
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Paracentesis - haemodynamic effects of large-volume paracentesis (LVP)
Grajecki Donata1*; Bibizza Eric2; Just Isabell A3,4; Feldheiser A5; Wiedenmann Bertram1
1Medical Department, Division of Hepatology and Gastroenterology (Including Metabolic Diseases), Charité - University Medicine Berlin, Augustenburger Platz 1, 13359 Berlin, Germany.
§Department of Internal Medicine - Gastroenterology, Schlosspark Clinic, Berlin, Germany.
2Medical Biometry and Epidemiology, University Hospital Hamburg-Eppendorf, Martinistrasse 52, 20246 Hamburg, Germany.
3Department of Cardiothoracic and Vascular Surgery, Deutsches Herzzentrum Charité, Augustenburger Platz 1, 13359 Berlin, Germany.
4DZHK (German Centre for Cardiovascular Research), Partner Site Berlin, Berlin, Germany.
5Department of Anaesthesiology and Intensive Care Medicine, Charité - University Medicine Berlin, Augustenburger Platz 1, 13359 Berlin, Germany.
*Corresponding Author : Grajecki Donata
Medical Department, Division of Hepatology and Gastroenterology (including Metabolic Diseases), Charité -
University Medicine Berlin, Augustenburger Platz 1, 13359
Berlin, Germany.
Received : Apr 21, 2024
Accepted : May 10, 2024
Published : May 17, 2024
Archived : www.jjgastro.com
Copyright : © Donata G (2024).
Abstract
Introduction: Ascites is one of the manifestations of acute decompensation of liver cirrhosis. Study results in recent years indicate that liver cirrhosis is a systemic inflammation and leads to altered haemodynamics in addition to organ complications. The haemodynamic effects of paracentesis on the disturbed circulation must therefore be reconsidered.
Methods: Observational study of 21 patients who underwent haemodynamic and laboratory monitoring before, under and up to 48 hours after paracentesis with albumin substitution using noninvasive haemodynamic monitoring (esCCO TM System®, Nihon Kohden, Japan).
Results/Discussion: Patients with liver cirrhosis showed a significant decrease in systolic blood pressure (mean 117.10 mmHg SD +/- 21.9 to 112.96 mmHg +/- SD +/- 12.52 mmHg; p=0.044) and diastolic blood pressure (mean 69.05 mmHg SD +/- 13.34 to minimum 57 mmHg +/- SD +/- 12.49 mmHg; p<0.001) under paracentesis. Previous values were not reached even after 24 h (systolic blood pressure 24 h after invention: 112.95 mmHg SD +/- 21.59 mmHg p=0.0085, diastolic blood pressure 67 mm Hg SD +/- 13.17; p=0.03). Within the subgroups, there were different trends: Patients with higher MELD score showed an increase in stroke volume and cardiac output compared to patients with lower MELD score.
Conclusion: Paracentesis leads to an influence on the haemodynamics of patients with liver cirrhosis independent of albumin substitution, which is also detectable up to 48 hours after the intervention. There are indications that the stage of cirrhosis could be an influencing factor.
Keywords: Liver cirrhosis; Ascites; Paracentesis; Cancer; Haemodynamic changes.
Citation: Donata G, Eric B, Isabell AJ, Feldheiser A, Bertram W. Paracentesis - haemodynamic effects of large-volume paracentesis (LVP). J Gastroenterol Res Pract. 2024; 4(5): 1201.
Introduction
The development of ascites is one of the manifestations of decompensated liver cirrhosis.
While in the past the development of ascites was primarily attributed to portal hypertension and hypalbuminemia, there is increasing evidence that the course of liver cirrhosis and its complications are influenced by systemic inflammation (systemic inflammation hypothesis) [1-3].
Here, increased intestinal translocation of intraluminal bacteria and bacterial components (pathogen-associated molecular patterns, PAMPs) in particular appear to induce increased Nitric Oxide (NO) release via a release of pro-inflammatory cytokines [4,5]. However, the inflammatory processes also appear to have a systemic effect and exacerbate hyperdynamic circulatory states [2,1]. Significantly, however, endothelial NOproducing Nitric Oxide Synthase (eNOS) is not only stimulated by inflammatory processes or VEGF-associated but can also be influenced by mechanical forces [6,7].
Thus, vasodilation is present in the splanchnic area, whereas the systemic circulation - as cirrhosis progresses - shows an increasing hyperdynamic circulatory situation with signs of central underfilling and peripheral local vasoconstriction [8]. In addition to an increased plasma volume, an increased heart rate and cardiac index are found. At the same time, systemic resistance, as well as blood pressure, is reduced. The sympathetic and neurohumoral nervous systems are highly active [2].
A possible consequence of hyperdynamic circulation is manifested in the phenotype of cirrhotic cardiomyopathy with impaired contractility under stress, altered diastolic relaxation and electrophysiological abnormalities [9]. In particular, diastolic dysfunction appears to persist early and is associated with poor outcome [10]. Again, there is evidence that systemic inflammation maintains a hyperdynamic circuit and contributes significantly to the development of hepatic cardiomyopathy [11,12].
The treatment of uncomplicated ascites includes negative sodium balance and diuretic therapy, third-degree ascites is treated by large-volume paracentesis under albumin infusion. This is an overall low-risk procedure; local complications such as bleeding or bowel perforation are rare [13]. Far more significant, however, are the hemodynamic changes that can occur as a result of Large-Volume Paracentesis (LVP):
Systemic circulatory changes after large volume paracentesis (LVP) were first described in the late 1960s [14,15]. Several hypotheses regarding circulatory changes have been postulated: The original hypothesis was that there was a secondary fluid shift and decreased circulatory volume under LVP [16]. Further considerations included decreased systemic resistance due to improved right ventricular filling and activation of cardiac volume receptors via a vegetative reflex mechanism [17]. Another consideration was that there may be a direct influence on systemic circulation by influencing Intra-Abdominal Pressure (IAP) via myogenic vasoconstriction or mechanical compression of the splanchnic bed [18,19]. This hypothesis could be explained by influencing endothelial NO-producing Nitric Oxide Synthase (eNOS). However, another similar explanation could be that paracentesis leads to enhanced bacterial translocation, leading to hemodynamic effects via enhanced NO release [1].
Gines et al. demonstrated that the incidence of hemodynamic, renal, and endocrinologic changes under paracentesis was due to a significant increase in plasma renin activity and defined this reaction as post-Paracentesis-Induced Circulatory Dysfunction (PICD) [20]. The circulatory impairments observed included a reduction in mean arterial blood pressure, a decrease in systemic resistance, and changes in cardiac index [21]. The occurrence of PICD has been associated with rapid recurrence of ascites, acute renal failure, hyponatremia, and increased mortality [22,8]. Numerous follow-up studies have shown that albumin substitution after intervention can significantly reduce neurohumoral activation [23].
However, the hemodynamic changes under and after paracentesis are also detectable independently of the development of a PICD [24-26].
This raises the question of the effects of large-volume paracentesis on the haemodynamics of patients with liver cirrhosis and whether there is any evidence for explanatory causes.
The present study, therefore, examines non-invasively the changes in haemodynamics under paracentesis and combines this with close monitoring of blood sampling, control of infectious values and clinical follow-up parameters in patients with liver cirrhosis.
Methods
Study population and design
Study protocoll was originated in 2016, study investigation was approved by the Ethics Committee of Charité, Universitatsmedizin Berlin in April 2016 (EA2/052/16). Written informed consent to participate in the study was obtained from each patient. PARACENTESIS was registered in ClinicalTrials.gov (ClinicalTrials.gov Identifier: NCT02799160).
Recruiting started in October 2016, 52 patients were screened until December 2017. All patients had puncturable ascites caused by progressed liver cirrhosis diagnosed by ultrasound, biological or histological criteria. 21 patients passed the inclusion criteria:
Admitted patients at our institution between 18 and 70 years with liver cirrhosis and puncturable ascites. Exclusion criteria were clinical signs of infection in the last four weeks, alcohol abuse, hepatic encephalopathic stage III or more based on West Haven Criteria [27], chronic heartfailure, atrial defibrillation, implanted pacemaker and hepatorenal syndrome I or II. For this purpose, patients underwent laboratory incl. microbiological testing and electrocardiograms besides clinical history and physical examination. After written informed consent, blood collection was obtained from every patient to rule out an exclusion criteria and to evaluate thrombocythemia or coagulopathy. Laboratory results were performed at Institute of Laboratory Medicine, Clinical Chemistry and Pathobiochemistry, Charité. According to the institutional standard operation procedures every patient with thrombocytes <50.000/ul or INR>1,5 were transfused with thrombocytes or fresh frozen plasma or PPSB. The puncture site was determined following abdominal ultrasound. Every patient received 8 g of albumin per 1000 ml ascites removal, starting with 3000 ml of ascites removed [28]. To determine complications, side effects and outcome after the intervention, the follow-up period was se up to 14 days after the intervention.
Haemodynamic and laboratory measurement
After the first blood results were checked, the patient had to lie down for 10 min before the first hemodynamic measurement was started. The esCCOTM System® (Nihon Kohden, Japan) based on Pulse Wave Transit Time (PWTT) in combination with oscillometric measurements on the upper-arm to determine arterial pressuresis non-invasive monitoring (ECG, SpO2 and NIBP or IBP) measuring the time from the peak of the R-wave in the ECG to the rising point of the pulse waveform sensed by a SpO2 finger to derive continuously Cardiac Output (CO) and Stroke Volume (SV) as described before [29].
At the beginning of the paracentesis the second blood sample was collected and the continuous hemodynamic monitoring started with a pulse, ECG and pulse oximetry. Every 4 minutes blood pressure, Stroke Volume (SV) and estimated Cardiac Output (CO) were measured and calculated. After 50% of drainable ascites were removed, the third blood sample was collected. Up to 6000 ml ascites was removed, a fourth blood collection was taken. After 12 hours, hemodynamical measurement was repeated. The fifth and sixth blood sample were collected after 24 and 48 hours with a combined hemodynamical measurement. Twenty-four hours of fluid balance protocol was recorded for every patient.
Laboratory parameters
Every blood collection contained a complete blood count, blood gas analysis and renal parameters, electrolytes, osmolality, transaminases, bilirubin, albumin, c-reactive protein and procalcitonin.
Health status
In addition to haemodynamic and laboratory measurements, each patient received an EQ-5D questionnaire developed for this study before and 48 hours after the intervention.
Statistics
The evaluation of the following study is based on the initial research question primarily from an exploratory point of view.
To obtain a basic overview, the available data were initially descriptively analysed with simple methods such as contingency analysis and t-test for statistical significance (part 1). Conspicuous correlations were then selected and further analysed and verified by more complex statistical methods such as linear and non-linear mixed effect models (part 2).
In the descriptive analysis, p-values of less than 0.2 were defined as conspicuous. Alternatively, variables could be included in the model based on a clinically justifiable theory.
As an estimation matrix in the mixed effect models, robust methods such as the restricted maximum likelihood method were used to improve the estimation`s reliability. The individual heterogeneity was considered a random effect. An autoregression first order was assumed as covariance structure if measurement repetitions were present. If no repetitions of measurements were observed, a random intercept model was used instead.
Within these models, a variable selection was performed utilising backward selection. The variables were selected several times in different constellations to reduce random confounding
In the final considerations, p-values <0.05 were considered statistically significant. Due to the explorative approach, no adjustment to multiple testing is made.
After finalisation of an analysis model, the dependent variables were tested and described with these models.
The analysis showed that women had significantly worse results than men in some parameters. At the same time, the women also showed a significantly worse MELD score. The question arose as to whether the effects were due more to gender or the MELD score. Due to the extremely small number of 4 women, a unique method was necessary to analyse this question. In particular, a bootstrap resampling method was used to test utilising a simulation to which of the two parameters the effect was most likely to be due. This method is precarious due to the small number of cases of 4 women and the resulting data density should be interpreted extremely carefully. Nevertheless, it at least allows attenuating the guesswork regarding the effect and generating a slightly substantiated hypothesis. The analysis was performed using SAS software version 27-M1 (SAS Institute Inc.)
Results
Of 52 patients studied, 21 met the inclusion criteria, one patient was excluded due to septal ascites. In total, 21 patients had an average of 4600 ml of ascites SD +/- 1294 ml removed. The main characteristics of the patients are summarised in Table 1.
Haemodynamic data
Changes in systolic (SBP) and Diastolic Blood Pressure (DBP): Under paracentesis, systolic and diastolic blood pressure decreased significantly in all patients (SBP 117.10 mmHg SD +/- 21.86 to 112.96 mmHg SD +/- 12.52 mmHg (delta SBP-4.14 mmHg, 95% CI [-8.10; -0.28]; p=0. 044 and DBP 69.05 mmHg SD +/- 13.34 to a minimum of 57 mmHg SD +/- 12.49 mmHg (delta RR diastolic -5.71 mmHg, 95% CI [-8.82; -2.61]; p<0.001).
While systolic blood pressure remained decreased until 24 h after the intervention, diastolic pressure showed an increasing trend (SBP 112.95 mmHg SD +/- 21.59 mmHg (delta RR systolic - 4.67 mmHg, 95% CI [-7.99; -0.83]; p=0.0085. DBP: 67 mmHg SD +/- 13.17 mmHg at 24 hours (delta RR diastolic -3.14 mmHg, 95% CI [-6.90-0.62]; p=0.03).
After 48 hours, a further increase in systolic and diastolic blood pressure to near baseline values was detected, but this was no longer statistically significant. See also Figures 1 and 2.
Changes in haemodynamics according to subgroups: Strikingly, there appeared to be significant gender differences, although important characteristics such as age or concomitant cardiovascular diseases did not differ:
Systolic blood pressure was initially higher in men compared to women (men mean 119.65 mmHg SD +/- 20.80 vs women 102.67 mmHg SD +/- 26.69 mmHg, p=0.025). In men, the value decreased to a minimum of 88 mmHg SD +/- 21.07 mmHg (delta RR systolic -5.35 mmHg; 95% [-10.51; -0.12]) during the intervention. Women started with a lower systolic blood pressure, which, however, remained almost stable under the intervention (+ 1.0 mmHg SD +/- 2.45 mmHg). This effect was significant between the two sexes (p=0.031). The divergent trend was also seen for diastolic blood pressure between the two groups and continued until 48h after intervention Table 2.
Changes in haemodynamics in the presence of cancer: Patients with tumour disease (5 of 6 patients with hepatocellular carcinoma) had higher systolic and diastolic blood pressure compared with non-tumour patients (SBP initial 132.83 mmHg SD +/- 24.63 mmHg vs. 110.36 mmHg SD +/- 17.38 mmHg, p=0. 015 and 75.67 mmHg SD +/- 13.74 mmHg vs. 66.21 mmHg SD +/- 12.60 mmHg, respectively; p=0.0581. After the intervention, systolic as well as diastolic blood pressure decreased in patients with cancer (SBP 125 mmHg SD +/- 39.60 mmHg; DPB 61 mmHg SD +/- 11.3 mmHg), but almost returned to baseline values after 24h.
Stroke volume (esSV): Under intervention, SV was almost stable in all patients with a minimal decrease (mean 86.35 ml, delta esSV - 0.81 ml; 95% [-2.96; 1.34]; p=0.44).
Changes in haemodynamics by subgroup: Considering the subgroups, there was a significant difference in initial stroke volume between male and female patients (males 90.1 ml vs females 62 ml, delta esSV 28.1 95% CI [10.20; 47.32]; p=0.0043). While men´s stroke volume showed no significant changes, women´s stroke volume increased to an average of 74.25 ml SD +/- 12.71 ml (95% CI [54.02; 94.47]; delta esSV + 12.25 ml) after 24 hours. This effect was highly significant between the two groups (p=0.01). After 48 hours, no further effects on stroke volume were detectable (men mean 85.47 ml vs women 74.00 ml), but the effect of the intervention in the male and female groups compared with the initial measurements was still observable (delta esSV men - 5.29 ml SD +/- 13.62 ml vs delta women + 12.00 ml SD +/- 11.74 ml; p=0.031). Figure 3.
Changes in haemodynamics in the presence of cancer: In a comparison of tumour and non-tumour patients, patients with tumour disease showed a significantly higher stroke volume (non-malignancy mean 80.01 ml SD +/- 15.90 ml, 95% CI 71.26-88.81; malignancy 98.33 ml SD +/- 22.58 ml, 95 CI [74.64; 122]; p=0.048). A difference between the two groups was also detected after 24h (non-tumour patients mean 78.60 ml SD +/- 12.57 ml, 95% CI [71.63; 85.56]; tumour patients mean 99.00 ml SD +/- 26.56 ml, 95% CI 71.12 - 127; p=0.025).
Cardiac Output (CO): Cardiac output in all patients decreased from an initial mean of 6.42 l/min to 6.28 l/min SD +/- 0.49 l/ min immediately after intervention (delta esCCO - 0.12 l/min SD + 0.80 l/min, 95% CI [-0.4863; 0.244]; p=0.047). At 24 hours, cardiac output was still decreasing (delta esCCO - 0.36 SD 1.13, 95% CI [-0.87; -0.16]; p=0.0024) and was still reduced to the original esCCO at 48 hours (delta esCCO - 0.34 SD +/- 1.21, 95% CI [-0.89; -0.21]; p=0.037).
Changes in haemodynamics by subgroup: Similar to stroke volume, cardiac output differed significantly between men and women (male patients mean 6.68 l/min SD +/- 1.34 l/min, 95% CI [5.99; 7.37] vs female patients 4.92 l/min SD +/- 0.26 l/min, 95% CI [4.29; 5.55]; p=0.039). This was also seen in cardiac index, which was significant between the sexes (males mean 3.23 l/min/m2 SD +/- 0.64 l/min/m2 , CI 95% 2.89 - 3.56 vs females mean 2.76 l/min/m2 SD +/- 0.14 l/min/m2 , CI 95% 2.40 - 3.13 l/ min/m2 ; p=0.044).
After the puncture, males showed a slightly reduced CO (male patients mean 6.36 l/min SD +/- 1.29 l/min, 95% CI [5.70; 7.02]), but female patients had a higher mean esCCO of 5.84 l/ min SD +/- 1.14 l/min, 95% CI [4.03; 7.66]; p=0.47). This effect was insignificant but showed a clear trend concerning cardiac index (p=0.08).
Changes in haemodynamics in the presence of cancer: When comparing patients with tumour disease in the non-tumour group, a higher cardiac output was found (non-malignant mean 6.10 l/min SD +/- 1.10 l/min, 95% CI; malignant 7.17 l/min SD +/- 1.80 l/min, delta esCCO 1.07 l/min, 95% CI [0.02; 2.12]; p=0.0483). As with stroke volume, the tumour group showed no significant changes under and after the puncture.
A summary of the relevant haemodynamic data is given in table 2.
Heart rate (bpm) and saturation (%): Heart rate and saturation were regular in all patients at baseline and follow-up. There were no exorbitant or significant changes in the patient´s pulse or saturation. There were no discernible effects in terms of gender and malignancy.
Summary: The apparent gender differences in haemodynamics were further investigated using a bootstrap model. We found that the apparent haemodynamic effects between the sexes were 78% likely to be due to the higher MELD score and not to sex. However, this calculation was not significant due to the small study size.
The Glimmex procedure was then used to estimate whether the pre-puncture MELD score could have influenced haemodynamics. It was found that with each additional MELD score, heart rate decreased by 0.84 and 1.05 beats per minute at 24 and 48 hours, respectively (p=0.03). In contrast, diastolic blood pressure tended to increase by 0.46 mmHg with each MELD score (p=0.13).
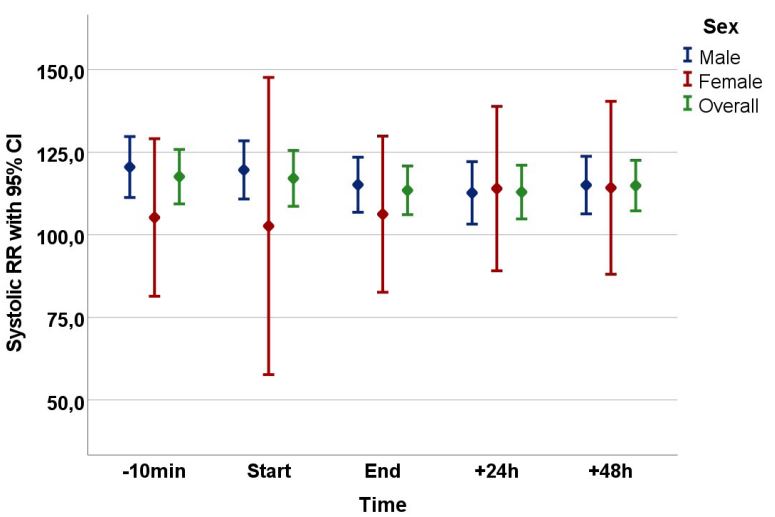
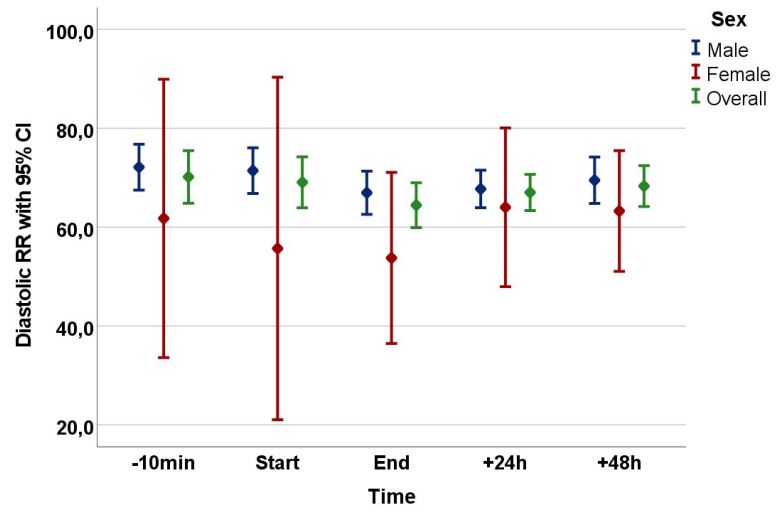
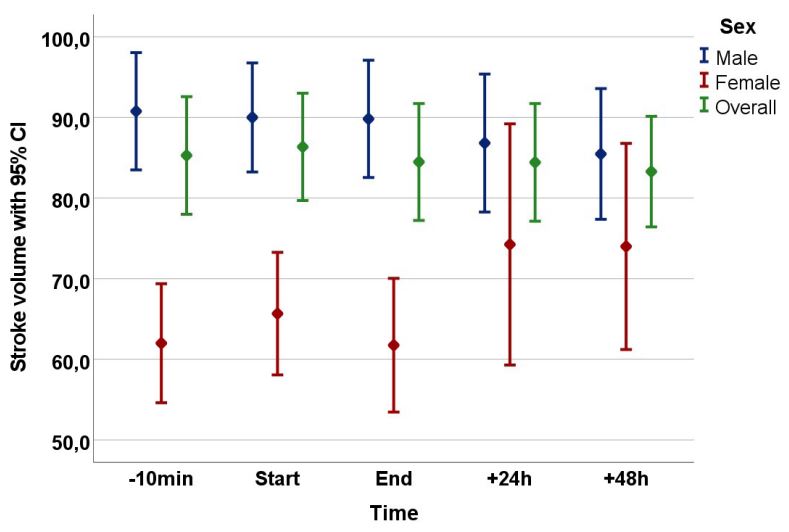
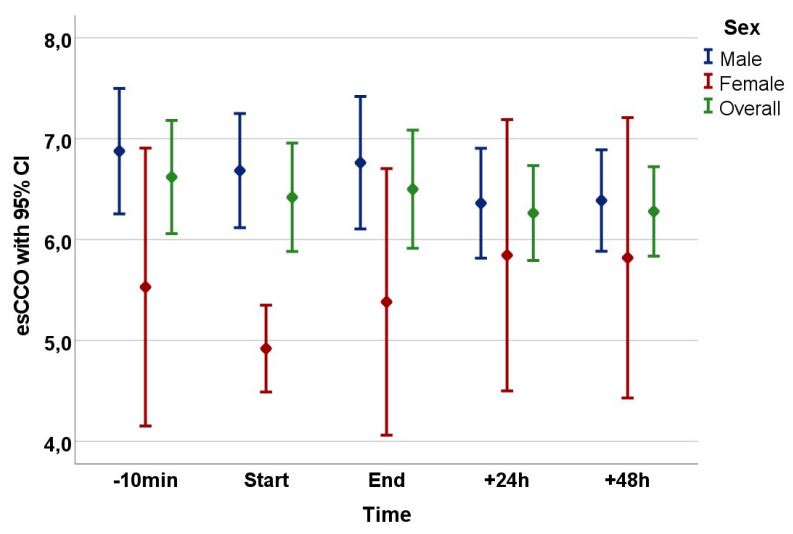
Table 1: Clinical and laboratory characteristics of the patients.
| Age (years) | 57.43 +/- 10.01 | ||
|---|---|---|---|
| Height (cm) | 173.10 +/- 7.99 | ||
| Weight (kg) | 86.46 +/- 14.86 | ||
| P Value | |||
| Gender | Male n = 17 (81%) |
Female n = 4 (11%) |
0.0017 |
| Age (years) | 58.35 +/-8.05 | 53.50+/- 17.25 |
0.6330 |
| Etiology of cirrhosis | |||
| Alcohol abuse (n) | 15 | 1 | 0.0173 |
| Virusinfection (n) | 3 | 0 | 1.000 |
| Others (n) | 2 | 3 | 0.0276 |
| Child-Turcotte-Pough-score (points) | 8 | 10 | 0.7429 |
| MELD Score (points) | 15.35 +/- 4.59 | 20 +/- 8.25 | 0.6352 |
| Malignancy (n) | 6 | 0 | 0.2807 |
| Liver (n) | 5 | 0 | 0.5322 |
| Extrahepatic (n) | 1 | 0 | 1.000 |
| SBP | 0 | 1 | 0.1905 |
| Other signs of infection | 1 | 0 | 1.000 |
| Drugs | |||
| Betablocker | 6 | 2 | 0.6177 |
| ACE-Inhibitor/Sartans | 1 | 1 | 0.3524 |
| Diuretics | 14 | 4 | 0.9621 |
| Aldosteron-Antagonists | 12 | 4 | 0.5322 |
| Nitrovasodilatator | 1 | 0 | 1.000 |
| Calcium-Antagonists | 2 | 0 | 1.000 |
| Statins | 2 | 3 | 0.0276 |
| PPI | 11 | 4 | 0.2871 |
| Others | 15 | 4 | 1.000 |
| Diseases | |||
| Diabetes mellitus | 6 | 1 | 1.000 |
| Arterial Hypertension | 7 | 1 | 1.000 |
| Cardial Insufficiency | 1 | 0 | 1.000 |
§ Note: Child-Turcotte-Pough-Score is represented as mean. Results are expressed as number of patients (n) or mean +/- standard devia- tion
Table 2: Summary of the haemodynamic data.
| Δ BP syst (mmHg) | Δ BP dia (mmHg) | Δ esSV (ml) | Δ esCCO (l/min/m2) | Δ esCI (l/min/m2) | |
|---|---|---|---|---|---|
| T0 – T End of puncture | |||||
| All patients | - 4.14 (p = 0.04) | - 5.71 (p = 0.001) | # | - 0.12 (p = 0.47) | - 0.16 (p = 0.05) |
| Male | - 5.35 + 1.0 (p = 0.031) $ |
# | # | # | # |
| Female | # | # | # | # | |
| T0 – T24h | |||||
| All patients | - 4.67 (p = 0.0085) | - 3.14 (p = 0.03) | # | - 0,36 (p = 0.0024) | - 0.17 (p = 0.03) |
| Male | -7.82 + 8.75 (p = 0.046) |
- 4.41 + 2.25 (p = 0.15) |
- 3.94 + 12.25 (p = 0.01) |
# | - 0.26 + 0.18 (p = 0.08) |
| Female | # | ||||
| T0 – T48h | |||||
| All patients | - 2.71 (p = 0.067) | - 1.86 (p = 0.09) | - 2.0 (p = 0.14) | - 0.34 (p = 0.037) | -0.17 (p = 0.05) |
| Male | - 5.47 + 9.0 (p = 0.10) |
# | - 5.29 + 12.0 (p = 0.03) |
# | # |
| Female | # | # | # |
$ Even before puncture, there was a significant difference between male and female patients in systolic and diastolic pressure (BP), Stroke Volume (esSV) and Cardiac Output (CO).
Discussion
In the present observational study, it could be illustrated that paracentesis in ascitic decompensated patients with liver cirrhosis resulted in partly pronounced changes in haemodynamics.
It was shown that the entire patient cohort experienced a significant reduction in systolic and diastolic blood pressure during the puncture. Surprisingly, it was also shown that within the patient cohort there were partly different haemodynamic changes under and after paracentesis.
To date, no study in the literature has continuously monitored haemodynamics under paracentesis. Previous studies have mainly focused on investigating Paracentesis-Induced Circulatory Dysfunction (PICD). However, it is also striking that in the previous data, there were sometimes inconsistent haemodynamic response patterns due to the intervention.
Haemodynamic changes under paracentesis were first described in the 1960s. Even in the first studies, partially contradictory data were found within the patient cohort, with a drop and rise in systolic blood pressure up to 48 h after intervention [30].
While in the work of Simon et al., no influence on mean arterial pressure could be found under fractionated ascites drainage, an increase in cardiac output was shown [31].
In contrast, a paper by Pozzi et al. found a reduction in mean arterial pressure, systemic resistance and an increase in stroke volume and cardiac output under continuous ascites drainage, which persisted after 24 hours [17].
In 1987, Gines et al. showed that the incidence of haemodynamic, renal and neurohumoral changes under paracentesis was significantly lower in a direct comparison between groups of patients who had received albumin substitution and patients without substitution, the increase in urea, plasma renin and plasma aldosterone 48 h after the procedure [20]. Even with albumin substitution, however, there was a significant decrease in mean arterial pressure under paracentesis.
In the work of Vila et al. 46 patients received ascites puncture [24]. Twenty patients developed effective hypovolaemia (neurohumoral activation with renin and aldosterone increase) on day 6 after intervention. However, a closer look at the data shows that the patients who showed an increase in renin and aldosterone (i.e., developed effective hypovolaemia with neurohumoral activation) showed a decrease in mean arterial pressure but a significant increase in cardiac output 3 and 6 hours after paracentesis. In contrast, the group of patients (n=26) who did not show neurohumoral changes also showed a slight decrease in MAP but also in cardiac output with an increase in systemic resistance. It should be mentioned that only 14 patients received albumin after paracentesis, the remaining patients received dextran 70 or polygeline.
Similar data could also be shown in the study by Nasr et al. [26]: 45 patients received blood tests before and after paracentesis and some of the patients also received transthoracic echocardiography before, 48 hours and six days after the procedure. Regardless of whether the patients had developed PICD, all patients showed a significant decrease in MAP 48 hours after paracentesis, with an increase in heart rate, ejection fraction and cardiac output.
Even though the present data are not directly comparable with our study in view of the study design, the research question and the patient characteristics, the results are similar:
Albumin substitution significantly reduces activation of the neurohumoral system and has since been recommended by numerous guidelines [32], but the haemodynamic effects of paracentesis seem independent of albumin administration. In our study, all patients received 8 g of albumin per litre of ascites removed and showed haemodynamic changes.
Most importantly, when looking at the subgroups of our patient cohort, we found that patients seemed to respond differently to the intervention.
It is known that with an increase in the severity of liver cirrhosis, the adaptive capacity of the circulation to stressors such as volume shifts, infections or even dobutamine administration decreases [33,34]. As the female patients in our study had a higher MELD score, we first checked whether the pre-puncture MELD score differed significantly between the sexes. This was not the case, although the number of cases was small.
Using a bootstrap model, we found that the apparent haemodynamic effects were 78% likely to be due to the higher MELD score of female patients and not per se to gender. However, this calculation was not significant due to the small study size.
We used the Glimmex procedure to estimate the haemodynamic effects of the MELD score before puncture. It was found that with each additional MELD score, heart rate decreased by 0.84 and 1.05 beats per minute at 24 and 48 hours, respectively (p=0.03). In contrast, diastolic blood pressure tended to increase by 0.46 mmHg with each MELD score (p=0.13).
It is known that with an increase in the severity of liver cirrhosis, there is also an increase in heart failure - cirrhotic cardiomyopathy - in the sense of first diastolic and then also systolic insufficiency [35,9]. The presence of ascites may worsen cardiac function due to upward displacement of the diaphragm, increased intrathoracic pressure, right atrial and right ventricular filling [36,37].
Although the amount of puncture was comparable concerning body surface area, the patients who tended to have higher MELD scores appeared to have improved diastolic filling. The observation of an influence of paracentesis on systolic function in patients with a lower MELD score has not been described so far.
It is also noteworthy that the patients with tumour disease in our analysis had significantly higher baseline systolic and diastolic blood pressure, but this was hardly affected by the intervention. Stroke volume and cardiac output also remained almost stable during treatment. Possible explanations for this observation could be that almost all patients with tumour disease had an average MELD score lower than the average of non-tumour patients (non-tumour 16.47 +/- 6.93 SD vs. tumour 15.67 +/-2.25 SD) and lower than the average of all patients of 16.24 +/- 5.91 SD. Since almost all patients had multifocal HCC, whether the tumour disease itself could have led to increased ascites formation should be considered.
Certainly, one of the major limitations of our study is the small sample size and high dimensionality of the data, which poses problems such as low statistical power of the analyses, inflated false discovery rate, inflated effect size estimate and low reproducibility. Although haemodynamic monitoring was only performed non-invasively in this study, similarities with previous results obtained with invasive procedures are comparable.
Despite our small study size, there are indications from our data that the haemodynamic changes change with increasing disease severity.
In order to analyse the described effects more precisely, a multicentre, interdisciplinary study involving, for example, hepatologists and cardiologists would be necessary to survey the different stages of liver cirrhosis more accurately. A longitudinal survey over a longer period of time, in which the interactions between the heart, circulation and liver are detected, would also be conceivable.
Conclusion
In summary, we could demonstrate in our observational study that patients with liver cirrhosis under paracentesis showed haemodynamic changes such as a decrease in systolic and diastolic blood pressure, mean arterial pressure, but also changes in stroke volume and cardiac output under but also after the intervention. The influence on systemic circulation parameters was partly detectable up to 48 hours after the puncture.
Abbreviations: SD: standard deviation; PAMPS: pathogen associated molecular patterns; NO: nitric oxide; Enos: endothelial nitric oxide synthase; LVP: endothelial nitric oxide synthase; PICD: paracentesis-induced circulatory dysfunction; PPSB: Prothrombin complex concentrate; PWTT: Pulse Wave Transit Time; ECG: Electrocardiogram; NIBP: Non-Invasive Blood Pressure; IBP: Invasive Blood Pressure; esCCO: estimated Continuous Cardiac Output; sv: stroke volume; EQ-5D: European Quality of life 5 dimensions; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; HCC: Hepatocellular Carcinoma.
Declarations
Data availability statement: The data are secured in pseudonymised electronic form and are available on request.
Conflict of interest disclosure: The authors declare that they have no conflict of interest regarding the content of this manuscript. IAJ received speakers’ fees from AstraZeneca outside the submitted work.
Funding statement: This research received no specific grant from any funding agency in the public, commercial, or not-forprofit sectors.
Acknowledgement: We would especially like to thank the study participants for their participation in the study and the provision of their measurement data. We would like to thank the company Nihon Kohden, Japan, for providing the measurement monitors esfree of charge.
We also thank Mrs Barbara Malik for her expert support in the preparation of the laboratory samples.
Clinical trial registration: ClinicalTrials.gov Identifier: NCT02799160
Ethics approval statement: Study investigation was approved by the Ethics Committee of Charité, Universitatsmedizin Berlin (EA2/052/16).
Patient consent statement: Each study participant received written information about the study project and provided written informed consent.
References
- Wiest R, Lawson M, Geuking M. Pathological bacterial translocation in liver cirrhosis. J Hepatol. 2014; 60(1): 197-209.
- Bernardi M, Moreau R, Angeli P, Schnabl B, Arroyo V. Mechanisms of decompensation and organ failure in cirrhosis: From peripheral arterial vasodilation to systemic inflammation hypothesis. J Hepatol. 2015; 63(5): 1272-84.
- Arroyo V, Angeli P, Moreau R, Jalan R, Clària J, et al. The systemic inflammation hypothesis: Towards a new paradigm of acute decompensation and multiorgan failure in cirrhosis. J Hepatol. 2021; 74(3):670-85.
- Iwakiri Y, Kim MY. Nitric oxide in liver diseases. Trends Pharmacol Sci. 2015; 36(8): 524-36.
- 4. Bellot P, Francés R, Such J. Pathological bacterial translocation in cirrhosis: Pathophysiology, diagnosis and clinical implications. Liver Int. 2013; 33(1): 31-9.
- Dimmeler S, Fleming I, Fisslthaler B, Hermann C, Busse R, et al. Activation of nitric oxide synthase in endothelial cells by Aktdependent phosphorylation. Nature. 1999; 399(6736): 601-5.
- Wiest R, Cadelina G, Milstien S, McCuskey RS, Garcia-Tsao G, Groszmann RJ. Bacterial translocation up-regulates GTP-cyclohydrolase I in mesenteric vasculature of cirrhotic rats. Hepatol. 2003; 38(6): 1508-15.
- Ruiz-del-Arbol L, Monescillo A, Arocena C, Valer P, Ginès P, et al. Circulatory function and hepatorenal syndrome in cirrhosis. Hepatol. 2005; 42(2): 439-47.
- Kazankov K, Holland-Fischer P, Andersen NH, Torp P, Sloth E, et al. Resting myocardial dysfunction in cirrhosis quantified by tissue Doppler imaging. Liver Int. 2011; 31(4): 534-40.
- Ruíz-del-Árbol L, Achécar L, Serradilla R, Rodríguez-Gandía MÁ, Rivero M, et al. Diastolic dysfunction is a predictor of poor outcomes in patients with cirrhosis, portal hypertension, and a normal creatinine. Hepatol. 2013; 58(5): 1732-41.
- Praktiknjo M, Monteiro S, Grandt J, Kimer N, Madsen JL, et al. Cardiodynamic state is associated with systemic inflammation and fatal acute-on-chronic liver failure. Liver Int. 2020; 40(6): 1457-66.
- Yotti R, Ripoll C, Benito Y, Catalina MV, Elízaga J, et al. Left ventricular systolic function is associated with sympathetic nervous activity and markers of inflammation in cirrhosis. Hepatol. 2017; 65(6): 2019-30.
- Pache I, Bilodeau M. Severe haemorrhage following abdominal paracentesis for ascites in patients with liver disease. Aliment Pharmacol Ther. 2005; 21(5): 525-9.
- Knauer CM, Lowe HM. Hemodynamics in the cirrhotic patient during paracentesis. N Engl J Med. 1967; 276(9): 491-6.
- Shear L, Ching S, Gabuzda GJ. Compartmentalization of ascites and edema in patients with hepatic cirrhosis. N Engl J Med. 1970; 282(25): 1391-6.
- Hecker R, Sherlock S. Electrolyte and circulatory changes in terminal liver failure. Lancet. 1956; 271(6953): 1121-5.
- Pozzi M, Osculati G, Boari G, Serboli P, Colombo P, et al. Time course of circulatory and humoral effects of rapid total paracentesis in cirrhotic patients with tense, refractory ascites. Gastroenterol. 1994; 106(3): 709-19.
- Luca A, Cirera I, García-Pagán JC, Feu F, Pizcueta P, et al. Hemodynamic effects of acute changes in intra-abdominal pressure in patients with cirrhosis. Gastroenterol. 1993; 104(1): 222-7.
- Cabrera J, Falcón L, Gorriz E, Pardo MD, Granados R, et al. Abdominal decompression plays a major role in early postparacentesis haemodynamic changes in cirrhotic patients with tense ascites. Gut. 2001; 48(3): 384-9.
- Ginès P, Titó L, Arroyo V, Planas R, Panés J, et al. Randomized comparative study of therapeutic paracentesis with and without intravenous albumin in cirrhosis. Gastroenterol. 1988; 94(6): 1493-502.
- Ruiz-del-Arbol L, Monescillo A, Jimenéz W, Garcia-Plaza A, Arroyo V, et al. Paracentesis-induced circulatory dysfunction: mechanism and effect on hepatic hemodynamics in cirrhosis. Gastroenterol. 1997; 113(2): 579-86.
- Ginès A, Fernández-Esparrach G, Monescillo A, Vila C, Domènech E, et al. Randomized trial comparing albumin, dextran 70, and polygeline in cirrhotic patients with ascites treated by paracentesis. Gastroenterol. 1996; 111(4): 1002-10.
- Bernardi M, Caraceni P, Navickis RJ, Wilkes MM. Albumin infusion in patients undergoing large-volume paracentesis: A metaanalysis of randomized trials. Hepatol. 2012; 55(4): 1172-81.
- Vila MC, Solà R, Molina L, Andreu M, Coll S, et al. Hemodynamic changes in patients developing effective hypovolemia after total paracentesis. J Hepatol. 1998; 28(4): 639-45.
- Sola-Vera J, Such J. Understanding the mechanisms of paracentesis-induced crculatory dysfunction. Eur J Gastroenterol Hepatol. 2004; 16(3): 295-8.
- Nasr G, Hassan A, Ahmed S, Serwah A. Predictors of large volume paracantesis induced circulatory dysfunction in patients with massive hepatic ascites. J Cardiovasc Dis Res. 2010; 1(3): 136-44.
- Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, et al. Hepatic encephalopathy-definition, nomenclature, diagnosis, and quantification: Final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatol. 2002; 35(3): 716-21.
- EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J Hepatol. 2010; 53(3): 397-417.
- Ishihara H, Okawa H, Tanabe K, Tsubo T, Sugo Y, et al. A new noninvasive continuous cardiac output trend solely utilizing routine cardiovascular monitors. J Clin Monit Comput. 2004; 18(5-6): 313-20.
- Kao HW, Rakov NE, Savage E, Reynolds TB. The effect of large volume paracentesis on plasma volume-a cause of hypovolemia? Hepatol. 1985; 5(3): 403-7.
- Simon DM, McCain JR, Bonkovsky HL, Wells JO, Hartle DK, et al. Effects of therapeutic paracentesis on systemic and hepatic hemodynamics and on renal and hormonal function. Hepatol. 1987; 7(3): 423-9.
- Paolo Angeli, Mauro Bernardi, Càndid Villanueva, Claire Francoz, Rajeshwar P. Mookerjee, Jonel Trebicka et al. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018; 69(2): 406-60.
- Naqvi IH, Mahmood K, Naeem M, Vashwani AS, Ziaullah S. The heart matters when the liver shatters! Cirrhotic cardiomyopathy: Frequency, comparison, and correlation with severity of disease. Prz Gastroenterol. 2016; 11(4): 247-56.
- Gassanov N, Caglayan E, Semmo N, Massenkeil G, Er F. Cirrhotic cardiomyopathy: A cardiologist’s perspective. World J Gastroenterol. 2014; 20(42): 15492-8.
- Møller S, Henriksen JH. Cardiovascular dysfunction in cirrhosis. Pathophysiological evidence of a cirrhotic cardiomyopathy. Scand J Gastroenterol. 2001; 36(8): 785-94.
- Guazzi M, Polese A, Magrini F, Fiorentini C, Olivari MT. Negative influences of ascites on the cardiac function of cirrhotic patients. Am J Med. 1975; 59(2): 165-70.
- Karasu Z, Mindikoğlu AL, van Thiel DH. Cardiovascular problems in cirrhotic patients. Turk J Gastroenterol. 2004; 15(3): 126-32.