
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Expression and correlation analysis of related molecules in peripheral blood of patients with COVID-19
Hongwei Li1 ; Li Zhao2 ; Shangzhi Wu1 ; Sixiang Tang2 ; Keshab Bahadur Kunwar2 ; Chengyu Lu1 ; Dehui Chen1*
1The First Affiliated Hospital of Guangzhou Medical University, Pediatrics, Guangzhou 510120, China.
2Guangzhou Medical University, Guangzhou 510120, China.
*Corresponding Author : Dehui Chen
The First Affiliated Hospital of Guangzhou Medical University, Pediatrics, Guangzhou 510120, China.
Tel: 18928868216;
Email: dehuichen2022@163.com
Received : May 01, 2024
Accepted : May 22, 2024
Published : May 29, 2024
Archived : www.jjgastro.com
Copyright : © Chen D (2024).
Abstract
Objective: To investigate the expression of neuropeptide family members in the peripheral blood of children infected with COVID-19 and its correlation with inflammatory indicators.
Methods: Blood samples were collected from 40 newly diagnosed children with COVID-19 infection and 17 hospitalized children with non-COVID-19 bronchial pneumonia in our hospital during the same period. Baseline clinical data were collected and analyzed. Expression and correlation analysis of neuropeptide-related molecules in peripheral blood were detected and analyzed by ELISA.
Results: In this study, 43% of COVID-19 patients are male. 71% of non-COVID-19 patients are male. ACE and ACE2 in the COVID-19 group were not significantly higher than that in the non-COVID-19 group, and ACE2 in non-COVID-19 and moderate COVID-19 groups was higher than that in severe groups (p=0.04*; p=0.03*). ASCL1 in the non-COVID-19 group was higher than that in the COVID-19 group (p=0.04*). ASCL1 in the non-COVID group was higher than that in the severe COVID group (P=0.02*). There were no significant differences in SP, VIP, and GRP between COVID-19 and non-COVID-19 groups. ASCL1 respectively with N % (r=-0.534, p< 0.001***), CRP (r =- 0.522, p < 0.001***) negatively correlated, L % (r=0.572, p<0.001***), AST (r=0.496, p=0.001**) were positively correlated. There was no significant correlation with WBC count, PLT count, ALT, LDH.
Conclusion: We found that, unlike adults, ACE and ACE2 were not high in children with COVID-19. ASCL1 in children with COVID-19 is lower than that in non-COVID-19 children, which may indicate that ASCL1 may be decreased in COVID-19 patients. At the same time, ASCL1 is negatively correlated with N% and CRP, suggesting that ASCL1 may play a certain role in COVID-19 inflammation.
Keywords: COVID-19; Neuropeptides; Inflammation.
Citation: Li H, Zhao L, Wu S, Tang S, Chen D, et al. Expression and correlation analysis of related molecules in peripheral blood of patients with COVID-19. J Gastroenterol Res Pract. 2024; 4(6): 1203.
Introduction
Omicron is a variant of the novel coronavirus. Compared with other strains, Omicron is highly transmissible and highly occult. After infection, it mainly presents systemic symptoms such as fever and is mostly accompanied by local symptoms such as respiratory symptoms such as cough, digestive symptoms such as vomiting, and nervous system symptoms such as dizziness [1,2]. Up to 30% of COVID-19 infections in adults have neurological symptoms, such as memory loss, confusion, severe headaches, and even stroke, which can persist even after the infection has ended, while children who are infected have a lower incidence of neurological symptoms, but are more likely to experience coughing, wheezing, and wheezing. In addition to the inflammation of the lung interstitial after COVID-19 infection, it may also be related to the regulation of the expression of neuropeptides in lung epithelial cells [2-4]. There are abundant neuropeptide systems in the human body, such as the neurokinin family (Substance P, SP) and the bombine peptide family: Bell toad peptide, Gastrin-Releasing Peptide (GRP), neurokinin B, vasoactive intestinal peptide, ACE/ACE2, such as Vasoactive Intestinal Peptide (VIP), neuroblast-specific transfer factor (Achaete Scute Homolog 1 (ASCL1), and angiotensinase. ACE2 has been shown to be the key for the new coronavirus to enter the human body. In 2022, Professor Rick Thompson of Queensland University of Technology said that the new coronavirus needs to bind to the receptor ACE2 on the surface of human cells to enter and infect human cell C, and their research found that even if it is only briefly exposed to atmospheric pressure cold plasma. The ACE2 receptor on the cell surface will also disappear immediately, which reduces the way for the novel coronavirus to infect human cells through the receptor and achieve the effect of preventing infection [5,6]. The expression of other neuropeptide family members in children with COVID-19 infection and their correlation with inflammatory indicators will be further discussed below.
Material and methods
The EDTA tube collected peripheral blood samples from 40 newly diagnosed children with COVID-19 infection in the Department of Pediatrics of the First Affiliated Hospital of Guangzhou Medical University from December 2022 to February 2023 (diagnosed by the diagnosis and treatment protocol for novel coronavirus infection (10th edition)) and 17 hospitalized children with non-COVID-19 bronchial pneumonia in the department of Pediatrics of our hospital during the same period. Baseline clinical data were collected and analyzed, including the basic information, clinical symptoms, and laboratory tests of the case group and the disease control group. The expression of angiotensin molecules (ACE, ACE2) and neuropeptide-related molecules (SP, VIP, GRP, ASCL1) in the serum of the two groups were detected by ELISA, and the correlation with white blood cell count, lactate dehydrogenase, and other substances was analyzed (approval number: 20230570).
Statistical analysis
After data collection and coding, statistical analysis was performed using GraphPad Prism 9 (The authors confirm that they had obtained copyright licenses). Descriptive analysis was performed on all variables for which the data were frequency and percentage distributions, including demographic data and clinical characteristics. The mean and Standard Deviation (SD) for the measurement data was calculated. When comparing the mean of the samples of the two groups in the measurement data, the Unpaired t-test was used for the comparison of groups with normal distribution, and the Mann-Whitney test was used for the comparison of groups with no normal distribution. When comparing the mean of the three groups of samples in the measurement data, a pair-to-pair comparison was conducted among the three groups. A parametric test (ANOVA test) was used for comparison between groups that all obeyed normal distribution, and a non-parametric test (Kruskal-Wallis test) was used for comparison between groups that did not obey normal distribution. When analyzing the correlation of laboratory indicators, the Pearson correlation coefficient is used to calculate the bivariate correlation if both variables obey the normal distribution, and the Spearman correlation coefficient is used to calculate the bivariate correlation if some variables do not obey the normal distribution. The difference was statistically significant with P<0.05.
Results
A total of 40 children with COVID-19 infection were collected in this study, accounting for 43% of males, and 17 children without COVID-19 infection, accounting for 71% of males (P=0.391). The average age of patients with and without COVID-19 infection was (3±3) vs. (7±6) years, respectively (P=0.039*). In the collected cases, the length of stay of patients with and without COVID-19 infection was (6±3) vs (7±4) years, respectively (P=0.515). There were no statistical differences in clinical symptoms such as fever (31[78%] vs. 10[59%], P=0.201), nasal congestion (18[45%] vs. 6[35%], P=0.568), runny nose (21[53%] vs. 12[71%], P=0.251), cough (36[90%] vs. 16[94%], P>0.999), expectoration (31[78%] vs. 15[88%], P=0.476), wheeze (6[15%] vs. 5[29%], P=0.275) and diarrhea (1[3%] vs. 1[6%], P=0.511) between COVID children and non-COVID children. There were no significant differences in CK-MB (22.50±10.05 vs. 17.59±5.42, P=0.091), CK (150.81±193.20 vs. 180.50±180.07, P=0.281), neutrophil ratio (40.36±19.64 vs. 43.85±16.36, P=0.481), lymphocyte ratio (48.28±19.26 vs. 43.04±15.02, P=0.322), WBC (10.35±5.74 vs. 10.60±5.60, P=0.813) and CRP (1.19±2.18 vs. 0.74±1.73, P=0.232) between COVID children and non-COVID children. The expressions of ALT (33.74±54.19 vs. 15.44±5.41, P=0.005**), AST (53.67±40.95 vs. 31.96±10.40, P=0.004*), and LDH (379.62±145.04 vs. 289.93±85.97, P=0.013*) in the COVID-19 group were higher than those in the non-COVID-19 group, eosinophilic granulocyte ratio (EOS%) (1.21±1.46 vs. 2.06±2.00, P=0.028*) was lower than those in the non-COVID-19 group (Table 1).
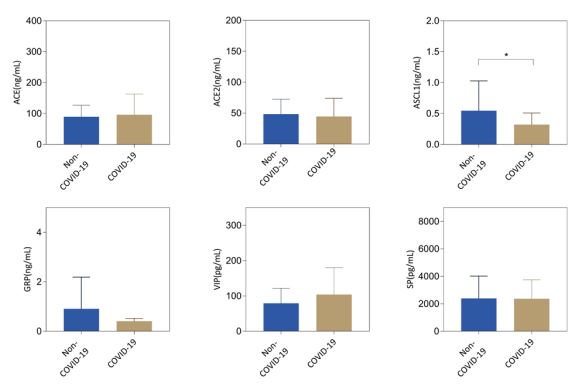
The expression of angiotensin molecules (ACE, ACE2) and neuropeptide-related molecules (SP, VIP, GRP, ASCL1) in peripheral blood of COVID-19 and non-COVID-19 infected groups were detected by ELISA. The results showed that the expression of ACE and ACE2 in the peripheral blood of children in the COVID-19 group was not significantly higher than that in the non-COVID-19 group (P=0.749; P=0.319, respectively), and the level of ACE2 in severe COVID-19 patients was lower than that in non-COVID-19 patients and moderate COVID-19 patients (P=0.036*; P=0.029*, respectively). The level of ASCL1 in COVID-19 patients was lower than that in non-COVID-19 patients (p=0.039*), and the level of ASCL1 in severe COVID-19 patients was lower than that in non-COVID-19 patients (p=0.021*). There were no significant changes in VIP, SP and GRP expression in COVID-19 and non-COVID-19 groups (P=0.373, P=0.401, P=0.464, respectively) (Figure 1).
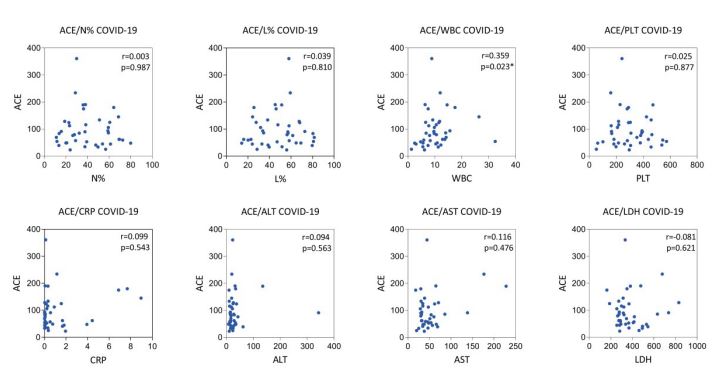
ACE was positively correlated with WBC (r=0.359, P=0.023*), but was not significantly correlated with N% (r=0.003, P=0.987), L% (r=0.039, P=0.810), PLT (r=0.025, P=0.877), CRP (r=0.099, P=0.543), ALT (r=0.094, P=0.563), AST (r=0.116, P=0.476), LDH (r=-0.081, P=0.621) (Figure 2).
ACE2 was positively correlated with PLT (r=0.345, P=0.029*) and negatively correlated with N% (r=-0.314, P=0.049*), but was not significantly correlated with L% (r=0.311, P=0.051), WBC (r=0.278, P=0.083), CRP (r=-0.139, P=0.394), ALT (r=0.102, P=0.532), AST (r=0.089, P=0.584), LDH (r=-0.037, P=0.821) (Figure 3).
ASCL1 respectively with N% (r=-0.534, p<0.001***), CRP (r=-0.522, p<0.001***) negatively correlated, L% (r=0.572, P<0.001***) and AST (r=0.496, p=0.001 * *) were positively correlated. There was no significant correlation with WBC, PLT, ALT, LDH (r=-0.092, P=0.573; r=0.059, P=0.720; r=0.291, P=0.069; r=0.216, P=0.182, respectively) (Figure 4).
GRP and VIP were not significantly correlated with N% (r=0.169, P=0.297; r=-0.087, P=0.595, respectively), L% (r=- 0.147, P=0.364; r=0.093, P=0.567, respectively), WBC (r=0.067, P=0.682; r=-0.130, P=0.424, respectively), PLT (r=-0.074, P=0.649; r=-0.173, P=0.286, respectively), CRP (r=0.221, P=0.172; r=0.133, P=0.412, respectively), ALT (r=0.197, P=0.223; r=-0.085, P=0.604, respectively), AST (r=-0.140, P=0.391; r=0.120, P=0.461, respectively), and LDH (r=0.026, P=0.875; r=0.048, P=0.768, respectively) (Figures 5,6).
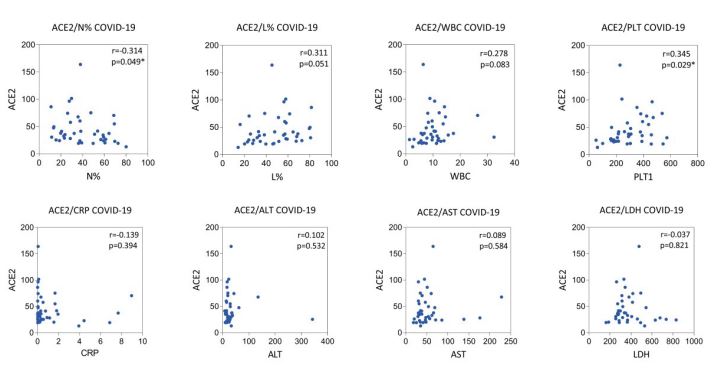

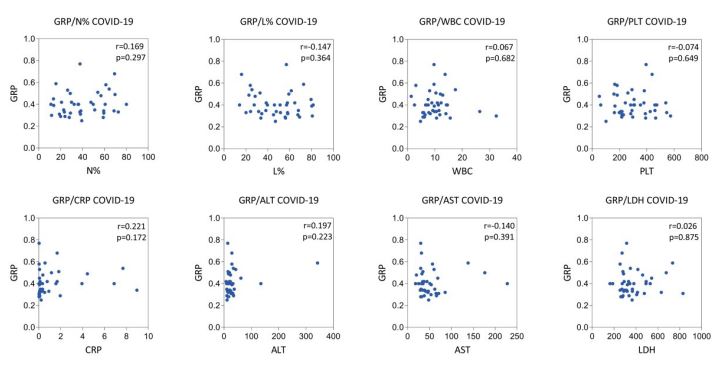
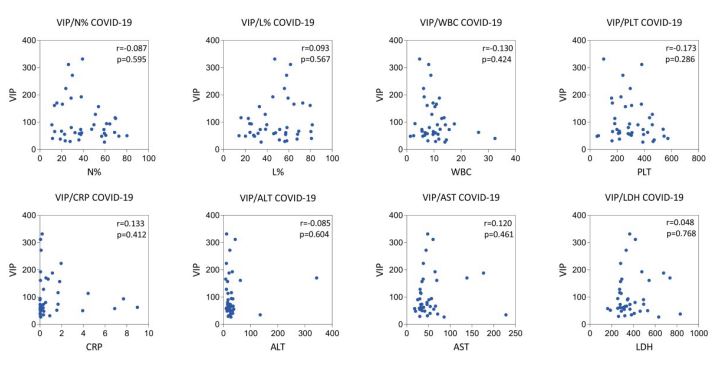

Table 1: Baseline data between COVID-19 and non-COVID-19 group.
| COVID-19 (n=40) | Non-COVID-19 (n=17) | P value | |
|---|---|---|---|
| Age (year), s±x | 3±3 | 7±6 | 0.039* |
| Male, n(%) | 17 (43) | 12 (71) | 0.391 |
| In-hospital (day), s±x | 6±3 | 7±4 | 0.515 |
| Fever, n(%) | 31 (78) | 10 (59) | 0.201 |
| Nasal obstruction, n(%) | 18 (45) | 6 (35) | 0.568 |
| Running nose, n(%) | 21 (53) | 12 (71) | 0.251 |
| Cough, n(%) | 36 (90) | 16 (94) | >0.999 |
| expectoration, n(%) | 31 (78) | 15 (88) | 0.476 |
| Wheeze, n(%) | 6 (15) | 5 (29) | 0.275 |
| Diarrhea, n(%) | 1 (3) | 1 (6) | 0.511 |
| CK-MB(U/L), s±x | 22.50±10.05 | 17.59±5.42 | 0.091 |
| CK (U/L), s±x | 150.81±193.20 | 180.50±180.07 | 0.281 |
| Neutrophil ratio (N%), s±x | 40.36±19.64 | 43.85±16.36 | 0.481 |
| Lymphocyte ratio (L%), s±x | 48.28±19.26 | 43.04±15.02 | 0.322 |
| Eosinophilic ratio (EOS%), s±x | 1.21±1.46 | 2.06±2.00 | 0.028* |
| WBC (×109/L), s±x | 10.35±5.74 | 10.60±5.60 | 0.813 |
| PLT (×109/L), s±x | 300.95±132.40 | 405.76±156.51 | 0.012* |
| CRP (mg/dl), s±x | 1.19±2.18 | 0.74±1.73 | 0.232 |
| ALT (U/L), s±x | 33.74±54.19 | 15.44±5.41 | 0.005** |
| AST (U/L), s±x | 53.67±40.95 | 31.96±10.40 | 0.004** |
| LDH (U/L), s±x | 379.62±145.04 | 289.93±85.97 | 0.013* |
SP was positively correlated with L% (r=0.329, P=0.038*), but was not significantly correlated with N% (r=-0.310, P=0.051), WBC (r=0.028, P=0.866), PLT (r=-0.046, P=0.780), CRP (r=-0.188, P=0.246), ALT (r=0.080, P=0.625), AST (r=-0.007, P=0.967), LDH (r=0.068, P=0.677) (Figure 7).
Discussion & conclusion
Neuropeptides are a kind of special information substances, which generally refer to the endogenous active substances that exist in nervous tissues and participate in the function of the nervous system. It is characterized by low content, high activity, extensive and complex effects, and regulates a variety of physiological functions in the body, such as pain, sleep, emotions, learning and memory, and even the differentiation and development of the nervous system itself are regulated by neuropeptides. Neuropeptides not only exist in the nervous system, but also widely exist in various systems throughout the body, playing various roles such as neurohormones, neurotransmitters, neuromodulators, and cytokines, and playing important regulatory roles in various physiological functions at various stages of biological development [7]. In recent years, with the development of molecular biology technology, the research of neuropeptides is making rapid progress with each passing day.
The novel coronavirus may invade sensory neurons and glial cells of the vagus nerve, inducing the release of neuropeptides and inflammatory mediators. Epithelial cells and inflammatory cells (such as macrophages, neutrophils, lymphocytes, etc.) involved in COVID-19 infection and recognition can release a variety of cytokines and inflammatory mediators [8]. Neuropeptides and neuroinflammatory mediators can further recruit and activate immune cells, cause lung and airway inflammation, and enhance cough sensitivity. The nerve-phagocytic nature of the novel coronavirus leads to the release of various inflammatory mediators such as histamine, triggering neurogenic inflammation, and directly or indirectly stimulating nerve receptors, resulting in increased cough sensitivity [9]. COVID-19 infection can induce eosinophilic bronchitis or airway hyperresponsiveness, a subacute stage of eosinophilic bronchial inflammation, or cough-variant asthma. At present, a large number of studies have found that local glucocorticoids can reduce bronchial inflammation caused by COVID-19 infection or the subacute stage of variant asthma, mainly through a wide range of effects on structural cells and inflammatory cells, and multi-target blocking airway inflammation. It also reduces neuroreceptor sensitivity by reducing neurogenic inflammation. This suggests that the abnormal release of neuropeptides plays a major role in the pathogenesis of COVID-19 [10,11].
ACE2 is distributed in almost all immune cells and endothelial cells, and its loss in these two cells will lead to the weakening and failure of many important organs in the body [12]. COVID-19 has a high affinity with ACE2 receptors, and ACE2 is highly expressed in some COVID-19 infections with chronic underlying diseases and elderly people, suggesting that more ACE2 is needed to counteract the adverse effects of angiotensin II [13,14]. The number of ACE2 receptors is related to age and body health. Studies have shown that the expression of ACE2 in children’s nasal epithelial cells is low. In this study, the expression of ACE and ACE2 in children’s COVID-19 group was not high. There was no significant correlation with the expression of LDH/N%/L%/CRP, an inflammatory indicator of the disease, similar to foreign studies, which may be one of the reasons why children are more tolerant to COVID-19 and have a lower incidence of severe diseases.
ASCL1, a key transcription factor in the development of autonomic ganglia that is overexpressed in fibroblasts, has not been detected in COVID-19-infected patients. Studies have shown that specifically knocking out the ASCL1 gene in asthmatic mice can restrict nerve conduction in lung tissue. At the same time, the levels of inflammatory cells such as Th2, eosinophil, and ILC2 cells were significantly lower than those of wild-type mice, and the expressions of IL-5 and IL-13 were also significantly lower than those of the control group. It is suggested that ASCL1 plays an important role in airway neuroendocrine regulation. In particular, it plays an important role in the occurrence of human wheezing. In this study, the expression level of ASCL1 was negatively correlated with N% and CRP, suggesting that ASCL1 may play a certain role in the inflammation of COVID-19. Further studies on the mechanism of action and larger samples will be discussed in the future.
Gastrin-Releasing Peptide (GRP) is a neuropeptide widely available in the central nervous system. It has a high affinity with GRP Receptor (GRPR) and its expression in different brain regions can participate in different functions. Such as itch, sighing, fear memory, and so on. Recent studies have shown that GRP is significantly elevated in children with asthma, and the use of GRP blockers and GRP antibodies can prevent the abnormal increase of airway reactivity in asthmatic mouse models stimulated by OVA, reduce the number of macrophages and granulocytes in bronchoalveolar lavage fluid, and reduce the levels of IL-5, IL-13, and other cytokines. In this study, there was no statistically significant difference in GRP/VIP expression between COVID-19 infection and non-COVID-19 infection. These results suggest that GRP/VIP has different roles in asthma and COVID-19 infection, so its expression level may be conducive to distinguishing acute asthma attacks or asthma combined with COVID-19 infection.
VIP is distributed in the nerve endings of the bronchial smooth muscle near the human lung and around the submucosal glands of the lung and bronchus. The enzymes released by inflammatory cells in children with asthma will degrade and destroy VIP, which is conducive to cholinergic nerve action and leads to bronchospasm. Therefore, VIP mainly acts as an inhibitory neurotransmitter in the body.
SP is the most abundant sensory neuropeptide in the lung. When SP is released from the sensory nerve by the axonal reflex after inhalation of stimuli, it can induce bronchoconstriction by binding to the specific opposite receptors in the lung, resulting in wheezing. At the same time, SP is involved in the occurrence of lung immune regulation and inflammatory response, and SP has a chemotactic effect on T cells, mononuclear macrophages, and eosinophils [15,16]. SP level in the sputum of asthmatic patients and chronic bronchitis patients is significantly higher than that of the control group, and SP level in asthmatic patients induced sputum is positively correlated with eosinophils level [17]. SP has not been studied in children with COVID-19 infection. Cough and wheezing are usually one of the main symptoms in children infected with COVID-19. The specific mechanism of cough and wheezing remains unclear. Non-specific inflammation of the lung interstitial is the main pathophysiological change.
In this study, the expression of neuropeptide-related molecules in COVID-19-infected patients and their correlation with inflammatory indicators were preliminarily analyzed. It was found that, unlike adults, ACE and ACE2 expression was not high in children with COVID-19. The level of neuropeptide ASCL1 in children with COVID-19 was lower than that in non-COVID-19 children, which may indicate that the expression level of ASCL1 may be decreased in COVID-19 patients. At the same time, the expression level of ASCL1 is negatively correlated with N% and CRP, suggesting that ASCL1 may play a certain role in COVID-19 inflammation. Limited by the size of the sample size, this project failed to conduct large-sample and multi-center clinical studies. However, we have provided a new research entry point for COVID-19 infection, focusing on the level of neuropeptides. We will further explore the role of neuropeptides in lung diseases caused by COVID-19 infection through in vivo and in vitro experiments to provide accurate treatment for COVID-19 Therapy provides a new theoretical basis.
Declarations
Acknowledgments: Not applicable.
Funding: This work was supported by the Basic and Applied Basic Research Foundation of Guangdong Medical Research Foundation (grant number A2023345), Zhong Nanshan Medical Foundation of Guangdong Province (grant number202102010343) and the Science and Technology Program of Guangzhou (grant number 202102010276).
Availability of data and material: The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Patient consent for publication: The study scheme was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University. All volunteers participating in the experiment signed the informed consent.
Authors’ contributions: DHC and HWL were involved in the design and supervision of the experiment. LZ, SXT and KBK conducted several experiments and experimental data collection. CYL and SZW collect and classify clinical data. HWL analyzed all data and completed the initial writing of the manuscript. LZ completed the revision and submission of the manuscript.
Ethics approval and consent to participate: This article had received ethical approval and data could be obtained in supplementary materials.
Competing interests: The authors declare that they have no competing interests.
References
- Farman M, et al. Fractal-fractional operator for COVID-19 (Omicron) variant outbreak with analysis and modeling. RESULTS PHYS. 2022; 39: 105630.
- Franch-Llasat D, et al. Pneumococcal meningitis secondary to otitis media in two patients with COVID-19 omicron variant. INT J EMERG MED. 2022; 15: 50.
- Galloway S, Taunton C, Matysek R, Hempenstall A. Seeking to improve access to COVID-19 therapeutics in the remote Torres and Cape communities of Far North Queensland during the first COVID-19 omicron outbreak. RURAL REMOTE HEALTH. 2022; 22: 7657.
- Jing Y, et al. Potential influence of COVID-19/ACE2 on the female reproductive system. MOL HUM REPROD. 2020; 26: 367-373.
- South AM, Diz DI, Chappell MC. COVID-19, ACE2, and the cardiovascular consequences. AM J PHYSIOL-HEART C. 2020; 318: H1084-H1090.
- Sui P, et al. Pulmonary neuroendocrine cells amplify allergic asthma responses. SCIENCE. 2018; 360.
- Carvelli J, et al. Association of COVID-19 inflammation with activation of the C5a-C5aR1 axis. NATURE. 2020; 588: 146-150.
- Lamb LE, et al. COVID-19 inflammation results in urine cytokine elevation and causes COVID-19 associated cystitis (CAC). MED HYPOTHESES. 2020; 145: 110375.
- Fernandez-Cruz A, et al. A Retrospective Controlled Cohort Study of the Impact of Glucocorticoid Treatment in SARS-CoV-2 Infection Mortality. ANTIMICROB AGENTS CH. 2020; 64.
- Jiao X, et al. A real-world study of glucocorticoid treatment in COVID-19 patients with different disease severities. CLIN TRANSL MED. 2020; 10: e235.
- Thye AY, et al. Psychological Symptoms in COVID-19 Patients: Insights into Pathophysiology and Risk Factors of Long COVID-19. BIOLOGY-BASEL. 2022; 11.
- Martinez-Gomez LE, et al. ACE and ACE2 Gene Variants Are Associated With Severe Outcomes of COVID-19 in Men. FRONT IMMUNOL. 2022; 13: 812940.
- Khan WH, et al. COVID-19 Pandemic and Vaccines Update on Challenges and Resolutions. FRONT CELL INFECT MI. 2021; 11: 690621.
- Huang B, et al. Substance P protects against hyperoxic-induced lung injury in neonatal rats. EXP LUNG RES. 2015; 41: 12-20.
- Wang N, et al. Substance P-induced lung inflammation in mice is mast cell dependent. CLIN EXP ALLERGY. 2022; 52: 46-58.
- Lieb K, et al. Effects of the neuropeptide substance P on sleep, mood, and neuroendocrine measures in healthy young men. NEUROPSYCHOPHARMACOL. 2002; 27: 1041-1049.
- Piedimonte G. Neural mechanisms of respiratory syncytial virusinduced inflammation and prevention of respiratory syncytial virus sequelae. AM J RESP CRIT CARE. 2001; 163: S18-S21.