
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 4
The management of peptic ulcer disease using conventional methods, bioactive compounds and dietotherapy: A review
Mumukom Maximus Anchang*; Francis Chigozie Okoyeuzu; Jane Ngozi Okafor; Gabriel Ifeanyi Okafor
Department of Food Science and Technology, University of Nigeria Nsukka, Nigeria.
*Corresponding Author : Anchang M Maximus
Department of Food Science and Technology, University of
Nigeria Nsukka, Nigeria.
Tel: +234-8108240311;
Email: anchangmaximus@daad-alumni.de
Received : Apr 18, 2024
Accepted : May 15, 2024
Published : May 22, 2024
Archived : www.jjgastro.com
Copyright : © Anchang MM (2024).
Abstract
Purpose of review: The management of Peptic Ulcer Disease (PUD) is achieved using pharmacological agents to counteract the aggressive factors or stimulate the mucosal defence. In recent years, plant-based bioactive products have gained popularity as an alternative management protocol due to the increased antibiotic resistance of Helicobacter pylori (H. pylori), lower cost, perceived effectiveness, availability, and little side effects. In this review, we summarized the conventional treatment methods, alternative bioactive compounds, and the dietotherapy of PUD.
Recent findings: The conventional management methods include antacids, gastric muscle stimulants, mucosal-increasing resistance agents, antisecretory medications (anticholinergic agents), and Proton Pump Inhibitors (PPIs). Most of the plant’s bioactive compounds are alkaloids, terpenes, flavones, isoflavones, flavonols, chalcones, flavanones, xanthones, flavan-3-ols, anthocyanins, and capsaicinoids. These bioactive compounds work in a dose-dependent manner and express their therapeutic functions through pro-inflammatory cytokines such as Tumor Necrosis Factor-alpha (TNF-α), Interleukin-1 beta (IL-1β), and Interleukin-6 (IL-6), resulting in a reduction in prostaglandin E2. No food product has a history of causing the PUD, but some foods are prohibited or need to be taken with caution. Some of these food items, such as spicy foods, caffeine, and alcohol, can hinder healing and worsen the symptoms while fibres, vitamins C and A, zinc, iron, and selenium can promote healing.
Conclusion: While there are limited articles in the literature to elucidate the dietotherapy of PUD, a balanced diet should always be provided in this course to manage the pathology. The paucity of this information opens up more research opportunities in PUD dietotherapy.
Keywords: Helicobacter Pylori; Gastric defence factors; Aggressive factors; Antibiotic resistance; Pro-inflammatory cytokines; Balanced diet.
Citation: Anchang MM, Okoyeuzu FC, Okafor JN, and Okafor GI. The management of peptic ulcer disease using conventional methods, bioactive compounds and dietotherapy: A review. J Gastroenterol Res Pract. 2024; 4(5): 1202.
Introduction
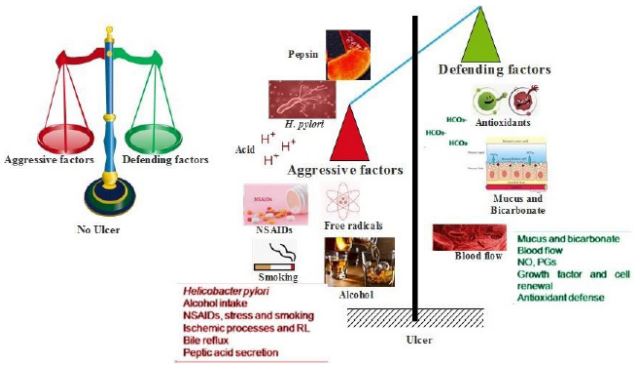
Peptic ulcer is a sore in the gastrointestinal lining resulting in the breakdown of the mucosal and submucosal layers [1]. Peptic ulcers come about due to the peptic acid injury of the gut, leading to the breakdown of the digestive system’s mucosal layer, with injury greater than 3-5 mm [1]. This injury can occur along the oesophagus (oesophageal ulcer), stomach walls (gastric ulcer), and the duodenum (duodenal ulcer). It occurs due to rupturing of the mucosal layer’s protective barrier for these three digestive system components. Individual susceptibility to Non-Steroidal Anti-inflammatory Drugs (NSAID) toxicity and H. pylori virulence determines the degree of damage to the mucosa layer. The mucosa layer has the unique ability to resist injury resulting from high peptic acid concentration, influx of bile, and pepsin [2]. The breakdown of this layer is due to the imbalance between the protective and aggressive factors of the mucosal layer [3].
The protective factors include bicarbonate (HCO3 - ), the mucus barrier consist of 95% water and 0.2-5.0% mucins, ions, lipids, cell debris, DNA, and salts, the endogenous antioxidant system’s synthesis of cytoprotective Prostaglandins (PGs), Nitric Oxide (NO), and adequate blood flow [2,3]. Other protective factors include the hydrophobic mucosal surface epithelium, which can repel acids and other water-soluble agents. Aggressive factors that compromise the integrity of the mucosal layer include Helicobacter pylori, which is the leading causative agent [4], and Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), which are the second-most causative agents [1]. H. pylori accounts for about 70% of the cases, while NSAIDs account for about 10% [5]. Other aggressive factors include Hydrochloric Acid (HCl), pepsin activity, bile reflux, and decreased blood flow. Also, some exogenous actors include inappropriate eating habits, stress [6], and chemical agents such as alcohol, smoking, hygienic conditions, level of education, low socioeconomic status, poor water supplies, and financial status [7,8]. The etiopathogenesis of peptic ulcer disease is presented in Figure 1.
The mode of invasion by H. pylori starts when the bacterium creates an environment required for its survival in the stomach beneath the mucosal barrier by producing urease. Additionally, the bacterium expresses adhesins like the blood group antigen adhesin (BabA) and the Outer inflammatory protein Adhesin (OipA) that aid the bacterium in adhering to the gastric epithelium. The virulent factors CagA and PicB, encoded by a pathogenic genome island, and other bacterial factors, interact aggressively with host tissue and be associated with gastric mucosal inflammatory cell and activate stomach epithelial injury [9]. Again, NSAID can increase complications of peptic ulcers by four folds and aspirin can increase the risk by two folds [10]. This is through the inhibitory effect of prostanoid biosynthesis caused by NSAID and aspirin. Prostanoids (prostaglandins, thromboxanes, prostacyclins) are derivatives of arachidonic acid obtained with the help of Cyclo-Oxygenase (COX) isoenzymes after cell lesions [11]. NSAID exert the inhibitory effect by limiting the action of COX 2 enzymes that are needed in the synthesis of prostanoids. Risk factors that have been associated with the acquisition and prevalence of H. pylori infection in West and Central Africa include poor sanitary practices, family income, educational level, age, occupation, some religious practices, and poor water supplies [12].
Although, its complications have remained constant, about 5-10% of the general population worldwide is infected with PUD, with about four million people infected annually [13,14]. In western countries, the prevalence is 0.1-0.3% [1]. Introducing new therapies for treating this disease in developed countries has reduced its frequency of occurrence. In sub-Saharan Africa, the prevalence is high, at 24.5% in dyspeptic patients compared to 12-25% for symptomatic patients [15]. In 2019, the prevalence amounted to 8.09 million people worldwide, with a further tendency to increase [5]. Comparing the prevalence of PUD in different parts of Africa, studies have revealed that the prevalence in Northern Savana is lower than in Central and Western parts of Africa [15]. Studies have shown that the incidences in Sub-Saharan African countries are higher in women than in men, with the mortality rate in males being higher than in females except in Central Sub-Saharan Africa [5]. In Ghana and Nigeria, the incidence in females is about 54-57% [15]. In some 264 children, aged 2-11 years who were administered in Cottage Hospital Inyi, Nigeria, 16% of those children were diagnosed with PUD, with 8.3% cases in females and 7.6% of the cases in males [16]. In the Northern part of Nigeria (Kanu State) a study conducted at a teaching hospital showed that in a sample size of 70 patients, 64.3% were males while 35.7% were females, with the highest number of cases found in patients aged between 31-50 years [17]. Generally, for patients with gastric ulcers (stomach), the symptoms are postprandial abdominal pain, vomiting, nausea, and weight loss. For patients with duodenal ulcers, the symptoms include abdominal pain at night and the feeling of being hungry [18]. Other complications include bloating, fullness, heartburn, bleeding, perforation and gastric outlet obstruction, with fatality rate between 5-10% [19].
Management of PUD
The use of conventional drugs for the management of PUD
Healing peptic ulcers and avoiding potential relapses are possible with H. pylori eradication alone, however, due to H. pylori’s growing antibiotic resistance to standard medications, this endeavour is challenging. Since PUD is caused by an imbalance in the defensive and aggressive factors, its treatment can focus on stemming the aggressive factors or strengthening the defensive mechanism. Proton Pump Inhibitors (PPI), clarithromycin, bismuth salt, tetracycline, amoxicillin, metronidazole, and other medications are frequently used to treat PUD [20]. If the use of the NSAIDs is stopped, PPIs can treat more than 85% of PUD cases caused by NSAIDs or aspirin in 6 to 8 weeks. A combination of COX-2-selective NSAIDs and PPI is the most effective defence against PUD caused by NSAIDs [21]. Antiulcer medications’ sites of action or modes of action can be used to categorize them. Examples include antacids, gastric muscle stimulants, mucosalincreasing resistance agents, antisecretory medications (anticholinergic agents), corticohypothalamic drugs, and Proton Pump Inhibitors (PPIs). Table 1 summarizes the conventional drugs used in treating PUD and the groups to which each drug belongs.
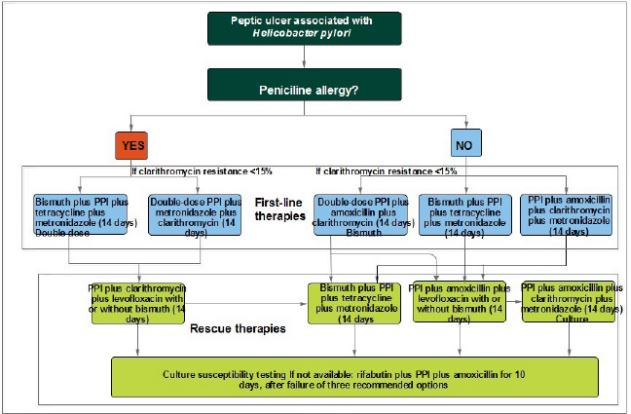
Figure 2 displays the algorithm for treatment of peptic ulcers caused by Helicobacter pylori. Proton pump inhibitors and two antibiotics, namely clarithromycin and either amoxicillin or metronidazole, are used in the treatment for 7-14 days. This therapy is called the proton pump inhibitor-based triple therapy [1,20].
The use of plant bioactive compounds
Plant-based products have gained popularity as an alternative treatment over commercially available synthetic drugs in the management of PUD due to increased antibiotic resistance of H. pylori, lower cost, perceived effectiveness, and availability, and because of little or no adverse side effects [22]. Examples of some of the major bioactive compounds with a track record of use in the management of peptic ulcer disease are presented in Table 2.
Dietotherapy of PUD
The long history of a balanced diet having the potential to treat and eradicate chronic diseases and enhance health is no longer news. To this effect, dietotherapy has played a significant role in the management of peptic ulcers, with the potential to protect the gastrointestinal lining, reduce pain, improve digestion, and improve nutritional status [23]. Dietotherapy for peptic ulcers always aims to prevent acid hypersecretion and subsequent pain reduction in the gastric and duodenal mucosa, as a decrease in this acid secretion promotes overall healing [24]. There may be no ideal diet that can express this effect on all individuals, as people have different nutritional needs. Hence, understanding the dietary deficiencies of people suffering from peptic ulcers can be crucial in formulating recovery diets. However, as a rule of thumb, functional food for the management of peptic ulcer should contain; energy (25-30 Kcal/Kg), proteins (12-15% or 1.2-1.5 g/Kg/weight), carbohydrates (50-60%), lipids (25-30 g/day), fibre (20-30 g/day), zinc (40 mg), selenium (400 µg), vitamin A (3000 µg/day), vitamin C (500 mg), vitamin B12 (2.4 µg), folic acid (400 µg), iron (45 mg), and probiotics containing 109 to 1011 cfu/day lactic acid bacteria [24].
Particularly helpful in the management of peptic ulcers is fibre. The different physicochemical properties of fibres make them have a broader effect on organisms, demonstrating different effects on the gastrointestinal tract. Fibres regulate bowel function and, thus, are crucial in maintaining health and managing many GI tract-related pathologies. The health claims are remarkably higher for soluble fibres that add bulk to the stool and reduce food transit time through the gut. According to HealthLinkBC [25], a diet high in fibres, especially soluble fibres from vegetables, fruits, beans, oatmeal, and peas, can manage peptic ulcers. The World Health Organization recommends 20 to 30 g of fibre daily to manage the disease. The fibres act as buffers, lowering bile concentration, and abdominal bloating, and reducing pain and discomfort in the gastrointestinal tract [23,24,26].
Vitamin A can increase mucus production in the gastrointestinal tract, so a diet rich in vitamin A can be beneficial in treating peptic ulcer disease [27]. A 100 mg/kg dose of carotenoid extract has shown the ability to reduce NO production, IL-6, and prostaglandin E2 in gastric ulcer rats induced with HCl and ethanol [28]. In addition to Vitamin A, Vitamins E, C, and B12, selenium, and iron have also shown prospects for managing the disease. In a study by Yousaf et al. [29] in ulcer rats experimentally induced with indomethacin, 400 mg/kg body weight of Vitamin E increased mucus production in the gastric glands compared to the groups that were not treated with Vitamin E, indicating the efficacy of Vitamin E in PUD management. In another study by Sezikli et al. [30], 500 mg/kg body weight and 200 mg/kg body weight of vitamins E and C were administered to patients with H. pylori for four weeks. At the end of the four weeks, the concentration of H. pylori, the principal cause of peptic ulcer disease, was significantly reduced. This indicated the potency of these two vitamins in managing peptic ulcer disease since it eliminated the vector responsible for the condition. On the other hand, Mwafy and Afana [31] investigated the histopathological parameters of serum iron and vitamin B12 levels in hospitalized patients suffering from H. pylori infections and regular healthy patients as a control group. Results of the study showed that patients infected with H. pylori were deficient in vitamin B12 and iron compared to the control group. After treatment of the patients with omeprazole, amoxicillin, and clarithromycin, vitamin B12 and iron levels were normalized by the triple effect treatment. Iron and vitamin B12 levels can be a helpful marker for PUD. In addition to dietotherapy and the nutrients highlighted above, zinc and selenium can help accelerate healing. While zinc is essential in maintaining the immune system functions [32], selenium, on the other hand, helps to reduce disease complications and improve the healing process [33].
While no food can cause PUD, certain food items, such as spicy foods, caffeine, and alcohol, can hinder healing and worsen the symptoms in some patients. Table 3 summarizes the recommended foods that can help accelerate healing, those to be taken cautiously and foods that are prohibited in patients as they can slow the healing process and worsen symptoms.
Table 1: The types of conventional drugs used in the treatment of PUD.
| Drug class | Characteristics | Examples | References |
|---|---|---|---|
| Antacids |
Acid-neutralizing effect,
reduction of diarrhoea,
prevent erosion by gastric acid, increase gastric pH |
A combination of calcium and
aluminium carbonates, Aluminium Hydroxide, Magnesium hydroxide |
[34,35] |
| Gastric muscle stimulants | Accelerates gastric emptying | Domperidone and metoclopramide | [34] |
|
Mucosalincreasing resistance agents |
Protects the stomach’s mucus
lining from acid by
shielding it from acid damage |
Carafate (sucralfate),
Cytotec (misoprostol),
carbenoxo- lone, and chelated bismuthate |
[36] |
|
Antisecretory medications (anticholinergic agents and H2 antagonists) |
Inhibits gastric acid
secretion and reduces
gastric acidity, output, and volume. Histamin H2 receptor antagonist func- tions as a competitor antagonist with gastrin by inhibiting the binding and activity of histamine and reducing gastric acid release |
Anticholinergic agents
include phentonium,
atropine, py- oscyamine, methantheline, and propantheline while H₂ receptor antagonists include famotidine and cimetidine |
[34,37,38] |
|
Corticohypothal amic drugs |
Regulation of gastric
secretion in the central
nervous sys- tem. Inhibit the secretion of inflammatory cells |
Hydrocortisone, Cortisone,
Prednisone, Prednisolone, etc. |
[39,40] |
|
Proton pump inhibitors (PPIs) |
Inhibits H+/K+ ATPase in
parietal cells or blockage
of the site of gastric acid secretion in the parietal cell of the stomach thereby reducing it |
Omeprazole, Esomeprazole,
Pantoprazol, Vonoprazan, Rabeprazole, etc. |
[41,42] |
Table 2: Plant bioactive compounds in the management of peptic ulcer disease.
| Group | Bioactive compound | Source | Dose | Model used | Mode of action | Ref |
|---|---|---|---|---|---|---|
| Alkaloids | Total alkaloids | Phellodendron amurense |
30 mg/kg/day | Induction by acetic acid [0.14 mol/ L] in rats |
Significant increase in serotonin and nor- adrenaline levels, indicating the gastropro- tective effect of total alkaloids |
[43] |
| Total alkaloids | Mahonia bealei | 18.56 mg/kg/day | Induction of ulcers in rats by pyloric ligation |
Inhibition of H+/K+-ATPase release also caused a decrease in gastrin gastric acidity |
[44] | |
| Total Alkaloids | Coptis | 25 mg/kg/day | Acetic acidinduced peptic ulcer in rats |
Increases the level of epidermal growth factor (EGF), 5-hydroxytryptamine (5-HT) in the brain and noradrenaline (NE) in the adrenal tissue |
[45] | |
| Piperine | Piper nigrum | 100 mg/kg bw | Ethanolinduced ulcer in rats | Inhibition of ulcer in vitro and in vivo via oxidation by regulating the Nrf2/HO-1 and MAPK signalling pathways |
[46] | |
| Terpenes and Terpenoids | (−)-linalool | Dalbergia latifolia |
5; 10; 20; 40 mg/ kg/day |
Acetic acidinduced and abso- lute ethanol-induced peptic ulcer in rats |
10 mg/kg/day reduced lipid peroxidation in ethanolinduced ulcers and showed strong gastroprotective activity |
[47] |
| Geraniol | Cymbopogon citratus (lemongrass) |
1-100 mg/kg (p.o) |
Acute ethanol- and chronic acetic acidinduced ulcer in rat models |
Geraniol (3 mg/kg) accelerated the gastric healing process by 80.57%, and promoted healing on installed ulcer but did not inhibit the H+/K+- ATPase activity |
[48] | |
| Thymoquinone (TQ) |
Nigella sativa | 20 mg/kg | Acetylsalicylic acid (ASA) induced gastric ulcer in rats |
Reduction of TNF-α, ulcer indices, apop- tosis, total oxidant status, asymmetric dimethylarginine, Nuclear factor kappa- light-chainenhancer of activated B cells (NF-κB), and inducible nitric oxide synthase (iNOS) expressions |
[49] | |
| Flavones | Apigenin | Celery, parsley, and onions |
75 and 150 mg/ kg |
Atopic dermatitis itch model in mice using compound 48/80 |
Modulation of IL-31 mRNA, protein expres- sion protein expression, and inhibit the phosphorylation activation of Mitogen- activated protein kinase (MAPK) pathway and NF-κB cells. |
[50] |
| Luteolin | Coconut (Cocos nucifera L.) |
20 -100 μg/mL | Indomethacininduced gastric ulcer in human gastric adeno- carcinoma epithelial (AGS) |
Cytotoxic effect against human gastric adenocarcinoma epithelial |
[51] | |
| Coconut (Cocos nucifera L.) |
100 mg/kg and 200 mg/kg |
Diclofenac (DIC)-induced gas- troduodenal ulcers in rats |
Attenuation of gastroduodenal and hepatic damage |
[52] | ||
| chrysin | Flowers of Passiflora |
50 and 100 mg/ kg |
indomethacininduced gastric | Activation of peroxisome proliferator activated |
[53] | |
| incarnateI and Oroxylum indicum |
ulcer model in rats | receptor-ɣ (PPAR-ɣ) and downregulation of IL-6. Promote mucus secretion |
||||
| Tangeretin | Citrus peels | 100 mg/kg | Ethanolinduced acute peptic ulcer in rat model |
Exhibited anti-inflammatory functions by decreasing TNF-α, IL-6, and IL-1β and increasing the IL-10 levels |
[54] | |
| Nobiletin | Citrus fruits | Coculture of H. pylori in hu- man gastric epithelial (GES)-1 cell line |
Nobiletin prevents TNF-α, IL-6, COX-2, Phosphatidylinositol-3 kinase (PI3K), pro- tein kinase B (AKT), and mitogenactivated protein kinase molecules |
[55] | ||
| Isoflavones | Daidzein | Soybeans | 400 mg/kg, ip | Induction of lung inflam- mation by exposing mice to TNF-α |
Inhibition of proinflammatory chemokine Cxcl2 expression in lung tissues |
[56] |
| Genistein | Soybeans | 25 mg/kg orally | Single dose of indomethacin (80 mg/kg) orally |
Reduction of the expression of Wnt/β- catenin and transforming growth factor (TGF-β/SMAD4), and Protein Kinase B (PKB) pathways |
[57] | |
| Genistein | Soybeans | 16 mg/kg body weight |
H. pyloriinduced ulcer in rat model (108−1010 CFU/mL; 1 mL/rat) |
Significant reduction of proinflammatory cells (TNFα and cytokine-induced neutro- phil chemoattractant-1 (CINC-1) |
[58] | |
| Flavonols | Glycitein | Soybeans | 50 or 100 mg/ kg/d |
Water immersion restraint (WIR) stress model |
Suppression of TNF-α, cytokine-induced neutrophil chemoattractant (CINC)-1) lev- els, and reduction of mucosa injury |
[59] |
| Quercetin | Citrus fruits, grapes, apples, mangoes |
50 mg/kg | Ethanolinduced gastric ulcer in rat |
Upregulation of Nrf2 and HO1 and ecreased High mobility group box 1 (HMGB1), Toll- like receptor 4 (TLR4), NF-κB p65 and TNF-α |
[60] | |
| Myricetin | Mangoes, berries and red wine |
50 mg/kg | Histamine (20 mg/kg)-in- duced gastric ulcer |
Showed inhibitory effects on gastric H+ and K+-ATPase in a dose-dependent manner |
[61] | |
| Myricetin | Mangoes, berries and red wine |
12 mg/kg body weight |
Alcoholinduced peptic ulcer in rats |
Reduction of the level of malondialdehyde (MDA) and NF-κB) and increased total gluta- thione (GSSG/GSH), superoxide dismutase (SOD), cyclooxygenase-1 (COX-1) and prostaglandin E2 (PGE2) |
[62] | |
| Kaempferol | Spinach and kale | 40, 80, or 160 mg/kg b.w. |
Acute ethanolinduced lesions in mice mucosa |
Reduced ulcer index, myeloperoxidase (MPO) activity and TNF-α, and IL-1β levels, and improved nitric oxide (NO) levels |
[63] | |
| chalcones | Boesenbergin A (BA) |
Boesenbergia rotunda (L.) |
10 and 20 mg/kg body weight |
Ethanolinduced ulcer model in rats |
Reduction of the tumor necrosis factor- alpha (TNF-α) and Interleukin 6 (IL-6), with an increase in prostaglandin synthesis |
[64] |
| (1-(4-hydroxy- phenyl)-3-m-tolyl- propenone) (HPTP) |
250, 500, 1000 mg/kg) |
Indomethacininduced peptic ulcer in rats |
Decreased superoxide dismutase (SOD), Glutathione peroxidase (GPx) activity and prostaglandin E2 (PGE2) level and decrease MDA in a dose-dependent way |
[65] | ||
| Flavanones | Naringenin | grapes, tangelos, blood oranges, lemons, and tangerines |
10 and 20 mg/kg body weight |
Ethanolinduced in vivo in rats and ethanolstimulated KATO III cells in vitro |
Suppressed nuclear factorκB (NF-κB) and decreased NO, MDA, TNF-α, IL-6, IL-8, and myeloperoxidase (MPO), and (COX-2 activities |
[66] |
| Naringenin | grapes, tangelos, blood oranges, lemons, and tangerines |
100 mg/kg, ig | Indomethacininduced gastric ulcers in rats |
Reduction of TNF-α, IL-6, C-Reactive Protein (CRP), iNOS, and increased COX-2 levels. |
[67] | |
| Hesperidin | Citrus fruits | 20 mg/kg body weight |
Aspirin-induced peptic ulcer in rats |
Reduction of bleeding score of the gastric mucosa thereby reducing the damage caused to the gastric mucosa |
[68] | |
| Hesperidin | Citrus fruits | 1-10 mg/kg, p.o | Acetic acidinduced chronic gastric ulcer in rats |
Reduction of glutathione levels in the gastric mucosa tissue and normalized the superoxide dismutase and catalase activi- ties in a dosedependent way |
[69] | |
| Hesperidin | Citrus fruits | 50 mg/kg, p.o. | Ethanolinduced oxidative stress and peptic ulcer in rats. |
Increased the level of TNF-α and the ex- pression of COX2. A reduction of GPx, SOD, catalase (CAT), and Thiol groups. |
[70] | |
| Anthocyanins | Hirsutidin | Catharanthus roseus, Fruits and vegetables |
10 and 20 mg/kg | Ethanolinduced ulcer in rats | Increased oxidative stress, with an improve- ment in NO, prostaglandin E2, TNF-α, and inflammatory cytokines |
[71] |
| Anthocyanins | Black rice bran | 5, 25, and 50 mg/ kg bw |
Naproxeninduced gastric ulcer in rats |
Inhibition of lipid peroxidation, scavenging reactive oxygen species, regulation of ma- trix metalloproteinase-2 (MMP-2) activity |
[72] | |
| Anthocyanins (Anthocyanidins) | Cyanidin chloride | Red berries such as raspberries, blueber- ries, grapes, etc. |
5, 10, and 20 mg/kg per body weight |
Ethanolinduced gastric ulcer in rats |
Reduction in the levels of superoxide, catalase, myeloperoxidase, dismutase, and glutathione levels showing the dose-depen- dent effect of cyanidin chloride |
[73] |
| Delphinidin-3-Oglu- coside |
Pomegranate | 100 mg/kg orally | H. pyloriinduced ulcer in rats with a 9 McFarland (2.7×109 CFU) |
Reduction of TNF-α and increased expres- sion of autophagy-related genes (Beclin1, ATG5, and ATG12) |
[74] | |
| Petunidin Petunidin 3-O [rhamnopyranosyl- (trans-pcoumaroyl)]- 5-O[β-D-gluco- py- ranoside] |
Lycium ruthenicum Murray |
200 mg/kg/d | Dextran sodium sulfate (DSS) induced gastric ulcer in rats |
Blocking of proinflammatory cytokines (TNF-α, IL-6, IL-1, and IFN- γ). It also increased tight junction pro- tein and modulated gut microbiota |
[75] | |
| Peonidin | Euterpe oleracea, Banana |
30-300 mg/kg, p.o) or 3 mg/ kg, i.p. |
Ethanolinduced gastric ulcer in rats |
In-vitro radical scavenging activity and in vivo gastroprotective activity. There was also a normalization of SOD, an increase in CAT, with a decrease in MPO activity and TNF-a levels. |
[76] | |
| Malvidin | Berries | 5 mg/kg | Ethanol- NSAIDs- ischemi- areperfusion-, and acetic acidinduced |
Increased EGF gene and COX-1 expressions and down-regulation of MMP-9. Reduced the expression of toll-like receptor 4 (TLR4) and increased the haeme oxygenase 1 (HMOX-1) and IL-10. |
[77] | |
| Xanthones | Mangiferin | Mango (Mangifera indica L.) |
30 mg/kg peels and 10 mg/kg of pulp |
Naproxeninduced gastric ulcers in rat model |
Reduction of MDA content and MPO activ- ity. |
[78] |
| Mangiferin | Mango (Mangifera indica L.) |
3,10 and 30 mg/ kg, p.o. |
Ethanol- and indomethacinin- duced gastric ulcer in rats |
Reduction of ulcers by 63% and 57%, respectively. Reduction of acid production and reduced the sulfhydryl group to show its good antioxidant activity. |
[79] | |
| Mangiferin | Mango (Mangifera indica L.) |
10 and 20 mg/ kg Mangiferin |
Rat ischemia/ reperfusion model |
The gastroprotective effects of mangiferin through the Nrf2/HO-1, PPAR-γ/NF-κB sig- nalling pathways and the anti-inflammatory effects through the reduction of IL-1β and sE-selectin. |
[80] | |
| Flavan-3-ols | Epicatechin gallate | Bauhinia hookeri, apples, cherries, grapes, pears |
100-400 mg/kg p.o. |
Acetic acidinduced ulcers and hot plate models in rats |
Significant reduction in PGE2, TNF-α, IL-1β, and IL-6 in a dose- dependent way. |
[81] |
| (+)-catechin | Apples, red wine, blue- berries, green tea, etc. |
100 μg/mL | Inflammatory mediators using murine RAW 264.7 cells (4 × 105) |
Significant inhibition of TNF-α, nitrite, 5-LOX, COX, and iNOS and upregulation of IL-10 |
[82] | |
| Catechin | Apples, red wine, blue- berries, green tea, etc. |
35 mg/kg/day | Ketoprofeninduced gastric ulcer in rat models |
Reduction of total sulfhydryl groups and glutathione reductase and upregulation of Nrf2 both in vivo and in vitro |
[83] | |
| Capsaicinoid | Capsaicin | Red pepper (Capsicum annuum) |
2 mg/kg | Aspirin-induced ulcer in rats | Reduction of proinflammatory cytokines ((TNF-α, IL-1β, IL-6) and COX-2 in the rat model |
[84] |
Table 3: Foods allowed, prohibited and those which need to be taken with caution to manage PUD.
| Food product | Allowed | To be taken with caution | Prohibited foods |
|---|---|---|---|
| Fruits | Apple, papaya, melon, banana, mango | Orange, pineapple, acerola, passion fruit | Lemon |
| Milk and dairy products | Low-fat cheeses, yoghurt, fermented milk | Milk, Fatty cheeses (mascarpone, cream cheese, gorgonzola), |
Skimmed milk, low-fat cot- tage cheese |
| Oil seeds | Flaxseed, Brazilian nut, walnuts | - | - |
| Cereals | brown rice, bulgur, millet, and oatmeal | Baked products, white bread loaves, pasta, noodles, cookies |
- |
| Vegetables | Leafy dark green vegetables, carrot, beet, green bean, spinach, kale, radish, zucchini, leek |
Broccoli, cauliflower, cabbage, cucumber, onion, red pepper |
Spicy peppers (black pepper, chillies) |
| Oils and olive oils | Vegetable oils, olive oil | - | Fried foods, peanut butter |
| Meats | Lean meat (beef, pork, chicken, fish) | Fatty meats, organ meats and sausages | - |
| Legumes | Bean soup, lentils, chickpeas, soybean | Beans | - |
| Beverages | Natural juices, Green tea | Citrus/acidic fruit juices | Coffee, black tea, fizzy/cola drinks, alcoholic beverages |
| Sweets | - | Concentrated sweets | Chocolate and cocoa-based sweets |
| Others | Probiotics | Industrialized seasonings, Ketchup, mayonnaise | Mustard grain |
source: [23,24]
Conclusion
It has been deduced from the review that some of the significant plant bioactive compounds that have a track record in the management of peptic ulcer disease are in the major groups of alkaloids, terpenes and terpenoids, flavones, isoflavones, flavonols, chalcones, flavanones, anthocyanidins, xanthones, flavan3-ols, anthocyanins, and capsaicinoid. Most of these bioactive compounds work in a dose-dependent manner and express their therapeutic functions through the pro-inflammatory cytokines such as the TNF-α, IL-1β, and IL-6, reduction in prostaglandin E2 in both in vivo and in vitro models. The therapeutic effect of these bioactive compounds is also expressed through the radical scavenging activity and gastroprotective activity by normalizing the SOD, increased CAT, a decrease in MPO, NO, as well as in the suppression of Malondialdehyde (MDA) and nuclear factor-κB (NF-κB).
While no food product has a history of causing the PUD, there are some food items which need to be taken with caution or are prohibited by peptic ulcer patients. Some of these foods, such as spicy foods, caffeine, and alcohol, can hinder healing and worsen the symptoms in some patients. Understanding the nutritional needs of patients with PUD is one of the first and fundamental steps in formulating the required dietotherapy for this health challenge. As a rule of thumb, a balanced diet should always be provided in this course to manage the pathology. Unfortunately, there are scanty articles in the literature to elucidate the ideal dietotherapy of PUD.
Hence, there is a need to fill the gap through more research.
Abbreviations: 5-HT: 5-Hydroxytryptamine; AKT- Protein Kinase B; Baba: Antigen Adhesin; CAT: Catalase; CINC-1: CytokineInduced Neutrophil Chemoattractant-1; COX: Cyclo-Oxygenase; EGF: Epidermal Growth Factor; Gpx: Glutathione Peroxidase; Hcl- Hydrochloric Acid; HCO3 -: Bicarbonate; HMGB1: High Mobility Group Box 1; HMOX-1: Haeme Oxygenase 1; IL-1β: Interleukin-1 Beta IL-6 : Interleukin-6; Inos: Inducible Nitric Oxide Synthase; MAPK: Mitogen-Activated Protein Kinase; MDA: Malondialdehyde; MMP-2: Metalloproteinase-2; MPO: Myeloperoxidase; NE: Noradrenaline; NF-Κb: Nuclear Factor-Κb; NFΚb: Suppressed Nuclear Factor-Κb; NO: Nitric Oxide; NSAID: Non-Steroidal Anti-Inflammatory Drugs; Oipa: Outer Inflammatory Protein Adhesin; PGE2: Prostaglandin E2; Pgs: Prostaglandins; PI3K: Phosphatidylinositol-3 Kinase; PPAR-Ɣ: Peroxisome Proliferator Activated Receptor-Ɣ; Ppis: Proton Pump Inhibitors; PUD: Peptic Ulcer Disease; SOD: Superoxide Dismutase; TLR4: Toll-Like Receptor 4; TNF-Α: Tumor Necrosis Factor-Alpha.
Declarations
Conflict of interest: The authors declare that they have no competing interests to disclose
Funding: African-German Network of Excellence in Science (AGNES), and Sigma XI, the Scientific Research Honours Society with grant number G20221001-3797
Acknowledgement: The authors thank the African-German Network of Excellence in Science (AGNES) for granting Anchang Mumukom Maximus a Mobility Grant in 2023; the Grant is generously sponsored by the German Federal Ministry of Education and Research and supported by the Alexander von Humboldt Foundation. The authors also thank the Sigma Xi, The Scientific Research Honor Society for the Grants in Aid of Research awarded to Anchang Mumukom Maximus.
References
- Lanas A, Chan FKL. Peptic ulcer disease. Lancet. 2017; 390(10094): 613-24. http://dx.doi.org/10.1016/S0140-6736(16)32404-7.
- Galura GM, Chavez LO, Robles A, McCallum R. Gastroduodenal Injury: Role of Protective Factors. Curr Gastroenterol Rep. 2019; 21(8).
- Serafim C, Araruna ME, Júnior EA, Diniz M, Hiruma-Lima C, et al. A Review of the Role of Flavonoids in Peptic Ulcer (2010-2020). Molecules. 2020; 25(22): 1-32.
- Shafrir A, Shauly-Aharonov M, Katz LH, Paltiel O, Pickman Y, et al. The association between serum vitamin d levels and helicobacter pylori presence and eradication. Nutrients. 2021; 13(1): 1-12. https://doaj.org/article/efdc43e1e59544f9a4b8a8d66f99765e.
- Xie X, Ren K, Zhou Z, Dang C, Zhang H. The global, regional and national burden of peptic ulcer disease from 1990 to 2019: A population-based study. BMC Gastroenterol. 2022; 22(1): 1-13. https://doi.org/10.1186/s12876-022-02130-2.
- Szabo S, Yoshida M, Filakovszky J, Juhasz G. Stress is 80 Years Old: From Hans Selye Original Paper in 1936 to Recent Advances in GI Ulceration. Curr Pharm Des. 2017; 23(27).
- Basic-Denjagic, M, Calic-Pavlovic N, Aleckovic-Halilovic M. Peptic Ulcer Disease and Socioeconomic Status. Acta Medica Salin. 2018; 45: 25-9.
- Wang W, Jiang W, Zhu S, Sun X, Li PL, et al. Assessment of prevalence and risk factors of helicobacter pylori infection in an oilfield Community in Hebei, China. BMC Gastroenterol. 2019; 19(1): 4-11.
- Datta De D, Roychoudhury S. To be or not to be: The host genetic factor and beyond in Helicobacter pylori mediated gastro-duodenal diseases. World J Gastroenterol. 2015; 21(10): 2883-95. /pmc/articles/PMC4356907/.
- Lanas Á, Carrera-Lasfuentes P, Arguedas Y, García S, Bujanda L, et al. Risk of upper and lower gastrointestinal bleeding in patients taking nonsteroidal antiinflammatory drugs, antiplatelet agents, or anticoagulants. Clin Gastroenterol Hepatol. 2015; 13(5): 906-12.
- Drini M. Peptic ulcer disease and non-steroidal anti-inflammatory drugs. Aust Prescr. 2017; 40(3): 91. Available from: /pmc/articles/PMC5478398/.
- Agbor NE, Esemu SN, Ndip LM, Tanih NF, Smith SI, et al. Helicobacter pylori in patients with gastritis in West Cameroon: Prevalence and risk factors for infection. BMC Res Notes. 2018; 11(1): 1-6. Available from: https://doi.org/10.1186/s13104018-3662-5.
- Abbasi-Kangevari M, Ahmadi N, Fattahi N, Rezaei N, Malekpour MR, et al. Quality of care of peptic ulcer disease worldwide: A systematic analysis for the global burden of disease study 1990-2019. PLoS One. 2022; 17: 1-15. Available from: http://dx.doi.org/10.1371/journal.pone.0271284.
- Kavitt RT, Lipowska AM, Anyane-Yeboa A, Gralnek IM. Diagnosis and Treatment of Peptic Ulcer Disease. Am J Med. 2019; 132(4): 447-56. Available from: https://doi.org/10.1016/j.amjmed.2018.12.009.
- Archampong TNA, Asmah RH, Wiredu EK, Gyasi RK, Nkrumah KN. Factors associated with gastro-duodenal disease in patients undergoing upper GI endoscopy at the Korle-Bu Teaching Hospital, Accra, Ghana. Afr Health Sci. 2016; 16(2): 611-9.
- Umegbolu EI. Peptic ulcer disease in school children aged 2-11 years in Southeast Nigeria. Int J Res Med Sci. 2022; 10(5):1007. Available from: https://www.msjonline.org.
- Haruna SA. Prevalence and Risk Factors of Helicobacter Pylori Infection among Patients with Peptic Ulcer Disease Attendeing Muhammad Abdullahi Wase Teaching Hospital. Sch Acad J Biosci. 2023; 11(12): 467-73.
- Zhang W, Lian Y, Li Q, Sun L, Chen R, et al. Preventative and therapeutic potential of flavonoids in peptic ulcers. Vol. 25, Molecules. 2020.
- Malmi H, Kautiainen H, Virta LJ, Färkkilä N, Koskenpato J, et al. Incidence and complications of peptic ulcer disease requiring hospitalisation have markedly decreased in Finland. Aliment Pharmacol Ther. 2014; 39(5): 496-506.
- Fallone CA, Chiba N, van Zanten SV, Fischbach L, Gisbert JP, et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology. 2016; 151(1): 51-69.
- Yuan JQ, Tsoi KKF, Yang M, Wang JY, Threapleton DE, et al. Systematic review with network meta‐analysis: comparative effectiveness and safety of strategies for preventing NSAID‐associated gastrointestinal toxicity. Aliment Pharmacol Ther. 2016; 43(12): 1262-75.
- Hamedi S, Arian AA, Farzaei MH. Gastroprotective effect of aqueous stem bark extract of Ziziphus jujuba L. against HCl/ethanol-induced gastric mucosal injury in rats. J Tradit Chinese Med. 2015; 35(6): 666-70.
- Sheneni VD, Shaibu IE, Akomolafe AP. Peptic Ulcer Disease: A Look into Diet Therapy. J Dig Dis Hepatol. 2023; 195.
- Vomero ND, Colpo E. Nutritional care in peptic ulcer. Arq Bras Cir Dig. 2014; 27(4): 298-302.
- Health Link BC. Healthy Eating Guidelines for People with Peptic Ulcers. Br Columbia. 2021; 1-3. Available from: https://www.healthlinkbc.ca/healthy-eating.
- Marotta RB, Floch MH. Diet and nutrition in ulcer disease. Med Clin North Am. 1991; 75(4): 967-79.
- Rahantasoa Finaritra CFP, Andrianjafiarivony C, Randrianasolo F, Rajaonera AT, Samison LH. The Role of Diet and Hygiene in the Management of Digestive Haemorrhages on Peptic Ulcer Disease. Am Acad Sci Res J Eng Technol Sci. 2020; 71(1): 207-11. https://asrjetsjournal.org/index.php/American_Scientific_Journal/article/view/6090.
- Bae JY, Park WS, Kim HJ, Kim HS, Kang KK, et al. Protective Effect of Carotenoid Extract from Orange-Fleshed Sweet Potato on Gastric Ulcer in Mice by Inhibition of NO, IL-6 and PGE2 Production. Pharmaceuticals. 2021; 14(12).
- Yousaf A, Ali S, Bokhari ZH, Khalid AM, Sheikh MA. Protective Effect of Vitamin E on Indomethacin Induced Gastric Ulcers. J Rawalpindi Med Coll. 2014; 18(2). https://www.journalrmc.com/index.php/JRMC/article/view/362.
- Sezikli M, Çetinkaya ZA, Güzelbulut F, Çimen B, Özcan Ö, et al. Effects of Alpha Tocopherol and Ascorbic Acid on Helicobacter pylori Colonization and the Severity of Gastric Inflammation. Helicobacter. 2012; 17(2): 127-32.
- Mwafy SN, Afana WM. Hematological parameters, serum iron and vitamin B12 levels in hospitalized Palestinian adult patients infected with Helicobacter pylori: A case-control study. Hematol Transfus Cell Ther. 2018; 40(2): 160-5. https://doi.org/10.1016/j.htct.2017.11.010.
- Prasad AS. Zinc: Role in immunity, oxidative stress and chronic inflammation. Curr Opin Clin Nutr Metab Care. 2009; 12(6): 646-52.
- Ferguson M, Cook A, Rimmasch H, Bender S, Voss A. Pressure ulcer management: The importance of nutrition. Medsurg Nurs. 2000; 9(4): 163.
- Saheed S, Oladipo AE, Sunmonu TO, Balogun FO, Ashafa AOT. The Purview of Phytotherapy in the Management of Gastric Ulcer. In: Stomach Disorders. 2018.
- Salisbury BH, Terrell JM. Antacids. In: StatPearls. StatPearls Publishing; 2022.
- Safavi M. Treatment of Helicobacter pylori infection: Current and future insights. World J Clin Cases. 2016; 4(1): 5.
- Compta Y, Tolosa E. Anticholinergic Medications. In: Handbook of Clinical Neurology. StatPearls Publishing. 2022; 121-5. https://www.ncbi.nlm.nih.gov/books/NBK555893/.
- Sharifi-Rad M, Fokou PVT, Sharopov F, Martorell M, Ademiluyi AO, et al. Antiulcer agents: From plant extracts to phytochemicals in healing promotion. Molecules. 2018; 23(7): 1-37.
- Ericson-Neilsen W, Kaye AD. Steroids: Pharmacology, complications, and practice delivery issues. Ochsner J. 2014; 14(2): 203-7.
- Kapugi M, Cunningham K. Corticosteroids. Orthop Nurs. 2019; 38(5): 336-9.
- He HS, Li BY, Chen QT, Song CY, Shi J, et al. Comparison of the use of vonoprazan and proton pump inhibitors for the treatment of peptic ulcers resulting from endoscopic submucosal dissection: A systematic review and meta-analysis. Med Sci Monit. 2019; 25: 1169-76. https://www.medscimonit.com/abstract/index/idArt/911886.
- Sykes BW. Courses for horses: Rethinking the use of proton pump inhibitors in the treatment of equine gastric ulcer syndrome. Equine Vet Educ. 2019; 31(8): 441-6.
- Wang L, Wang X, Zhu XM, Liu YQ, Du WJ, et al. Gastroprotective Effect of Alkaloids from Cortex Phellodendri on Gastric Ulcers in Rats through Neurohumoral Regulation. Planta Med. 2017; 83(3-4): 277-84.
- Zhang SL, Li H, He X, Zhang R, Q Sun, Y. H, et al. Alkaloids from Mahonia bealei posses anti-H+/K +-ATPase and antigastrin effects on pyloric ligation-induced gastric ulcer in rats. Phytomedicine. 2014; 21(11): 1356-63. http://dx.doi.org/10.1016/j.phymed.2014.07.007.
- Duan Q, Li Y, Qin F. Research on the protection and mechanism of coptis alkaloids on acetic acid type gastric ulcer. J Phys Conf Ser. 2020; 1629(1).
- Duan Z, Yu S, Wang S, Deng H, Guo L, et al. Protective Effects of Piperine on Ethanol-Induced Gastric Mucosa Injury by Oxidative Stress Inhibition. Nutrients. 2022; 14(22): 4744.
- da Silva FV, de Barros Fernandes H, Oliveira IS, Viana AFSC, da Costa DS, Lopes MTP, et al. Beta-cyclodextrin enhanced gastroprotective effect of (−)-linalool, a monoterpene present in rosewood essential oil, in gastric lesion models. Naunyn Schmiedebergs Arch Pharmacol. 2016; 389(11): 1245-51.
- Venzon L, Mariano LNB, Somensi LB, Boeing T, de Souza P, et al. Essential oil of Cymbopogon citratus (lemongrass) and geraniol, but not citral, promote gastric healing activity in mice. Biomed Pharmacother. 2018; 98: 118-24. https://doi.org/10.1016/j.biopha.2017.12.020.
- Zeren S, Bayhan Z, Kocak FE, Kocak C, Akcilar R, et al. Gastroprotective effects of sulforaphane and thymoquinone against acetylsalicylic acid-induced gastric ulcer in rats. J Surg Res. 2016; 203(2): 348-59. http://dx.doi.org/10.1016/j.jss.2016.03.027.
- Che DN, Cho BO, Shin JY, Kang HJ, Kim JS, et al. Apigenin inhibits IL-31 cytokine in human mast cell and mouse skin tissues. Molecules. 2019; 24(7).
- Abiraami VS, Uma GS. Promising role of luteolin from the sprouts of Cocos nucifera L. in indomethacin-induced gastric ulcer of human gastric adenocarcinoma cell line. J Adv Sci Res. 2021; 12(1): 213-27. http://www.sciensage.info/journal/1359303580JASR_3006121.pdf
- Akinrinde AS, Soetan KO, Tijani MO. Exacerbation of diclofenacinduced gastroenterohepatic damage by concomitant exposure to sodium fluoride in rats: Protective role of luteolin. Drug Chem Toxicol. 2022; 45(3): 999-1011. https://doi.org/10.1080/01480545.2020.1802478.
- George MY, Esmat A, Tadros MG, El-Demerdash E. In vivo cellular and molecular gastroprotective mechanisms of chrysin; Emphasis on oxidative stress, inflammation and angiogenesis. Eur J Pharmacol. 2018; 818: 486-98. https://doi.org/10.1016/j.ejphar.2017.11.008.
- Susam S, Nevin İ, Tedik F, Berk B, İ AŞ, et al. The protective effect of tangeretin and pomegranate separately and in combination on ethanol-induced acute gastric ulcer model. Cukurova Med J. 2023; 48(3): 859-67.
- Ouyang Y, Li L, Ling P. Nobiletin inhibits helicobacterium pylori infection-induced gastric carcinogenic signaling by blocking inflammation, apoptosis, and mitogen-activated protein kinase events in gastric epithelial-1 cells. J Environ Pathol Toxicol Oncol. 2020; 39(1): 77-88.
- Li HY, Pan L, Ke YS, Batnasan E, Jin XQ, et al. Daidzein suppresses proinflammatory chemokine Cxcl2 transcription in TNF-αstimulated murine lung epithelial cells via depressing PARP-1 activity. Acta Pharmacol Sin. 2014; 35(4): 496-503.
- Hassan HM, Alatawi NM, Bagalagel A, Diri R, Noor A, et al. Genistein ameliorated experimentally induced gastric ulcer in rats via inhibiting gastric tissues fibrosis by modulating Wnt/βcatenin/TGF-β/PKB pathway. Redox Rep. 2023; 28(1): 2218679.
- Siriviriyakul P, Werawatganon D, Phetnoo N, Somanawat K, Chatsuwan T, et al. Genistein attenuated gastric inflammation and apoptosis in Helicobacter pylori-induced gastropathy in rats. BMC Gastroenterol.2020; 20(1): 1-9. https://doi.org/10.1186/s12876-020-01555-x.
- Takekawa S, Matsui T, Arakawa Y. The protective effect of the soybean polyphenol genistein against stress-induced gastric mucosal lesions in rats, and its hormonal mechanisms. J Nutr Sci Vitaminol (Tokyo). 2006; 52(4): 274-80.
- Shams SGE, Eissa RG. Amelioration of ethanol-induced gastric ulcer in rats by quercetin: Implication of Nrf2/HO1 and HMGB1/TLR4/NF-κB pathways. Heliyon. 2022; 8(10): e11159. https://doi.org/10.1016/j.heliyon.2022.e11159.
- Miyazaki Y, Ichimura A, Sato S, Fujii T, Oishi S, et al. The natural flavonoid myricetin inhibits gastric H+, K+-ATPase. Eur J Pharmacol. 2018; 820: 217-21. https://doi.org/10.1016/j.ejphar.2017.12.042.
- Park HS, Seo CS, Baek EB, Rho JH, Won YS, et al. Gastroprotective Effect of Myricetin on Ethanol-Induced Acute Gastric Injury in Rats. Evidence-based Complement Altern Med. 2021; 2021.
- Li, Q, Hu, X, Xuan, Y, Ying, J, Fei, Y, et al. Kaempferol protects ethanol-induced gastric ulcers in mice via pro-inflammatory cytokines and NO. Acta Biochim Biophys Sin (Shanghai). 2018; 50(3): 246-53.
- Mohan S, Hobani YH, Shaheen E, Abou-Elhamd AS, Abdelhaleem A, et al. Ameliorative effect of Boesenbergin A, a chalcone isolated from Boesenbergia rotunda (Fingerroot) on oxidative stress and inflammation in ethanol-induced gastric ulcer in vivo. J Ethnopharmacol. 2020; 261: 113104. https://doi.org/10.1016/j.jep.2020.113104.
- Dhiyaaldeen SM, Amin ZA, Darvish PH, Mustafa IF, Jamil MM, et al. Protective effects of (1-(4-hydroxy-phenyl)-3-m-tolyl-propenone chalcone in indomethacin-induced gastric erosive damage in rats. BMC Vet Res. 2014; 10(1): 1-14.
- Li WS, Lin SC, Chu CH, Chang YK, Zhang X, et al. The gastroprotective effect of naringenin against ethanol-induced gastric ulcers in mice through inhibiting oxidative and inflammatory responses. Int J Mol Sci. 2021; 22(21).
- Sengul E, Gelen V. Protective effects of naringin in indomethacin-induced gastric ulcer in rats. GSC Biol Pharm Sci. 2019; 8(2): 006-14.
- Shimamura Y, Sei S, Nomura S, Masuda S. Protective effects of dried mature Citrus unshiu peel (Chenpi) and hesperidin on aspirin-induced oxidative damage. J Clin Biochem Nutr. 2021; 68(2): 149-55.
- da Silva LM, Pezzini BC, Somensi LB, Bolda Mariano LN, Mariott M, et al. Hesperidin, a citrus flavanone glycoside, accelerates the gastric healing process of acetic acid-induced ulcer in rats. Chem Biol Interact. 2019; 308: 45-50. https://doi.org/10.1016/j.cbi.2019.05.011.
- Selmi S, Rtibi K, Grami D, Sebai H, Marzouki L. Protective effects of orange (Citrus sinensis L.) peel aqueous extract and hesperidin on oxidative stress and peptic ulcer induced by alcohol in rat. Lipids Health Dis. 2017; 16(1): 1-12.
- Alharbi KS, Al-Abbasi FA, Alzarea SI, Afzal O, Altamimi ASA, et al. Effects of the Anthocyanin Hirsutidin on Gastric Ulcers: Improved Healing through Antioxidant Mechanisms. J Nat Prod. 2022; 85(10): 2406-12.
- Kim SJ, Park YS, Paik HD, Chang HI. Effect of anthocyanins on expression of matrix metalloproteinase-2 in naproxen-induced gastric ulcers. Br J Nutr. 2011; 106(12): 1792- 801.
- Zarricueta ML, Fagundes FL, Pereira QC, Pantaleão SQ, Dos Santos R de C. Relationship between Hormonal Modulation and Gastroprotective Activity of Malvidin and Cyanidin Chloride: In Vivo and In Silico Approach. Pharmaceutics. 2022; 14(3).
- Ragab AE, Al-Madboly LA, Al-Ashmawy GM, Saber-Ayad M, AboSaif MA. Unravelling the In Vitro and In Vivo Anti-Helicobacter pylori Effect of Delphinidin-3-OGlucoside Rich Extract from Pomegranate Exocarp: Enhancing Autophagy and Downregulating TNF-α and COX2. Antioxidants. 2022; 11(9): 1752.
- Peng Y, Yan Y, Wan P, Chen D, Ding Y, et al. Gut microbiota modulation and anti-inflammatory properties of anthocyanins from the fruits of Lycium ruthenicum Murray in dextran sodium sulfate-induced colitis in mice. Free Radic Biol Med. 2019; 136: 96-108.
- Cury BJ, Boeing T, Somensi LB, Mariano LNB, de Andrade SF, et al. Açaí berries (Euterpe oleracea Mart.) dried extract improves ethanol-induced ulcer in rats. J Pharm Pharmacol.2020; 72(9): 1239-44.
- Fagundes FL, Pereira QC, Zarricueta ML, Dos Santos R de C. Malvidin protects against and repairs peptic ulcers in mice by alleviating oxidative stress and inflammation. Nutrients. 2021; 13(10).
- Ferreira Gomes CC, de Siqueira Oliveira L, Rodrigues DC, Ribeiro PRV, Canuto KM, Duarte ASG, et al. Evidence for antioxidant and anti-inflammatory potential of mango (Mangifera indica L.) in naproxen-induced gastric lesions in rat. J Food Biochem. 2022; 46(3): 1-15.
- Carvalho ACS, Guedes MM, de Souza AL, Trevisan MT, Lima AF, et al. Gastroprotective effect of mangiferin, a xanthonoid from Mangifera indica, against gastric injury induced by ethanol and indomethacin in rodents. Planta Med. 2007;73(13):1372-6.
- Mahmoud-Awny M, Attia AS, Abd-Ellah MF, El-Abhar HS. Mangiferin mitigates gastric ulcer in ischemia/reperfused rats: Involvement of PPAR-γ, NF-κB and Nrf2/HO-1 Signaling Pathways. PLoS One. 2015; 10(7): 1-14.
- Al-Sayed E, Abdel-Daim MM. Analgesic and anti-inflammatory activities of epicatechin gallate from Bauhinia hookeri. Drug Dev Res. 2018; 79(4): 157-64.
- Sunil MA, Sunitha VS, Santhakumaran P, Mohan MC, Jose MS, et al. Protective effect of (+)-catechin against lipopolysaccharideinduced inflammatory response in RAW 264.7 cells through downregulation of NF-κB and p38 MAPK. Inflammopharmacology. 2021; 29(4): 1139-55. https://doi.org/10.1007/s10787-021-00827-6.
- Cheng YT, Wu CH, Ho CY, Yen GC. Catechin protects against ketoprofen-induced oxidative damage of the gastric mucosa by upregulating Nrf2 in vitro and in vivo. J Nutr Biochem. 2013; 24(2): 475-83. http://dx.doi.org/10.1016/j.jnutbio.2012.01.010.
- Mendivil EJ, Sandoval-Rodriguez A, Meza-Ríos A, Zuñiga-Ramos L, DominguezRosales A, et al. Capsaicin induces a protective effect on gastric mucosa along with decreased expression of inflammatory molecules in a gastritis model. J Funct Foods. 2019; 59: 345-51. https://doi.org/10.1016/j.jff.2019.06.002.