indicative of their aggressive behavior and malignant potential [6,7]. Histological examination of type III tumors reveals a mixed phenotype characterized by both neuroendocrine and glandular differentiation [16,17]. Common histological patterns observed in type III gastric NETs include trabecular, glandular, or solid growth patterns, with nests or clusters of tumor cells surrounded by fibrovascular stroma [16,17].
Immunohistochemical staining plays a crucial role in confirming the neuroendocrine differentiation of gastric NETs, including type III tumors. Positive staining for neuroendocrine markers such as chromogranin A, synaptophysin, insulinoma-associated protein 1, and neuron-specific enolase is typically observed, supporting the diagnosis of a NET [18,19]. Synaptophysin, while highly sensitive, lacks full specificity and can be expressed in some non-NETs. Chromogranin A, on the other hand, is highly specific but slightly less sensitive than synaptophysin. Insulinoma-associated protein 1 demonstrates high specificity and sensitivity [5]. Additionally, assessment of the mitotic rate and Ki-67 proliferative index aids in grading the tumor and determining its aggressiveness, with high-grade tumors exhibiting rapid growth and increased metastatic potential [5].
Biochemical assessment
Biochemical assessment, such as serum chromogranin A, gastrin, 24-hour urinary 5-hydroxyindoleacetic acid (5-HIAA) level, and serum 5-HIAA measurement, plays a role in evaluating tumor burden and associated functional abnormalities. Elevated serum chromogranin A levels can be observed in patients with type III gastric NETs, serving as valuable biomarkers for monitoring disease progression and treatment response [18,19]. In line with this, 5-HIAA is recognized as a specific marker, although with diminished sensitivity compared to chromogranin A. Its elevation typically occurs during later stages of the disease, coinciding with metastatic occurrences [20]. Regarding gastrin level, while type I and II gastric NETs often exhibit high gastrin levels, those with type III NETs typically maintain gastrin levels within the normal range [7].
Despite their significance, interpreting the results of these biochemical tests can be challenging due to various factors such as tumor-specific peptide expression, secretion efficiency, and differences between tissue and circulating biomarkers. Furthermore, considerations regarding test availability, cost, and potential confounders like renal insufficiency should be taken into account when using biochemical tests [5].
Also, it is crucial to consider the influence of PPIs on gastrin levels. Concurrent or recent PPI use can artificially elevate gastrin levels, necessitating discontinuation of PPIs for at least one week before obtaining fasting gastrin levels [21]. Nevertheless, abrupt withdrawal of PPIs in cases of suspected Zollinger-Ellison syndrome can lead to severe consequences, such as gastrointestinal perforation [22]. Therefore, replacing PPIs with histamine H2-receptor antagonists 1-2 weeks before formal testing is recommended. The H2-receptor antagonist should be administered every 6 hours and then discontinued in the final 24-30 hours before testing. Antacids may be utilized as needed until midnight before testing [23].
Carcinoid syndrome
Carcinoid syndrome often occurs in NETs originating from the midgut [24]. In type III gastric NETs, carcinoid syndrome is more prevalent in cases with extensive hepatic metastases. It manifests as a paraneoplastic syndrome due to the secretion of serotonin and kallikrein by carcinoid tumors [25]. Typical symptoms include flushing, diarrhea, and abdominal pain, while atypical manifestations like bronchoconstriction may occur due to histamine release [25].
Management
The management of type III gastric NETs requires a multidisciplinary approach tailored to the individual patient’s tumor characteristics, stage of disease, and overall health status. Treatment strategies for type III gastric NETs aim to achieve local control of the tumor, alleviate symptoms, prevent complications, and improve long-term outcomes.
Endoscopic resection
Endoscopic resection has emerged as an important therapeutic modality in the management of select cases of type III gastric NETs, particularly for small, superficial lesions confined to the mucosal or submucosal layers of the gastric wall. Endoscopic resection techniques, including Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD), offer the advantages of minimal invasiveness, preservation of gastric anatomy and function, and rapid recovery compared to surgical resection. Compare to EMR, ESD is an advanced endoscopic technique that allows for en bloc resection of larger, flat or sessile lesions involving the mucosal and submucosal layers of the gastric wall. ESD enables precise dissection along the submucosal plane, facilitating the complete removal of type III gastric NETs with minimal risk of tumor fragmentation or recurrence (Figure 2). ESD is particularly useful for the resection of larger lesions (>10 mm) or those with suspected submucosal invasion, enabling accurate staging and histological evaluation of tumor margins.
According to ENET guideline [1], endoscopic resection is suitable for patients with localized type III grade 1 gastric NETs ≤10 mm in size. In certain situations, larger tumors with a Ki67 index of less than 10% may also be eligible for endoscopic resection, particularly when surgical risks are high, under the condition that thorough staging is conducted to ensure appropriateness.

Surgery
Surgery remains the cornerstone of treatment for localized or resectable type III gastric NETs. Total or subtotal gastrectomy is performed together with lymphadenectomy, as recommended in gastric adenocarcinomas. For patients with localized grade 1/2 type III gastric NETs and no evidence of lymphadenopathy on preoperative imaging, a limited wedge resection with local nodal sampling (without standard lymphadenectomy) can be considered [1]. According to ENET and NCCN guideline: radical surgical resection with lymphadenectomy is recommended for type III gastric NETs when regional lymph nodes are detected or suspected on preoperative staging, or if the Ki-67 index is >20% or tumor diameter exceeds 20 mm [1,26].
Systemic therapy
Medical therapy
In cases of unresectable or metastatic type III gastric NETs, systemic medical therapy plays a crucial role in controlling tumor growth, alleviating symptoms, and improving quality of life [1,8,26]. Somatostatin analogs, such as octreotide and lanreotide, are commonly used as first-line therapy to inhibit neuroendocrine hormone secretion and slow tumor progression [1,26]. Additionally, targeted agents, including everolimus and sunitinib, may be considered for patients with advanced disease refractory to somatostatin analogs, targeting signaling pathways implicated in tumor growth and angiogenesis [1,26].
Peptide Receptor Radionuclide Therapy (PRRT)
PRRT with radiolabeled somatostatin analogs, such as lutetium-177 (^177Lu)-DOTATATE or yttrium-90 (^90Y)-DOTATOC, has emerged as a promising therapeutic option for patients with unresectable or metastatic type III gastric NETs expressing somatostatin receptors [1,26,27]. PRRT delivers targeted radiation to tumor cells expressing somatostatin receptors, resulting in tumor cytotoxicity and regression [28]. PRRT has been shown to prolong progression-free survival and improve quality of life in patients with advanced neuroendocrine tumors, including type III gastric NETs [28].
Chemotherapy
Cytotoxic chemotherapy may be considered for patients with advanced or metastatic type III gastric NETs refractory to other treatment modalities [1,26]. Regimens incorporating platinumbased agents (e.g., cisplatin, carboplatin) in combination with etoposide or fluoropyrimidines (e.g., 5-fluorouracil, capecitabine) have demonstrated efficacy in some patients, albeit with limited response rates and modest survival benefits [29].
Symptom management
Palliative care and symptom management are integral components of the management of type III gastric NETs, particularly in patients with advanced or metastatic disease [1,26]. Symptomatic relief may be achieved through the use of PPIs to control gastric acid secretion, antidiarrheal medications to manage diarrhea, and analgesics to alleviate pain. Nutritional support and dietary modifications may be necessary to address malnutrition and weight loss associated with advanced disease.
Surveillance and follow-up
Localized type III gastric NETs amenable to curative resection have a more favorable prognosis, with 5-year survival rates 50- 100% [4,14,30,31]. However, the prognosis declines significantly for patients with advanced or metastatic disease. Therefore, vigilant surveillance and follow-up are paramount for monitoring disease trajectory and treatment response. This includes regular clinical assessments, biomarker testing (e.g., chromogranin A levels), radiological imaging, and endoscopic evaluations [1,8,26]. The frequency and duration of follow-up may vary depending on the individual patient’s risk profile, stage of disease, and treatment modality.
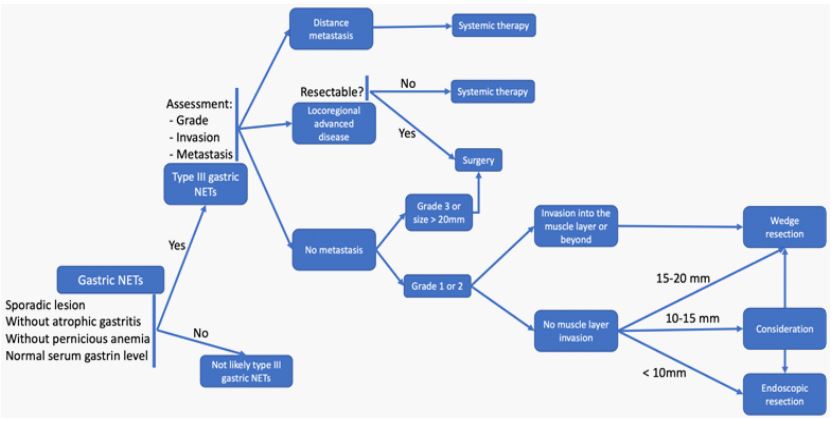
With all the above premises, the overall diagnosis and management of type III gastric NETs are summarized in Figure 3 [1,5,8,26].
Conclusion
Type III gastric NETs represent a clinically challenging entity requiring a multidisciplinary approach for optimal diagnosis and management. Continued research efforts aimed at elucidating the molecular mechanisms underlying tumor development and progression, as well as identifying novel biomarkers and therapeutic targets, are essential for advancing our understanding and improving outcomes for patients with type III gastric NETs.
Conflicts of interest: The Authors declare no conflict of interest in relation to this study.
References
- Panzuto F, Ramage J, Pritchard DM, van Velthuysen MLF, Schrader J, et al. European Neuroendocrine Tumor Society (ENETS) 2023 guidance paper for gastroduodenal Neuroendocrine Tumours (NETs) G1-G3. J Neuroendocrinol. 2023; 35(8): e13306.
- McMullen T, Al-Jahdali A, Gara C de, Ghosh S, McEwan A, et al. A population-based study of outcomes in patients with gastrointestinal neuroendocrine tumours. Can J Surg. 2017; 60(3): 192-7.
- Scherübl H, Cadiot G, Jensen R, Rösch T, Stölzel U, et al. Neuroendocrine tumors of the stomach (gastric carcinoids) are on the rise: small tumors, small problems? Endoscopy. 2010; 42(08): 664-71.
- Dasari A, Shen C, Halperin D, Zhao B, Zhou S, et al. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017; 3(10): 1335-42.
- Rindi G, Mete O, Uccella S, Basturk O, La Rosa S, et al. Overview of the 2022 WHO Classification of Neuroendocrine Neoplasms. Endocr Pathol. 2022; 33(1): 115-54.
- Rindi G, Luinetti O, Cornaggia M, Capella C, Solcia E. Three subtypes of gastric argyrophil carcinoid and the gastric neuroendocrine carcinoma: A clinicopathologic study. Gastroenterology. 1993; 104(4): 994-1006.
- Grozinsky-Glasberg S, Alexandraki KI, Angelousi A, Chatzellis E, Sougioultzis S, Kaltsas G. Gastric Carcinoids. Endocrinol Metab Clin North Am. 2018; 47(3): 645-60.
- Kunz PL, Reidy-Lagunes D, Anthony LB, Bertino EM, Brendtro K, et al. Consensus Guidelines for the Management and Treatment of Neuroendocrine Tumors. Pancreas. 2013; 42(4): 557.
- Modlin IM, Kidd M, Malczewska A, Drozdov I, Bodei L, et al. The NETest. Endocrinol Metab Clin North Am. 2018; 47(3): 485-504.
- Lloyd KA, Moore AR, Parsons BN, O’Hara A, Boyce M, et al. Gastrin-induced miR-222 promotes gastric tumor development by suppressing p27kip1. Oncotarget. 2016; 7(29): 45462-78.
- Yamashita S, Abe H, Kunita A, Yamashita H, Seto Y, et al. Programmed cell death protein 1/programmed death ligand 1 but not HER2 is a potential therapeutic target in gastric neuroendocrine carcinoma. Histopathology. 2021; 78(3): 381-91.
- Sahnane N, Furlan D, Monti M, Romualdi C, Vanoli A, et al. Microsatellite unstable gastrointestinal neuroendocrine carcinomas: a new clinicopathologic entity. Endocr Relat Cancer. 2015; 22(1): 35-45.
- Trinh VQ, Shi C, Ma C. Gastric neuroendocrine tumours from long-term proton pump inhibitor users are indolent tumours with good prognosis. Histopathology. 2020; 77(6): 865-76.
- Laffi A, Lania AGA, Ragni A, Di Vito V, Liccardi A, et al. Gastric Neuroendocrine Tumors (g-NETs): A Systematic Review of the Management and Outcomes of Type 3 g-NETs. Cancers. 2023; 15(8): 2202.
- Chun HJ, Yang SK, Choi MG, editors. Clinical Gastrointestinal Endoscopy: A Comprehensive Atlas [Internet]. Singapore: Springer Singapore. 2018. http: //link.springer.com/10.1007/978-981-10-4995-8
- Hirabayashi K, Zamboni G, Nishi T, Tanaka A, Kajiwara H, et al. Histopathology of gastrointestinal neuroendocrine neoplasms. Front Oncol. 2013; 3: 2.
- La Rosa S, Inzani F, Vanoli A, Klersy C, Dainese L, et al. Histologic characterization and improved prognostic evaluation of 209 gastric neuroendocrine neoplasms. Hum Pathol. 2011; 42(10): 1373-84.
- Manfé AZ, Norberto L, Marchesini M, Lumachi F. Usefulness of Chromogranin A, Neuron-specific Enolase and 5-Hydroxyindolacetic Acid Measurements in Patients with Malignant Carcinoids. In Vivo. 2011; 25(6): 1027-9.
- Nikou GC, Lygidakis NJ, Toubanakis C, Pavlatos S, Tseleni-Balafouta S, et al. Current diagnosis and treatment of gastrointestinal carcinoids in a series of 101 patients: The significance of serum chromogranin-A, somatostatin receptor scintigraphy and somatostatin analogues. Hepatogastroenterology. 2005; 52(63): 731-41.
- Modlin IM, Oberg K, Taylor A, Drozdov I, Bodei L, et al. Neuroendocrine Tumor Biomarkers: Current Status and Perspectives. Neuroendocrinology. 2014; 100(4): 265-77.
- Metz DC. Diagnosis of the Zollinger-Ellison Syndrome. Clin Gastroenterol Hepatol. 2012; 10(2): 126-30.
- Poitras P, Gingras M, Rehfeld JF. The Zollinger-Ellison Syndrome: Dangers and Consequences of Interrupting Antisecretory Treatment. Clin Gastroenterol Hepatol. 2012; 10(2): 199-202.
- Kwon DH, Nakakura EK, Bergsland EK, Dai SC. Gastric neuroendocrine tumors: management and challenges. Gastrointest Cancer Targets Ther. 2017; 7: 31-7.
- Roberto GA, Rodrigues CMB, Peixoto RD, Younes RN. Gastric neuroendocrine tumor: A practical literature review. World J Gastrointest Oncol. 2020; 12(8): 850-6.
- Kulke Matthew H, Mayer Robert J. Carcinoid Tumors. N Engl J Med. 1999; 340(11): 858-68.
- Shah MH, Goldner WS, Halfdanarson TR, Bergsland E, Berlin JD, et al. NCCN Guidelines Insights: Neuroendocrine and Adrenal Tumors, Version 2.2018. J Natl Compr Canc Netw. 2018; 16(6): 693-702.
- Bergsma H, van Vliet EI, Teunissen JJM, Kam BLR, de Herder WW, et al. Peptide receptor radionuclide therapy (PRRT) for GEPNETs. Best Pract Res Clin Gastroenterol. 2012; 26(6): 867-81.
- Van Der Zwan WA, Bodei L, Mueller-Brand J, De Herder WW, Kvols LK, et al. GEP-NETs UPDATE: Radionuclide therapy in neuroendocrine tumors. Eur J Endocrinol. 2015; 172(1): R1-8.
- Yamaguchi T, Machida N, Morizane C, Kasuga A, Takahashi H, et al. Multicenter retrospective analysis of systemic chemotherapy for advanced neuroendocrine carcinoma of the digestive system. Cancer Sci. 2014; 105(9): 1176-81.
- Modlin IM, Lye KD, Kidd M. A 50-Year Analysis of 562 Gastric Carcinoids: Small Tumor or Larger Problem? Am J Gastroenterol. 2004; 99(1): 23-32.
- Hirasawa T, Yamamoto N, Sano T. Is endoscopic resection appropriate for type 3 gastric neuroendocrine tumors? Retrospective multicenter study. Dig Endosc. 2021; 33(3): 408-17.