
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Defecation disorders in patients following definitive surgery for Hirschsprung’s disease: A tertiary care hospital study
Posam Manoj Kumar1*; Philpose Rashmi Tresa2; Gowni Ashrith Reddy3
1Department of Pediatric Surgery, Niloufer Institute for Women and Child Health, Hyderabad, Telangana, India.
2Department of Pathology, Osmania Medical College, Hyderabad, Telangana, India.
3Department of Pediatric Surgery, Niloufer Institute for Women and Child Health, Hyderabad, Telangana, India.
*Corresponding Author : Posam Manoj Kumar
Department of Pediatric surgey, Niloufer Hospital, Red
Hills, Hyderabad, Telangana, India.
Tel: +919703689469;
Email: manojtheps@gmail.com
Received : Apr 11, 2024
Accepted : May 01, 2024
Published : May 08, 2024
Archived : www.jjgastro.com
Copyright : © Kumar PM (2024).
Abstract
Background: Hirschsprung’s Disease (HD) poses a common challenge in pediatric surgery, often leading to congenital intestinal obstruction. Despite advancements in surgical techniques, postoperative Defecation Disorders (DDs) significantly impact the well-being of affected children. This study investigates the clinical manifestation, management, and outcomes of DDs in children after definitive surgery for HD, utilizing a comprehensive systematic algorithm.
Methods: 50 children with postoperative HD-related DDs were studied over a five-year period.
A systematic algorithm categorized them based on mechanical obstruction or obstructive symptoms. Management strategies, ranging from conservative measures to surgical interventions, were employed. Final diagnoses were determined through diagnostic testing and management response. Clinical outcomes were classified as poor, fair, good, or excellent. Statistical analyses utilized SPSS software.
Results: Chronic constipation was the predominant presentation (36%), with modified Duhamel’s pull-through being the most common surgery (74%). Diagnostic studies revealed diverse findings on contrast enema. Various revision surgeries were performed based on clinical scenarios. Final diagnoses included non-retentive fecal incontinence (28%), non-intractable constipation (24%), enterocolitis (20%), and others. Follow-up periods ranged from 4 months to more than 24 months. Functional outcomes showed good results in 54% of cases, fair in 30%, poor in 12%, and excellent in 4%
Conclusion: This study emphasizes the significance of a systematic algorithm in managing DDs in postoperative HD, providing insights into diverse diagnoses and interventions. Achieving favorable long-term outcomes for the majority of cases highlights the potential of tailored strategies. Further research and comparative studies are essential for refining treatment approaches and enhancing the quality of life for these children.
Keywords: Hirschsprung’s disease; Defecation disorders; Modified Duhamel’s pull-through; Anorectal manometry; constipation; Enterocolitis.
Abbreviations: HD: Hirschsprung Disease; DD: Defecation Disorder; DS: Definitive Surgery; RAIR: Recto-Anal Inhibitory Reflex; TERPT: Transanal Endorectal PullThrough; OS: Obstructive Symptoms; IAS: Internal Anal Sphincter.
Citation: Kumar PM, Tresa PR, Reddy GA. Defecation disorders in patients following definitive surgery for Hirschsprung’s disease: A tertiary care hospital study. J Gastroenterol Res Pract. 2024; 4(5): 1198.
Introduction
Hirschsprung’s Disease (HD), one of the most common cause of congenital intestinal obstruction in children. It is a neural crest disorder characterized by aganglionosis, beginning in the rectum, and extending to different lengths proximally. It occurs in approximately 1 in 5000 to 10,000 live births [1,2]. Inspite of introduction of techniques like laparoscopic and transanal 60% of children with HD experience Defecation Disorder (DD) and/ or enterocolitis after initial HD Definitive Surgery (DS) [3]. These DDs encountered include constipation, fecal incontinence, occasionally associated with abdominal distention, emesis, and/or enterocolitis [4,5]. Enterocolitis postoperatively increases morbidity and hospitalizations, sometimes leading to higher mortality rates, emphasizing the importance of timely recognition and management [6]. In late adolescence, full bowel continence and symptom resolution post-surgery are common but not guaranteed, presenting significant challenges for both the child and their family, necessitating comprehensive support [7,8].
A range of diagnostic and therapeutic methods, encompassing radiological, manometric, dietary, pharmaceutical, and surgical interventions, have been proposed to address Defecation Disorders (DDs) and enterocolitis subsequent to Hirschsprung’s disease surgery in children. These strategies are directed towards assessing and alleviating postoperative complications, particularly fecal incontinence, in this pediatric population [9].
Despite this, there hasn’t been a complete evaluation of a systematic algorithm that integrates various strategies and examines its effects on clinical outcomes in children with postoperative Defecation Disorders (DDs). This study investigates defecation disorders post Hirschsprung’s disease surgery in children, focusing on incidence, clinical aspects, and management. Its goal is to enhance treatment using a diagnostic protocol and management strategies to improve outcomes and children’s quality of life.
Material and methods
The study was conducted at Niloufer hospital for women and children in the Department of Pediatric Surgery, after approval from the ethics committee in compliance with ethical standards of the committee. 50 patients having defecation disorders post definitive surgery for Hirschsprung’s disease between January 2018 and December 2022 were reviewed in this study
All children from birth to 14 years of age, with documented follow-up of Hirschsprung’s disease post definitive procedure, who presented to our institute were included in the study. Children with abnormal motility disorders and other associated anomalies except HD causing defecation disorders were excluded from this study. After conducting an initial assessment, including medical history, physical examination, and radiological evaluation, children were divided into two groups according to the study conducted by Chumpitazi et al. (2011) [10].
Group 1 were children with evidence of mechanical obstruction (anal stenosis and stricture) or a transition zone, who were directly taken up for anal dilatation or revision surgery.
Group 2 were children with Obstructive Symptoms (OS) (like constipation, straining while defecating) abdominal distention or enterocolitis, and non-retentive fecal incontinence based on contrast enema findings and clinical examination findings.
(Non-retentive fecal incontinence is the diagnosis applied to children with a developmental age of at least 4 years, who have bowel movements in places and at inappropriate times, at least once a month for at least 2 months, in the absence of disease to explain it, and without signs of fecal retention).
Children exhibiting obstructive symptoms were commenced on a rigorous bowel regimen, whereas those presenting with non-retentive fecal incontinence were initiated on fiber supplementation to regulate colonic transit. Children with abdominal distention and/or recurrent enterocolitis after evaluation were initially managed conservatively with IV antibiotics and were later followed up. These children were closely followed up for 3 months and reassessed as shown in Figure 1. Another diagnostic and therapeutic protocol was followed for children who were unresponsive to the initial management for at least 3 months as shown in Figure 2. In patients with abdominal distention causing discomfort despite the use of an aggressive oral laxative regimen, rectal therapies (like bisacodyl suppositories and normal saline irrigations or enemas) were recommended.
Children without improvement were considered for Anorectal manometry to rule out internal sphincter achalasia who have absent RAIR (Rectoanal Inhibitory Reflex) and other issues like rectal sensation and compliance. If symptoms continue to persist with abnormal manometry findings, internal sphincter myectomy is performed. (The main physiological prerequisites for fecal continence included, preserved sphincter function, rectal reservoir, and anal canal sensation), Trans anal rectal biopsy was done in children who do not improve and children with improvement were followed up to assess the outcome. Children with acquired aganglionosis were considered for repeat pullthrough. Children who improved were closely followed up to assess the outcome, children without any improvement finally were labeled to have intestinal dysmotility.
Treatment
Treatment was based on the clinical course and diagnostic findings. Laxatives like senna and bisacodyl were used. When patients had less than 2 bowel movements per week and/or experienced discomfort due to abdominal distention despite aggressive oral laxative treatment, rectal therapies were recommended which included, normal saline irrigations and bisacodyl suppositories.
The diagnosis responsible for the symptoms were determined based on the outcomes of diagnostic testing and the response to management. Children whose obstructive symptoms notably improved (such as the absence of constipation or fecal incontinence episodes related to stool retention) following an initial bowel regimen were classified as having non-intractable constipation. The final diagnosis for children undergoing a surgical procedure was determined according to the indication for the procedure (eg, acquired aganglionosis). Children with nonretentive fecal incontinence received a final diagnosis reflecting the cause of the incontinence (e.g., food intolerance).
Assessment of clinical outcomes
Based on study conducted by Chumpitazi et al. (2011), clinical outcomes were determined based on symptom severity and management needed at the time of the last follow-up [10].
Poor: No improvement or worsening in the number of bowel movements or an enterocolitis episode within 3 months of the last documented follow-up.
Fair: Improvement in the number of bowel movements with a need for rectal therapies (eg, enema, suppository, irrigation), fecal incontinence episodes more than once per week, or an enterocolitis episode between 3 to 6 months of the last documented follow-up.
Good: Improvement in the number of bowel movements with continued usage of oral laxatives, fecal incontinence episodes less than once per week, or an enterocolitis episode between 6 to 12 months of the last documented follow-up.
Excellent: Improvement in the number of bowel movements or other obstructive symptoms without the need for medications, elimination of all fecal incontinence episodes, or last enterocolitis episode more than 1 year from the last documented follow-up.
Statistical analysis
Mean values are presented with standard error, and percentages are rounded to the nearest decimal point. χ2 analysis was utilized to compare categorical variables across groups. Longterm outcomes were deemed favorable if rated as excellent or good. Statistical analysis was conducted using SPSS software (SPSS Inc, Chicago, IL).
Results
A total of 50 children were studied. There were 38(76%) males and 12(24%) females. The median age was 3.64+2.27 years. With majority of cases seen in the age group of 1 to 4 years 32/50 (64%).
The predominant presentation was chronic constipation, evident in 18(36%) of the children. Fecal soiling was observed in 15(30%), while 8(16%) exhibited foul-smelling loose stools along with abdominal distention. Bilious vomiting and abdominal distension were seen in 5(10%), and 4(8%) experienced foulsmelling loose stools coupled with perianal excoriation.
The modified Duhamel’s pull-through procedure was performed in 37 cases, constituting 74% of the surgeries. The transanal endorectal pull-through method was utilized in 13 cases, representing 26% of the procedures.
In the diagnostic studies involving contrast enema, various findings were observed. The most prevalent was the absence of anatomical etiology, noted in 23 cases (65.7%). Colonic dilatation was identified in 5 cases (14.2%), while residual spur was observed in 3 cases (8.6%). Additionally, 3 cases (8.6%) exhibited a combination of colonic dilatation with anal stenosis. A transition zone was identified in 1 case (2.8%). These findings provide valuable insights into the diverse anatomical considerations in the studied cases as shown in Table 1.
Treatment
The revision surgeries performed in response to specific clinical scenarios were diverse in nature across the studied cases. The most common approach, observed in 36 cases, accounted for 72% of the procedures and involved a conservative strategy. Additionally, the division of residual spur, anal dilatation, and laparotomy with adhesiolysis were each performed in 3 cases, constituting 6% of the cases for each procedure. More extensive interventions, such as laparotomy combined with adhesiolysis and ileostomy, were undertaken in 2 cases, representing 4% of the total. Internal sphincter myectomy was performed in 2 cases (4%). Endorectal pull-through was conducted in 1 case (2%).
The final diagnosis responsible for the presenting symptoms were diverse, with non-retentive fecal incontinence being the most prevalent at 14(28%), followed by non-intractable constipation in 12(24%) and enterocolitis in 10(20%). Intestinal obstruction (IO) was identified in 5(10%) of cases, while anal stenosis and residual spur each accounted for3 cases each (6%) respectively. Internal sphincter achalasia was diagnosed in 2(4%) of cases, and acquired aganglionosis was the least common seen in 1cases (2%).
The findings on trans anal rectal biopsy revealed two main categories: Presence of ganglion cells: Observed in 11 cases, constituting 92% of the biopsies and Absence of ganglion cells: Detected in 1 case, representing 8% of the biopsies. As shown in Table 2.
Follow up
A total of 25(50%) of cases had a follow-up period ranging from 4 to 10 months, while 20(40%) were observed within the 11-17 months range. A smaller percentage of cases, 3(6%), had a followup period spanning 18 to 24 months. Additionally, 2 (4%) of cases had an extended follow-up period exceeding 24 months.
Functional outcome
Overall 27 cases (54%) had good outcome, 15 cases (30%) had fair outcome, 6 cases (12%) showed poor outcome and excellent outcome was seen in 2 cases (4%) For children aged 1-4 years, 4(14.3%) experienced poor outcomes, 9(32.1%) had fair outcomes, and the majority, 15(53.6%), achieved good/excellent outcomes. Similarly, in the 5-9 years age group, 2(9.1%) faced poor outcomes, 6(27.3%) had fair outcomes, and a significant 14(63.6%) achieved good/excellent outcomes. The overall distribution across all age groups reveals that 6(12%) experienced poor outcomes, 15(30%) had fair outcomes, and the majority, 29(58%) achieved good/excellent outcomes. With a p-value of 0.70 and a chi-square (χ2 ) value of 0.59, along with 2 degrees of freedom (df), the analysis indicates no statistically significant association between age groups as shown in table.
Among males, 4(10.3%) experienced poor outcomes, 14(35.9%) had fair outcomes, and the majority, 21(53.8%), achieved good/excellent outcomes. Whereas among females 2(%) had poor outcome, 1(%) had fair outcome and 8(72.7%) had good/excellent outcomes. With a p-value of 0.20 and a chisquare (χ2 ) value of 3.03, along with 2 degrees of freedom (df), the analysis indicates a lack of statistically significant association between gender (male and female) and the observed outcomes categorized as poor, fair, or good/excellent.
Evaluating the distribution, for those who underwent modified Duhamel’s pull-through, 5(13.5%) experienced poor outcomes, 12(32.5%) had fair outcomes, and the majority, 20(54%), achieved good/excellent outcomes. In contrast, among those who had transanal endorectal pull-through, 1(7.7%) had poor outcomes, 3(23.1%) had fair outcomes, and a significant 9(69.2%) achieved good/excellent outcomes. With a p-value of 0.60 and a chi-square (χ2 ) value of 0.93, along with 2 degrees of freedom (df), the analysis suggests no statistically significant association between the initial surgical procedure and the observed outcomes categorized as poor, fair, or good/excellent as shown in Table 3.
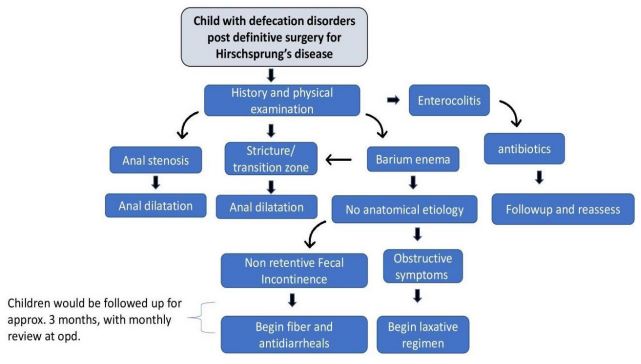
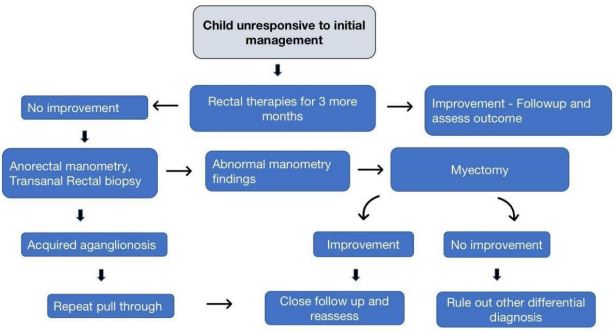
Table 1: Distribution of study subjects based on findings of contrast enema (n=34).
| S.no | Findings on contrast enema | Frequency (n) | Percentage |
|---|---|---|---|
| 1 | No anatomical etiology | 23 | 65.7% |
| 2 | Colonic dilatation | 5 | 14.2% |
| 3 | Residual spur | 3 | 8.6% |
| 4 | Colonic dilatation with anal stenosis | 3 | 8.6% |
| 5 | Transition zone | 1 | 2.8% |
| Total | 35 | 100% |
Table 2: Distribution of study subjects based on final diagnosis responsible for the symptom (n=50).
| S.no | Final diagnosis responsible for the symptom |
Frequency (n) | Percentage |
|---|---|---|---|
| 1 | Non retentive fecal incontinence | 14 | 28% |
| 2 | Non intractable constipation | 12 | 24% |
| 3 | Enterocolitis | 10 | 20% |
| 4 | Intestinal obstruction | 5 | 10% |
| 5 | Anal stenosis | 3 | 6% |
| 6 | Residual spur | 3 | 6% |
| 7 | Internal sphincter achalasia | 2 | 4% |
| 8 | Acquired aganglionosis | 1 | 2% |
| Total | 50 | 100% |
Table 3: Association between age, gender, initial surgical procedure and outcome of disease.
| Categories | Outcome of disease | Total | P value, χ2 | ||
|---|---|---|---|---|---|
| Poor | Fair | Good and Excellent | |||
| Age(years) | |||||
| 1-4 | 4(14.3%) | 9(32.1%) | 15(53.6%) | 28(100%) | p value=0.7 χ2=0.59 DF=2 |
| 5-9 | 2(9.1%) | 6(27.3%) | 14(63.6%) | 22(100%) | |
| Male | 4(10.3%) | 14(35.9%) | 21(53.8%) | 50(100%) | p value=0.2 χ2=3.03 DF=2 |
| Female | 2 | 1 | 8(72.7%) | 11(100%) | |
| Modified duhamels pull through | 5(13.5%) | 12(32.5%) | 20(54%) | 37(100%) | p value=0.6 χ2=0.93 DF=2 |
| Transanal endorectal pull through | 1(7.7%) | 3(23.1%) | 9(69.2%) | 13(100%) | |
Discussion
Our study evaluates functional outcomes, diagnosis and management approach, following a comprehensive systematic protocol addressing all defecation disorders in children with HD after DS. The outcome in comparison with age and sex was statistically not significant (p-value 0.7 and 0.2 respectively) as age distribution and sex distribution among the cohort varied. Similarly, the outcome with the type of initial surgical procedure was statistically insignificant (p-value - 0.6) as 37 children included in this study underwent modified Duhamel’s pull-through, while the remaining 13 underwent transanal endorectal pull-through.
Most of the children in this study had fecal incontinence (28%), and constipation (24%) followed by enterocolitis (20%) who were all managed conservatively with the help of a systematically prepared algorithm. Previous researchers have noted that the likelihood of needing surgical intervention after the initial pull-through Duhamel procedure for Hirschsprung’s Disease (HD) may be relatively high, with estimates ranging from 26% to 34% [11,12]. Surgical management was needed in 28% of our population. This might be attributed partially to the diverse nature of referral patients at our center.
Individuals who have undergone surgical treatment for Hirschsprung’s Disease (HD) may face a higher likelihood of experiencing Defecation Disorders (DDs) due to factors such as the development of a postsurgical neorectum with diminished sensation and capacity for accommodation, persistent nonrelaxation of the Internal Anal Sphincter (IAS), and an increased propensity for colonic dysmotility [13-15]. In spite of these acknowledged challenges, some children experiencing Obstructive Symptoms (OS) and/or enterocolitis responded favorably to an intensive regimen of oral laxatives alone. This suggests that children who have undergone surgery for Hirschsprung’s Disease (HD) may develop a propensity to avoid defecation due to past trauma or discomfort, resembling the behavior seen in children with functional constipation [16].
Children with Hirschsprung’s Disease (HD) experience a nonrelaxing Internal Anal Sphincter (IAS), which leads to functional obstruction. Some authors have attributed symptoms to this functional obstruction, particularly after observing improvement following local Botox injection therapy [17]. In our center, we preferred internal anal sphincter myectomy, as with Botox injection, the rate of transient fecal incontinence, non-response, and subsequent surgical procedures were significantly higher compared to IAS myectomy [18].
Given that the algorithm was followed in the entire studied cohort in a manner consistent with daily clinical care, we hope that this model will serve as an early step toward further work in comparative effectiveness in the care of these children. This stepwise protocol is generalizable and can be followed in the majority of medical centers that treat children with HD. Evaluation of the child’s anatomy followed by appropriate categorization into obstructive or nonretentive symptoms will lead to appropriate management. Referral to another institution will vary depending on the availability of therapies such as anal sphincter Botox, or the need for anorectal manometry evaluation. In our study, only a minority of patients underwent anorectal manometry (4%). As such, only a small number of patients needed to be referred for this evaluation using the algorithm.
In our study, 14 children had nonretentive fecal incontinence after a detailed evaluation, which included history (subjective to the child’s parents), physical examination, contrast enema, and a per rectal examination to evaluate the integrity of the anal canal. Thirteen children (92.8%) had good anal sphincter tone with no anatomical etiology on contrast enema, one child (7.2%) had mildly decreased anal sphincter tone on per rectal examination, colonic dilatation on contrast enema and low anal resting pressures on anorectal manometry. All thirteen children were able to achieve continence with conservative management and had good to excellent long-term outcomes, who were actually pseudo-incontinent in retrospect. However, the other child was determined to be truly incontinent, with relatively poor outcome on long-term follow-up.
The existing literature lacks clarity regarding which surgical procedure for Hirschsprung’s Disease (HD) yields optimal outcomes in bowel control, and it appears that there is no correlation between the occurrence of fecal incontinence and the type of initial procedure performed. Teitelbaum et al (2003) reported good to excellent continence in children undergoing a primary endorectal pullthrough for HD [19]. Langer et al (2010) reported that 19% of patients who underwent an endorectal procedure had some form of postoperative fecal incontinence [20]. In our study, only one child among fourteen children with nonretentive fecal incontinence had a TERPT procedure done.
While TERPT is considered a valuable maneuver, it can occasionally prompt surgeons to initiate dissection at a lower level, potentially resulting in excessive stretching through retraction to achieve visualization, which may inadvertently damage the anal canal. Yan et al (2019) reported that TERPT is superior to Transabdominal (TAB) approach in terms of hospitalization time, postoperative incontinence, and constipation [21]. Tian et al (2022) proposed the principle of “anorectal balance” where botulinum toxin injection and internal anal sphincter myectomy were used to treat postoperative intestinal dysfunction in children with HD [22]. Nonetheless, the genuine morbidity associated with various types of operations remains uncertain, and this article does not provide conclusive evidence linking any specific procedure to increased rates of fecal incontinence.
Limitations
The main limitation of the study is its restricted timeframe, which spans only five years. Variables such as follow-up intervals and adherence to prescribed medication regimens were not taken into consideration. Moreover, symptom improvement was subjectively assessed based on historical data documented by the primary pediatric surgeon. Additionally, another limitation of the current study is lack of incorporation of numerous diagnostic techniques and interventions being a tertiary care hospital.
Conclusion
Defecation issues following surgery in children with Hirschsprung’s Disease (HD) are prevalent and have a detrimental effect on the patient’s quality of life, leading to notable morbidity. A systematic and prompt evaluation is crucial to rule out anatomical and pathological factors contributing to fecal incontinence and obstructive symptoms. Subsequently, a functional assessment of the anorectum can be conducted to identify abnormalities in neuromuscular function. The outcomes of this study propose that employing a thorough systematic protocol for persistent defecation disorders in children postoperative for Hirschsprung’s disease could pinpoint diagnoses requiring tailored treatments, ultimately yielding positive long-term results.
Declarations
Conflicts of interest: None.
Funding sources: None.
Acknowledgements: None.
References
- Iwashita T, Kruger GM, Pardal R, et al. Hirschsprung disease is linked to defects in neural crest stem cell function. Science. 2003; 301: 972-6.
- Russell MB, Russell CA, Niebuhr E. An epidemiological study of Hirschsprung’s disease and additional anomalies. Acta Paediatr. 1994; 83: 68-71.
- Georgeson KE, Robertson DJ. Laparoscopic-assisted approaches for the definitive surgery for Hirschsprung’s disease. Semin Pediatr Surg. 2004; 13: 256-62.
- Catto-Smith AG, Coffey CM, Nolan TM, et al. Fecal incontinence after the surgical treatment of Hirschsprung disease. J Pediatr. 1995; 127: 954-7.
- Hyman PE. Defecation disorders after surgery for Hirschsprung’s disease. J Pediatr Gastroenterol Nutr. 2005; 41(Suppl 1): S62-3.
- Menezes M, Puri P. Long-term outcome of patients with enterocolitis complicating Hirschsprung’s disease. Pediatr Surg Int. 2006; 22: 316-8.
- Bax KN. Duhamel Lecture: the incurability of Hirschsprung’s disease. Eur J Pediatr Surg. 2006; 16: 380-4.
- Yanchar NL, Soucy P. Long-term outcome after Hirschsprung’s disease: patients’ perspectives. J Pediatr Surg. 1999; 34: 1152-60.
- Levitt MA, Martin CA, Olesevich M, et al. Hirschsprung disease and fecal incontinence: diagnostic and management strategies. J Pediatr Surg. 2009; 44: 271-7.
- Chumpitazi BP, Nurko S. Defecation disorders in children after surgery for Hirschsprung disease. J Pediatr Gastroenterol Nutr. 2011; 53(1): 75-9. doi: 10.1097/MPG.0b013e318212eb53. PMID: 21694540.
- Fortuna RS, Weber TR, Tracy TF, et al. Critical analysis of the operative treatment of Hirschsprung’s disease. Arch Surg. 1996; 131: 524-5.
- Weber TR, Fortuna RS, Silen ML, et al. Reoperation for Hirschsprung’s disease. J Pediatr Surg. 1999; 34: 153-7.
- Chumpitazi BP, Fishman SJ, Nurko S. Long-term clinical outcome after botulinum toxin injection in children with nonrelaxing internal anal sphincter. Am J Gastroenterol. 2009; 104: 976-83.
- Di Lorenzo C, Solzi GF, Flores AF, et al. Colonic motility after surgery for Hirschsprung’s disease. Am J Gastroenterol. 2000; 95: 1759-64.
- Pensabene L, Youssef NN, Griffifiths JM, et al. Colonic manometry in children with defecatory disorders. Role in diagnosis and management. Am J Gastroenterol. 2003; 98: 1052-7.
- Hyman PE. Defecation disorders after surgery for Hirschsprung’s disease. J Pediatr Gastroenterol Nutr. 2005; 41(Suppl 1): S62-3.
- Minkes RK, Langer JC. A prospective study of botulinum toxin for internal anal sphincter hypertonicity in children with Hirschsprung’s disease. J Pediatr Surg. 2000; 35: 1733-6.
- Friedmacher F, Puri P. Comparison of posterior internal anal sphincter myectomy and intrasphincteric botulinum toxin injection for the treatment of internal anal sphincter achalasia: a meta-analysis. Pediatr Surg Int. 2012; 28(8): 765-71.
- Teitelbaum DH, Coran AG. Primary pull-through for Hirschsprung’s disease. Semin Neonatol. 2003; 8(3): 233-41. doi: 10.1016/S1084-2756(03)00026-5.
- Kim AC, Langer JC, Pastor AC, Zhang L, Sloots CE, et al. Endorectal pull-through for Hirschsprung’s disease-a multicenter, long-term comparison of results: transanal vs transabdominal approach. J Pediatr Surg. 2010; 45(6): 1213-20. doi: 10.1016/j.jpedsurg.2010.02.087.
- Yan BL, Bi LW, Yang QY, Wu XS, Cui HL. Transanal endorectal pull-through procedure versus transabdominal surgery for Hirschsprung disease: A systematic review and metaanalysis. Medicine (Baltimore). 2019; 98(32): e16777. doi: 10.1097/MD.0000000000016777.
- Tian L, Ma C, Deng Z, Zhu T, Zhao X, et al. Treatment of postoperative intestinal dysfunction of hirschsprung’s disease based on the principle of “anorectal balance”. Front. Surg. 2022; 9: 996455. doi: 10.3389/fsurg.2022.996455.