
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Eating disorder symptoms and diagnoses in adults with celiac disease
Janet E Schebendach1; Anne R Lee2; Yara Gholmie3; Randi Wolf3; Benjamin Lebwohl2; Peter HR Green2
1Department of Psychiatry, Columbia University Irving Medical Center, New York, USA.
2Department of Medicine, Celiac Disease Center, Columbia University Irving Medical Center, Harkness Pavilion, New York, USA.
3Department of Health and Behavior Studies, Program in Nutrition, Teachers College, Columbia University, New York, USA.
*Corresponding Author : Janet E Schebendach
Department of Psychiatry, Columbia University Irving
Medical Center, New York, USA.
Email: js2202@cumc.columbia.edu
Received : Mar 22, 2024
Accepted : Apr 25, 2024
Published : Apr 30, 2024
Archived : www.jjgastro.com
Copyright : © Schebendach JE (2024).
Abstract
Introduction: Treatment for Celiac Disease (CeD) includes strict adherence to a Gluten-Free Diet (GFD) which may result in preoccupation with food choice, unwanted weight gain, and body dissatisfaction.
Objective: To determine frequency of Eating Disorder (ED) diagnoses and symptoms in adults with CeD.
Method: The Eating Disorder Diagnostic Scale (EDDS-DSM-5) and the Eating Pathology Symptoms Inventory (EPSI) were administered in a cross-sectional study of 50 adults with biopsy-confirmed CeD on a GFD for >1 year attending their routine clinic visits.
Results: Based on the EDDS, one participant met criteria for Diagnostic and Statistical Manual of Mental Disorders (DSM-5) diagnosis of binge eating disorder and four met criteria for possible diagnosis of Other Specified Feeding and Eating Disorders; none had previously been diagnosed with an ED. EDDS symptom scores were lower (i.e., better) than established cut-points, yet females scored higher than males when asked if they felt fat (p<0.001), feared weight gain (p<0.001), and felt undue influence of weight/ shape (p=0.034). EPSI scores were lower (i.e., better) than normative values, yet females scored significantly higher than males on body dissatisfaction (p<0.001), cognitive restraint (p=0.011), and purging (p=0.044) subscales.
Conclusion: Although disordered eating behaviors and weight/ shape concerns were apparent, only one patient met full criteria for an ED diagnosis. The EDDS and EPSI may be useful in screening for comorbidity among adults with CeD; however, clinical assessment is needed to assign a DSM-5 ED diagnosis.
Keywords: Celiac disease; Eating disorders; Eating disorder diagnostic scale; Eating pathology symptoms inventory.
Citation: Schebendach JE, Lee AR, Gholmie Y, Wolf R, Lebwohl B, et al. Disorder symptoms and diagnoses in adults with celiac disease. J Gastroenterol Res Pract. 2024; 4(4): 1196.
Introduction
Celiac Disease (CeD) is a genetically mediated autoimmune disease triggered by exposure to dietary gluten [1]. Prevalence is approximately 1% of the U.S. population [2,3], with twice as many females affected than males [4,5]. Gluten ingestion leads to pathological changes in the small intestine and malabsorption of nutrients, impacting many organ system (6). The only treatment for CeD is lifelong adherence to a gluten-free diet [7,8].
Maintenance of a strict Gluten-Free Diet (GFD) requires vigilance and control. This can result in preoccupation and anxiety around eating and food choice, and disordered eating behaviors may ensue [9]. Unwanted weight gain associated with implementation of a GFD may result in body dissatisfaction and restricting and/or purging behaviors [9], as well as purposeful gluten ingestion to promote weight loss [10]. Dietary noncompliance is associated with gastrointestinal and non-gastrointestinal comorbidity, including depression, bipolar disorder, anxiety disorders, and eating disorders [11].
Eating Disorders (ED) are psychiatric disorders characterized by disturbances in food intake and eating behaviors that adversely affect physical and mental health [12]. Studies suggest that risk of EDs among individuals with autoimmune diseases is high [13] and that a bidirectional relationship between EDs and CeD exists and warrants attention [9,14,15].
Hypothesis
Based on clinical observation and review of recent research, there is a subpopulation of individuals with CeD that may have disordered eating behaviors or diagnosable eating disorders.
Specific aims
In a cross-sectional sample of 50 adults with biopsy confirmed CeD we aimed: 1) to determine the prevalence of comorbid DSM-5 eating disorders (12; Supplement 1) using the Eating Disorder Diagnostic Scale-DSM-5 version (EDDS-DSM-5); 2) to distinguish between individuals with and without an eating disorder using the EDDS-DSM-5 symptom composite score; 3) to characterize disordered eating behaviors and body image concerns using the Eating Pathology Symptom Inventory (EPSI).
Material and methods
Study design and setting
A cross-sectional study was conducted at the Celiac Disease Center at Columbia University Irving Medical Center (CUIMC) in collaboration with the Program in Nutrition at Teachers College, Columbia University, and the Eating Disorders Research Center, New York State Psychiatric Institute, CUIMC. Institutional Review Board approval was obtained from CUIMC (8/1/2019) and Teachers College (9/5/2019). Enrollment began on 01/28/2020 but was paused from 3/8/2020-10/15/2020 due to the Covid-19 pandemic; recruitment resumed on 10/16/2020 and was completed on 12/15/2020.
Participants
Participants were 50 adult males and females, 18-to-45 years of age. Inclusion criteria included both a biopsy-confirmed diagnosis of CeD and the prescription of a GFD for at least 1-year. Exclusion criteria included self-reported or serum-diagnosed CeD (without biopsy), a diagnosis of CeD less than 1-year, and history of an ED.
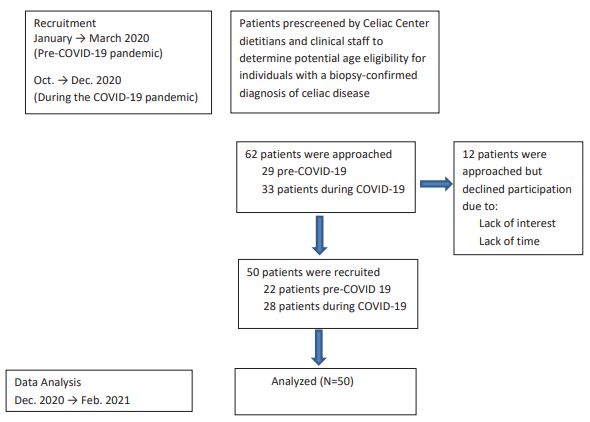
Potential research participants were pre-screened to determine eligibility prior to arrival for a scheduled outpatient clinic appointment at the Celiac Disease Center. Upon arrival, prescreened patients were consecutively approached by research staff to determine interest in study participation and obtain informed consent. Recruitment ended once the sample of 50 participants was attained (Figure 1. Recruitment flow sheet). Participants were provided with a questionnaire packet that took approximately 30-minutes to complete and they received a $50.00 gift card in return for their participation.
Demographic data
Age (date of birth), gender (female, male), ethnicity (Hispanic, non-Hispanic), race (White, Black or African American, Asian, other), education (highest level/grade achieved), and household annual income (<$50,000; $50,000 to $100,000; >100,000; prefer not to disclose) were collected.
Anthropometric
Body weight (clothed without shoes, minus 2 lbs. (0.907 kg) was measured by a Tanita dual frequency body composition analyzer. Height was measured by a wall-mounted stadiometer. Body Mass Index (BMI = weight in kg/ height in m2 ) was calculated by the Tanita scale.
Assessment measures
The Eating Disorder Diagnostic Scale - DSM-5 (EDDS-DSM5): The EDDS-DSM-5 [16] is a brief self-report scale that generates possible ED diagnoses and a symptom composite score. The 23-item measure includes Likert scales, dichotomous scores, behavioral frequency scores, and open-ended questions. The EDDS diagnostic scale has been used to screen for Anorexia Nervosa (AN), Bulimia Nervosa (BN), Binge Eating Disorder (BED), and Other Specified Feeding and Eating Disorder (OSFED) using instrument-specific scoring syntax. The EDDS symptom composite score is a continuous measure of eating pathology. Based on the EDDS-DSM-IV version of the EDDS, a symptom composite score >16.5 accurately distinguishes between females with and without a diagnosable eating disorder [17]; a cut point for males has not been established. Adequate criterion, predictive and convergent validity, internal consistency, sensitivity, and test-retest reliability were documented for the EDDS-DSM-IV version [18,19].
The Eating Pathology Symptoms Inventory (EPSI): The EPSI [20] is a self-report questionnaire designed to be a comprehensive multidimensional measure of eating pathology. It includes 45 items, each scored on a 5-point scale, covering eight subscales: body dissatisfaction (dissatisfaction with body weight and/or shape), binge eating (ingestion of large amounts of food and accompanying cognitive symptoms), cognitive restraint (cognitive efforts to limit or avoid eating, whether or not such attempts are successful), purging (self-induced vomiting, laxative use, diuretic use, and diet pill use), excessive exercise (physical exercise that is intense and/or compulsive), restricting (concrete efforts to avoid or reduce food consumption), muscle building (desire for increased muscularity and muscle building supplement use), and negative attitudes toward obesity (negative attitudes toward individuals who are overweight or obese). Reliability and validity have been established [21]. EPSI subscales show evidence for factor structure replicability in males and females, and excellent convergent, discriminant, and criterion validity; gender norms are available, and higher subscale scores are associated with increased ED symptomatology [22].
Data analysis
The independent samples t-test was used to compare demographic and anthropometric variables, the EDDS symptom composite score, and EPSI subscale scores between male and female participants. The one sample t-test was used: 1) to compare the EDDS symptom composite score of female participants with the established clinical cut-point of 16.5 (17); and 2) to compare EPSI subscale scores with established gender norms for male and female college students (22). Pearson correlation coefficients were calculated to compare EDDS and EPSI scores for selected variables. Analyses were performed by SPSS (version 28). Means +/- SDs are reported; t-tests were 2-tailed. Statistical significance was set at p<0.05. Effect size was assessed via Cohen’s d. Methods used to address missing data are described in Supplement 2.
Results
Sixty-two patients were approached, 12 declined, and 50 (35 females and 15 males) completed the study (Figure 1). Participants ranged in age from 19 to 45 years, with a mean age of 29.56 (+/- 7.4) yrs. Mean age at the time of CeD diagnosis was 22.76 +/- 9.28 yrs. Mean duration of illness was 7.2 +/- 5.3 yrs., with 40% diagnosed for 1-4 yrs., 40% diagnosed for 5-10 yrs., and 10% diagnosed for more than 10 yrs. Overall, 10% of the participants identified as Hispanic, 94% as White, 2% as Black or African American, 4% as Asian, and 6% as other race. More than half of the participants were college graduates (64%); 16% had some college education, and 20% had a postgraduate degree. Household income of participants was greater than $100,000 in 62%, between $50,000 and $100,000 in 22%, and less than $50,000 in 8%; the remaining 8% did not disclose income.
BMI, calculated from measured height and weight, ranged from 16 to 34 kg/m2 (mean 22.61 +/- 3.84) in females and 20 to 35.9 kg/m2 (mean 24.72 +/- 3.89) in males (t(48)=-1.77, p=0.08; Cohen’s d=-0.54). BMI classification among female participants (n=35) included 4 underweight (11.4%), 23 healthy weight (65.7%, 7 overweight (20%), and 1 obese (class I; 2.9%); none of the underweight females met criteria for an ED diagnosis. BMI classification among male participants (n=15) included 10 healthy weight 66.6%, 4 overweight (26.7%), and 1 obese (class II; 6.7%). Self-reported current weight as a percentage of highest weight was 93.2 (+/- 6.5)% in females and 94.7 (+/- 5.5)% in males (t(48)=0.78, p=0.43; Cohen’s d=0.24).
EDDS-DSM-5 diagnostic scale
The EDDS was completed by all 50 participants. Based on the EDDS diagnostic scale, one male and four female participants (10%) met criteria for a possible ED diagnosis: one with binge eating disorder (BED) and four with other feeding and eating disorders (OSFED; one with low frequency bulimia nervosa and three with night eating syndrome). Although the EDDS can determine DSM-5 BED with a reasonable degree of certainty, OSFED requires clinical assessment/interview to confirm the diagnosis. It is noteworthy that one participant endorsed selfinduced vomiting, fasting, intense exercise, and night eating however; the scoring syntax defaulted to a diagnosis of night eating syndrome. Once again, confirmation of a DSM-5 diagnosis by clinical interview was not conducted.
Weight and shape-related issues were endorsed by the five participants with a possible ED diagnosis. All answered affirmatively to the EDDS question “Has your weight or shape influenced how you judge yourself as a person?”, and four out of five answered affirmatively to “Have you felt fat?” and “Have you had a definite fear that you might gain weight or become fat?” In the full study sample (Table 1), the scores for felt fat, fear of weight gain/becoming fat, and weight/shape influence were all significantly higher (i.e., worse) in female vs. male participants, with medium to large effect sizes noted. The proportion of affirmative responses among both male and female participants (n=50) to felt fat, fear of weight gain, and weight/shape influence were 72%, 68%, and 80%, respectively. Among males (n=15), the proportion of affirmative responses to felt fat, fear of weight gain, and weight/shape influence were lower (53.4%, 40%, and 66.7%, respectively). Among females (n=35), the proportion of affirmative responses to felt fat, fear of weight gain, and weight/shape influence were higher (80%, 80%, and 85.7%, respectively).
EDDS-DSM-5 symptom composite score
The EDDS symptom composite score was 10.06 (+/- 13.24) in males and 13.57 (+/- 9.53) in females. Although this difference was not statistically significant (t(48)=-1.056, P=0.29), a small effect of gender was observed (Cohen’s d=- 0.32). In the current study, 10 out of 35 female participants had a symptom composite score >16.5. A one-sample t-test was conducted to determine whether the composite score of our female sample (n=35) differed from the clinical cut-off of 16.5. Although the mean score (13.57 +/- 9.53) of female CeD patients was lower than the 16.5 cut-off, this difference was not statistically significant (t(34)=-1.817, p=0.078, Cohen’s d=- 0.307). A male gender EDDS symptom composite score cut-off is not available; however, two out of 15 male participants had scores greater than 16.5, one of which was the highest score (53) in the total study sample.
EPSI subscale scores
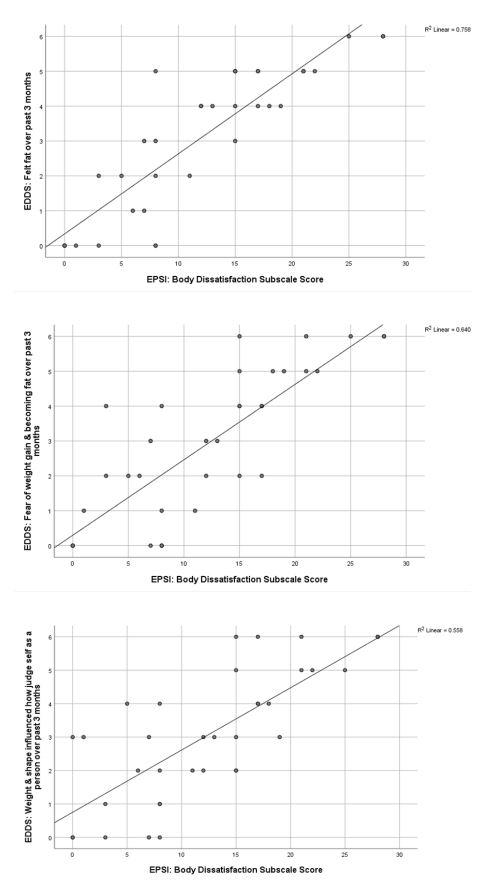
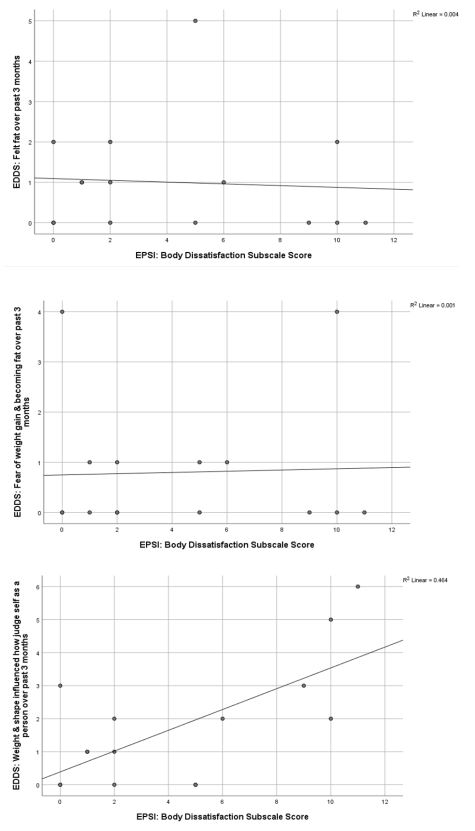
EPSI subscale scores are summarized in Table 2. Scores for Body Dissatisfaction, Cognitive Restraint, and Purging were significantly higher in female vs. male CeD patients. One-sample t-tests were conducted to compare the EPSI subscale scores of CeD study participants with EPSI scores from healthy control (i.e., without EDs) college students reported by Forbush, Wildes & Hunt [22]. In both the male and female CeD groups, subscale scores were significantly lower than normative values of male and female college students (Supplement 3). The EPSI body dissatisfaction subscale score and the EDDS scores for “felt fat”, “fear of weight gain/becoming fat”, and “weight/shape influence” were all significantly higher in female vs. male CeD participants. In females (Figure 2A), EPSI body dissatisfaction was significantly and positively correlated with EDDS “felt fat” (r=0.871, p=0.01), EDDS “fear wt. gain/becoming fat” (r=0.8, p=0.01), and EDDS “weight/shape influence” (r=0.747, p=0.01). In males (Figure 2B), EPSI body dissatisfaction was significantly and positively correlated with EDDS “weight/shape influence” (r=0.681, p=0.01), but failed to significantly correlate with EDDS “felt fat” (r=-0.065, p=0.819) or EDDS “fear weight gain/becoming fat” (r=0.036, p=0.899).
Discussion
This study screened 50 biopsy-confirmed adults with CeD to determine the prevalence of DSM-5 EDs using the EDDS-DSM-5 diagnostic scale; assessed the degree of ED symptomatology using the EDDS-DSM-5 symptom composite score; and evaluated participants for disordered eating behaviors and body image concerns using the EPSI.
Prevalence of a DSM-5 ED diagnosis
Five out of 50 adult patients (10%) with CeD and not previously diagnosed with an ED were found to have a DSM-5 ED diagnosis based on the EDDS-DSM-5 diagnostic scale. This rate is somewhat higher than the meta-analysis pooled prevalence of 6.37% [95% CI: 3.05, 10.75] from six cross-sectional studies of adults with CeD [13]. In their review of 14 studies of children, adolescents, and adults with CeD, Nikniaz et al. [13] reported that the subgroup meta-analysis of pooled prevalence of ED in CeD was higher in studies that used questionnaires vs. DSM-IV/ ICD codes for diagnosis of ED (17.36% vs. 3.45%, respectively), higher in studies that used biopsy/ICD-10 codes vs. serology for diagnosis of CeD (7.59% vs. 1.69%, respectively), and higher in studies with small (<500) vs. large (>500) sample sizes (16.56% vs. 1.35%, respectively). In the current study, an ED diagnosis was determined via questionnaire in a relatively small sample of biopsy-confirmed patients with CeD. Collectively, these may have skewed our results towards a higher vs. lower prevalence rate.
The current study used the EDDS adapted for the DSM-5. Sysko et al. [23] compared accuracy of a DSM-5 diagnosis determined by the Eating Disorders Assessment for DSM-5 (EDA5) semi-structured interview with that assigned by the EDDSDSM-5. Their results indicated that 9 out of 69 participants (13%) with an ED diagnosis determined by the EDA-5 semi-structured interview had no diagnosis when screened by the EDDS, and 5 out of 69 participants (7.2%) assigned a diagnosis of BED by the EDA-5 semi-structured interview were misdiagnosed as BN when screened by the EDDS. The EDDS-DSM-5 scoring syntax assigns a diagnosis of AN, BN, BED, atypical AN, low frequency BN, low frequency BED, purging disorder, and Night Eating Syndrome (NES). In the current study, one patient was diagnosed with BED and four were diagnosed with OSFED (one with low frequency BN and three with NES). Prior studies suggest that the EDDS may over-, under-, or misdiagnose an eating disorder. Given that clinical assessment and probing are necessary to determine gradations in cognitions and behaviors associated with EDs classified under OSFED, the assignment of an OSFED diagnosis based solely on the EDDS must be viewed with caution. For example, three patients with CeD were assigned an OSFED diagnosis of NES. Normal eating patterns of individuals with CeD may be affected by limitations of the diet itself such as the restrictive nature of the GFD, low availability of safe GF food, and concerns over chance gluten exposure when dining out. Given the possibility that individuals with CeD may have limited access to GF foods outside the home and greater access to GF foods inside the home, it’s possible that normal patterns of ingestion are skewed towards eating larger amounts of food later in the day or evening at home. Without probing, this could not be determined.
EDDS symptom composite score
The EDDS composite score may be used to assess the overall level of eating pathology as well as to differentiate between individuals with and without an eating disorder. Although the mean EDDS symptom composite score of our 35 female participants was lower than the 16.5 clinical cut-point established by Krabbenborg [17], 10 participants (28.6%) had scores above the cut-point; four with an EDDS assigned ED diagnosis and six without.
Prior to their CeD diagnosis, individuals may present as underweight. Compliance with a gluten-free diet in CeD is typically associated with the resolution of malabsorption and weight gain [24]; however, in some individuals, weight gain may be negatively interpreted and trigger disordered eating behaviors [25]. The EDDS composite score of our female participants was influenced by their response to questions related to weight and shape (EDDS Questions 1-3). Only a few studies have assessed the development of EDs in adults with CeD, and even fewer describe specific behaviors and attitudes associated with disordered eating. In a study of 100 newly diagnosed adult females with CeD, the drive for thinness subscale score on the Eating Disorder Inventory-2 [26] was significantly higher in patients vs. controls; however, no significant between-group difference in the body dissatisfaction subscale score was reported [27]. In a study of 177 adult females with CeD, Arigo et al. [28] administered the Eating Disorder Examination Questionnaire [29] and reported that 22% of participants had symptoms “in line with eating disorders of clinical significance” and that concerns about one’s body shape were slightly higher than normative levels. The degree to which gastrointestinal symptoms characteristic of CeD (e.g., distension, bloating, flatulence) influence body image, and shape/weight concerns in our female participants is also unknown.
EPSI subscale scores
Scores on all eight EPSI subscales were significantly lower than normative data in our male and female participants. This may stem from disparate sample sizes and age groups. Within our sample, females had a higher Body Dissatisfaction score than did their male counterparts; this difference was both statistically and clinically significant. Likewise, Forbush et al. [22] reported a significantly higher Body Dissatisfaction score in female vs. male college students (p<0.05) with a large effect size (Cohen’s d=-1.14). Similar to our findings, Forbush et al. [22] reported that college women had significantly higher EPSI scores than college men on the Cognitive Restraint and Purging subscales; in contrast to their finding of a significantly higher Muscle Building score in college men vs. college women, our relatively small sample of males had a score that was clinically (Cohens d=0.7) but not statistically different (p=0.066) from their female counterparts.
Forbush et al. [22] reported significant and positive correlations between the EPSI Body Dissatisfaction score and the Eating Disorder Examination-Questionnaire [30] Weight Concern Scale and the Weigh Concerns Scale in both male and female college students. In the current study, significant positive correlations were found between the EPSI Body Dissatisfaction score and EDDS scores for “felt fat”, “fear of weight gain/becoming fat”, and “weight/shape influence” in our female participants (Figure 2A), but only between the EPSI Body Dissatisfaction score and EDDS “weight/shape influence” in our male participants (Figure 2B). This may suggest a heightened level of concern about weight, shape, and size in our female participants; however, the degree to which gastrointestinal manifestations related to CeD (e.g., distension, bloating, weight-gain related to improved absorption) influenced body image, and shape/weight concerns in is unknown.
Strengths and limitations
Strengths of this study include biopsy-confirmed patients CeD; a gender distribution similar to the 2:1 ratio of females to males with CeD in the general population; and use of two validated screening instruments (EDDS-DSM-5 and EPSI). There are, however, several important limitations. First and foremost, the cross-sectional study design does not allow for a causal link between ED symptoms and diagnosis of CeD; therefore, directionality cannot be determined. Second, a healthy non-CeD control group was not included. Third, higher ED prevalence rates are reported by questionnaires compared to clinical interviews/assessments. Fourth, an EDDS diagnosis of OSFED in four participants could not be confirmed by clinical interview/assessment. Fifth, GI symptoms related to CeD (bloating, distension, weight gain) may be misinterpreted as weight/shape and body image concerns secondary to an ED. Sixth, two studies examining the prevalence of eating disorders in adults with biopsy-confirmed celiac disease have been published, and neither used the EDDSDSM-5 and/or EPSI for assessment or diagnosis of an eating disorder [13]. Given that the current study is largely exploratory, a sample size of 50 was selected for the adult cohort. Lastly, given that eating disorders, particularly anorexia nervosa, typically present in mid to late adolescence, this study may have underestimated the prevalence of ED, since those with a prior ED diagnosis were not included; a study in 14-to-17-year-old patients with biopsy-confirmed CeD is currently underway.
Conclusion
Clinically significant disordered eating behaviors and weight and shape concerns were apparent in this sample of adults with CeD; however, only one patient with BED met criteria for a fully recognized DSM-5 eating disorder. Sub-threshold presentations in four additional patients with an EDDS-DSM-5 assigned diagnosis of OSFED requires confirmation by clinical interview. The EDDS and EPSI may be useful in screening for disordered eating behaviors and body image concerns; however, clinical assessment is necessary to determine if an adult with CeD has a comorbid DSM-5 eating disorder diagnosis. In assessing the patient’s quality of life, eating patterns, attitudes and behaviors, the clinician or registered dietitian nutritionist, needs to be cognizant of the potential impact of the restrictive nature of the diet, changes in weight, and vigilance in maintaining food safety which has the potential to incline the patient toward either disordered eating behaviors or a clinical eating disorder.
Declarations
Conflicts of interest: The authors declare no conflicts of interest.
Funding sources/financial support: This research received no external funding.
Potential competing interests: None.
Acknowledgments: B.T. Walsh, MD, Department of Psychiatry, Columbia University Irving Medical Center for expert guidance and critical review of the final manuscript. Particia Zybert, PhD, MPH for expert statistical analysis and data management. Jessica Lebovits, MS, RD, Department of Medicine, Celiac Disease Center, Columbia University Irving Medical Center, for screening and enrolment of participants and review of completed assessment measures.
References
- Lebwohl B, Ludvigsson JF, Green PHR. Celiac disease and nonceliac gluten sensitivity. BMJ. 2015; 351: h4347.
- Lebwohl B, Sanders DS, Green PHR. Coeliac disease. Lancet. 2018; 391: 70-81.
- Rubio-Tapia A, Ludvigsson JF, Brantner TL, et al. The prevalence of celiac disease in the United States. Am J Gastroenterol. 2012; 107: 1538-44.
- Fasano A, Catassi C. Clinical practice. Celiac disease. N Engl J Med. 2012; 367: 2419-26.
- Rashtak S, Murray JA. Celiac disease in the elderly. Gastroenterol Clin North Am. 2009; 38: 433-46.
- Reinhardt K, Fanzo J. Addressing chronic malnutrition through multi-sectoral, sustainable approaches: A review of the causes and consequences. Front Nutr. 2014; 1: 13.
- Ludvigsson JF, Bai JC, Biagi F, et al. Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology. Gut. 2014; 63: 1210-28.
- Rubio-Tapia A, Hill D, Kelly CP, et al. ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol. 2013; 108: 656-76.
- Hedman A, Breithaupt L, Hübel C, et al. Bidirectional relationship between eating disorders and autoimmune diseases. J Child Psychol Psychiatr. 2019; 60: 803-12.
- Satherley RM, Higgs S, Howard R. Disordered eating patterns in coeliac disease: a framework analysis. J Hum Nutr Diet. 2017; 30: 724-36.
- Liester MB, Liester MG. A review of psychiatric disorders associated with celiac disease. Dual Diagn Open Acc. 2017; 2(2): 35.
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA: American Psychiatric Association. 2013.
- Nikniaz Z, Beheshti S, Abbasalizad Farhangi M, Nikniaz L. A systematic review and meta-analysis of the prevalence and odds of eating disorders in patients with celiac disease and vice-versa. Int J Eat Disord. 2021; 1-12.
- Marild K, Stordal K, Bulik CM, et al. Celiac Disease and Anorexia Nervosa: A Nationwide Study. Pediatrics. 2017; 139: e20164367.
- Golden NH, Park KT. Celiac disease and anorexia nervosa – an association well worth considering. Pediatrics. 2017; 139: e20170545.
- Stice E. The Eating Disorder Diagnostic Scale (EDDS-5) for the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5). Oregon Research Institute. http: //www.ori.org/sticemeasures/
- Krabbenborg MAM, Danner UN, Larsen JK, et al. The Eating Disorder Diagnostic Scale: psychometric features within a clinical population and a cut-off point to differentiate clinical patients from healthy controls. Eur Eat Disorders Rev. 2012; 20: 315-20.
- Stice E, Fisher M, Martinez E. Eating disorder diagnostic scale: additional evidence of reliability and validity. Psychol Assess. 2004; 16: 60-71.
- Stice E, Telch CF, Rizvi SL. Development and validation of the Eating Disorder Diagnostic Scale: A brief self-report measure of anorexia, bulimia, and binge-eating disorder. Psychol Assess. 2000; 12: 123-31.
- Forbush KT, Wildes JE, Pollack LO, et al. Development and validation of the Eating Pathology Symptoms Inventory (EPSI). Psychol Assess. 2013; 25: 859-78.
- Forbush KT, Bohrer BK, Hagan KE, et al. Development and initial validation of the Eating Pathology Symptoms Inventory- Clinician-Rated Version (EPSI-CRV). Psychol Assess. 2020; 32: 943-55.
- Forbush KT, Wildes JE, Hunt TK. Gender norms, psychometric properties, and validity for the Eating Pathology Symptoms Inventory. Int J Eat Disord. 2014; 47: 85-91.
- Sysko R, Glasofer DR, Hildebrandt T, et al. The eating disorder assessment for DSM-5 (EDA-5): Development and validation of a structured interview for feeding and eating disorders. Int J Eat Disord. 2015; 48(5): 452-63.
- Freeman HJ. Pearls and pitfalls in the diagnosis of adult celiac disease. Can Journal Gastroenterol. 2008; 22: 273-80.
- Satherley RM, Howard R, Higgs S. The prevalence and predictors of disordered eating in women with coeliac disease. Appetite. 2016; 107: 260-7.
- Garner DM, Olmstead MP, Polivy J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Int J Eat Disord. 1983; 2: 15-34.
- Passananti V, Siniscalchi M, Zingone F, et al. Prevalence of eating disorders in adults with celiac disease. Gastroenterol Res Pract. 2013: 1-7.
- Arigo D, Anskis AM, Smyth JM. Psychiatric comorbidities in women with celiac disease. Chronic Ill. 2011; 8: 45-55.
- Fairburn C, Beglin SJ. Assessment of eating disorders: interview or self-report questionnaire? Int J Eat Disord. 1994; 16: 363-70.
- Fairburn CG, Cooper Z. The Eating Disorders Examination (12th ed.) In: Fairburn C, Wilson G, eds. Binge Eating: Nature, Assessment, and Treatment). New York: Guilford Press. 1993: 317-60.