
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 4
Valproic acid-induced acute pancreatitis: First case report in Morocco and literature review
Fjouji Salahedddine1*; Elbouti Anass2 ; Houba Abdelhafid2 ; Kartit Nourreddine1 ; Doghmi Nawfal2 ; Balkhi H2
1Anesthesia and Intensive Care Department, Mohamed V Military Training Hospital Hassan II University of Casablanca, Morocco.
2Anesthesia and Intensive Care Department, Anesthesia and Intensive Care Department, Mohamed V University of Rabat, Morocco.
*Corresponding Author : Fjouji Salaheddine
Anesthesia and Intensive Care Department, Mohamed V
Military Training Hospital Hassan II University of Casablanca, Morocco.
Tel: 00212660006390;
Email: fjoujisalah@gmail.com
Received : Mar 21, 2024
Accepted : Apr 18, 2024
Published : Apr 25, 2024
Archived : www.jjgastro.com
Copyright : © Salaheddine F (2024).
Abstract
Acute pancreatitis is an inflammation of the pancreas following self-destruction by its own enzymes responsible for local lesions and systemic response. In rarely cases, several drugs are described as having adverse effects causing acute pancreatitis outside of a context of drug intoxication. Classically, drug-induced acute pancreatitis tends to be edematous and has a relatively limited course over time. Several cases of pancreatitis due to sodium valproate are described in the literature. We describe a first clinical case in Morocco of an epileptic adolescent treated with sodium valproate who developed severe acute pancreatitis. Making a diagnosis of drug-induced acute pancreatitis is based to evaluate intrinsec and extrinsec imputability of this drug. The mortality of valproate acid-related pancreatitis is estimated at 15%. Neurologists, pediatricians and emergency physicians must be informed of this complication.
Keywords: Acute pancreatitis; Drug-induced; Valproic acid; Moroccan case.
Citation: Salahedddine F, Anass E, Abdelhafid H, Nourreddine K, Nawfal D, et al. Valproic acid-induced acute pancreatitis: First case report in Morocco and literature review. J Gastroenterol Res Pract. 2024; 4(4): 1194.
Introduction
Acute pancreatitis is an inflammation of the pancreas following self-destruction by its own enzymes responsible for local lesions and systemic response. The severity varies from simple edema of the gland to diffuse necrosis with life-threatening systemic inflammation. Obstruction by cholelithiasis and chronic alcoholism remain the most common causes. Hereditary, malformative, infectious and autoimmune causes are less common. More rarely, several drugs are described as having adverse effects causing acute pancreatitis outside of a context of drug intoxication. Thus, several cases of pancreatitis due to valproic acid are described in the literature, most of which concern children and young adults [1]. We describe a first clinical case in Morocco of an epileptic adolescent treated with sodium valproate who developed severe acute pancreatitis and we review the literature on this subject.
Case report
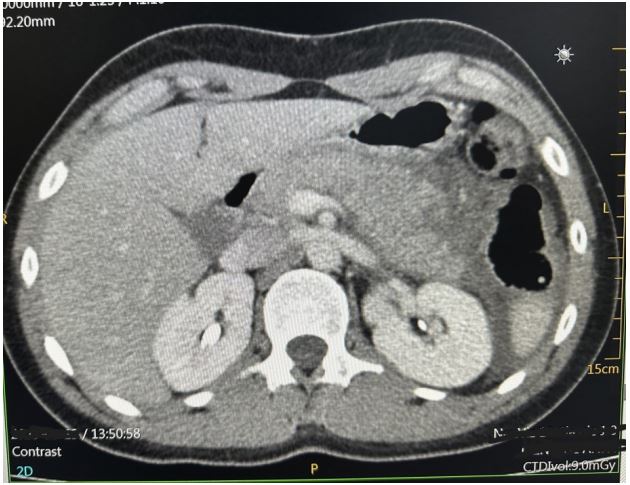
A Moroccan 17 year old male presented to the emergency department for four days of newly experienced epigastric pain associated to non-bloody and non-bilious emesis. The patient the child was diagnosed with epilepsy for which treatment with sodium valproate was initiated. The last dosage is changed nine months before from 750 mg to 1 g to maintain a dose of 20 mg/kg/d. There was no seizure the last year. On presentation he denied history of other new medications, supplements, alcohol or drug use, gallstones, fevers or chills. The epigastric pain was intense and resistant to anttispasmodic and oméprazole. Physical examination on arrival was notable for uncomfortable appearing, he complains of intense localized pain in the epigastrium radiating towards the back with an attitude of leaning forward. He was apyretic. On palpation we noted a focal epigastric tenderness with non-peritonitic abdomen. Respiratory and hemodynamic functions were stable. blood pressure 125/67, pulse 87, respiratory rate of 20, spo2 of 100%. The rest of the physical examination findings were unremarkable without any rashes, joint swelling, or adenopathy. Serum laboratory investigations in the emergency department revealed the following pertinent and significant findings: lipase level of 462 U/l, white blood cell count of 11.000 per mm3 , Activated protein C 27 mg/l, hemoglobin 10.6 g/dl, AST 28U/L, ALT 25U/L, Total bilirubin 8.2 mg/L, sodium 141 mmol/l, potassium 4.2 mmol/l, BUN 0.35 g/l, creatinine 10,2 mg/l, calcium 90 mg/l, and. All other initial laboratory invetigations within normal limits or insignificant. Patient was resuscitated with two liters of isotonic saline serum, received a total of 40 mg of intravenous omeprazole, 500 mg of intravenous paracetamol, and 4 mg of intravenous morphine. Initial abdominal ultrasound showed a normal gallbluddder, without any stones, gallbludder wall thickening, or common bile duct dilatation. the pancreas is globular with infiltration of gastric fat and presence of moderate peritoneal effusion (Figure 1). Subsequently, patient underwent a computed tomography of abdomen and pelvis with intravenous contrast (Figure 2). The pancreas was enlarged, had a homogeneous density, with a discreet homogeneous enhancement without an area of pancreatic parenchymal necrosis. presence of a peritoneal effusion of medium abundance surrounding the pancreas, perigastric, perihepatic, perisplenic level and in pelvic slope. The gallbladder, bile ducts, liver, spleen and kidneys were without abnormalities. The appearance was an acute edematous pancreatitis grade E of Balthazar. Patient was admitted to intensive care unit, he continued to receive intravenous boluses and maintenance fluids per standards of care for acute pancreatitis, along with adjunct therapies including antispasmodic, omeprazole and morphine to control pain. Food is reintroduced gradually from the 3rd day after the nausea and vomiting have disappeared and the pain has been controlled. we started with water, herbal teas, vegetable broths in small volumes. All this while monitoring digestive tolerance and the absence of pain. During the first days of hospitalization, patient underwent an extensive panel of investigations including bili-MRI showed the absence of stones in the Wirsung duct and bile ducts which are not dilated, no malformation or pancreatic mass is revealed (Figure 3). The other investigations were hematological toxicology screen, viral screening (including A, B and C hepatitis panel, respiratory viral panel, measles mumps rubella panel Epstein barr, cytomegalovirus panel), TPHA VDRL serology, tuberculosis quantiferon, lipid panel (cholesterol 1.46 g/L, triglycerids 0.9 g/L), blood smear, thyroid panel, antinuclear and anticardiolipin antibodies, hemoglobin electrophoresis; all returning either within normal or unremarkable limits. The absence of another cause responsible for pancreatitis led us to consider the drug etiology, particularly sodium valproate. Neurology consult was placed. Treatment with valproate of sodium was stopped and replaced by levetiracetam 250 mg twice a day. The opatient made a full recovery and was discharged after a total of eight days with prescription of levetiracetam. Any epileptic crisis was observed. The patient continue to have regular outpatient neurology follow up.


Discussion
The involvement of a drug in the triggering of acute pancreatitis is a rare event (less than 2%) [2] but not exceptional in adults. In children, acute drug-induced pancreatitis represents 30% of Acute Pancreatitis cases alongside traumatic causes [3]. To make a drug-induced etiological diagnosis of acute pancreatitis, no clinical criterion is formally specific to acute medicinal pancreatitis. There is no known individual predisposing factor for a particular sensitivity of the pancreas to a drug. Classically, drug-induced acute pancreatitis tends to be edematous and has a relatively limited course over time, provided that the drug in question has been suspended [4]. In 10 to 15% of cases, druginduced acute pancreatitis may develop in a necrotic-hemorrhagic manner and represent a severe form [5]. A first criterion for a drug-induced probability of pancreatitis is knowledge of the circumstances of occurrence in relation to the start of treatment. The closer the time of introduction of the drug, the more its involvement is highly suspect. The characteristics of the evolution of pancreatitis symptoms after stopping the drug and the risk of reappearance of symptoms after reintroduction of the molecule are also important data. A course is more suggestive when the symptoms regress after stopping the drug. The therapy in question, the clinical signs (pain, nausea, transit disorders) disappearing more quickly than the biological abnormalities (hyperamylasemia, hyperlipasemia). These criteria can only be analyzed in cases of moderate intensity acute pancreatitis; we know in fact that necrotic-hemorrhagic acute pancreatitis can progress over several weeks towards improvement or worsening, independently of the cessation of potentially pancreatotoxic treatment. A second Criterion 2 is that of eliminating differentials, namely pancreatitis of alcoholic, biliary, tumoral, hereditary, autoimmune, and infectious origin. In children and young people, we consider eliminating pancreatitis of viral, bacterial or parasitic origin (coxsackies, mumps, hepatitis A, B or C, chlamydia, salmonella, cytomegalovirus, Yersinia, Campylobacter, roundworm) or even possibility of recurrent AP due to congenital anomaly of the pancreatic ducts (pancréas divisum) [6]. The first 2 criteria represent an evaluation of the intrinsic imputability of the drug, the third criterion concerns extrinsic imputability. Thus, we know a list of drugs whose pancreatic toxicity is documented and classified in list B3: Valproic acid, Losartan, Mesalazine, Asparaginase, Mercaptopurine, Azathioprine, Methyldopa, Cimetidine. This class B3 includes drugs that have caused at least one case of acute pancreatitis with positive readministration reported. A Pancreatox file, which brings together 261 international nonproprietary names with the 1,115 corresponding bibliographic references, was published in 2001, classifying them into 3 groups according to the risk of pancreatotoxicity [7]. In this case report, the absence of an alternative diagnosis, the attributability of valproic acid (class B3), the appearance of pancreatitis after a few months of an increase in dose (from 750 mg to 1000 mg per day) are the elements which make the diagnosis of drug-induced pancreatitis is most likely. Valproic acid (dipropylacetic acid) or sodium valproate, a branched-chain carboxylic acid, is currently recommended to treat epilepsy, acute mania, and bipolar disorders and to prevent migraine headache [8]. While generally considered safe, valproic acid is associated with adverse effects such as skin rashes, bone marrow suppression, liver or kidney injury, hyperammonemia, and teratogenicity [8]. Valproic acid has also been incriminated first time as a cause of acute pancreatitis in 1979 [8]. Several reviews were subsequently published, the most recent of which are by Chapman 2002, Yazdani 2002 and Bischof in 2023 [9-11]. This case report would be the first described case of pancreatitis linked to valproic acid in Morocco. Bischof and al. [1] showed between 1979 and 2023, among 125 subjects (66% moins de 16 ans predominantly affected by an epilepsy) with an acute pancreatitis related to valproic acid. The diagnosis was made 11 (3.0-24) months (median and interquartile range) after starting valproic acid. One hundred and five cases (84%) recovered and twenty (16%) died. 16 of 19 (84%) subjects who were rechallenged with valproic acid after recovery, developed a further episode of pancreatitis. The physiopathological mechanism to explain the effect of valproate on the pancreas is not well elucidated. However, it is currently believed that valproic acid-associated pancreatic injury result from an accumulation of free radicals secondary to radical scavenger depletion [9,11]. The outcome is favorable in 84% of cases and allows recovery in less than 4 weeks for 81% of cases of pancreatitis [1]. A risk of recurrence after reintroduction of valpraoate is high 84%, hence it would be preferable to change the epilepsy treatment molecule once pancreatitis has appeared under sodium valproate [1]. The mortality of valproate acid-related pancreatitis is estimated at 15% [1]. Early severity is linked to the onset of a sepsis-like state of shock with risk of multi-organ failure. This risk obliges clinicians to consider the diagnosis as early as possible in the face of any acute digestive picture in a patient treated with sodium valprate by carrying out abdominal imaging and/or a pancreatic enzyme assay.
Conclusion
Drug-induced pancreatitis is rare but not exceptional. Sodium valproate is known to cause this type of complication. neurologists, pediatricians and emergency physicians must be informed of this risk and remain vigilant in order to make an early diagnosis and adequate management including stopping the resumption of treatment with sodium valproate given the increased risk of recurrence.
References
- Bischof MCM, Stadelmann MIE, Janett S, Bianchetti MG, Camozzi P, et al. Valproic Acid-Associated Acute Pancreatitis: Systematic Literature Review. J Clin Med. 2023; 12(18): 6044. doi: 10.3390/jcm12186044.
- Lankisch P, Dröge M, Gottesleben F. Drug-induced pancreatitis: incidence and severity. Gut. 1995; 37: 565-7.
- Jordan SC, Ament M. Pancreatitis in children and adolescents. J Pediatr. 1977; 91: 211-6.
- Rünzi R, Layer P. Drug-associated pancreatitis: facts and fiction. Pancreas. 1996; 13: 100-9.
- Banerjee A, Patel K, Grainger S. Druginduced pancreatitis. A critical review. Med. Toxicol. Adverse Drug Exp. 1989; 4: 186-98.
- Escourrou J, Buscail L. Quel bilan devant une pancréatite aiguë probablement non A non B. Gastroenterol Clin Biol. 2001; 25: 1S28-1S33.
- Biour M, Delcenserie R, Grange JD, Weissenburger J. Pancréatotoxicité des médicaments. Gastroenterol Clin Biol. 2001; 25: 1S22-1S27. Cette base de données régulièrement actualisée regroupe les références bibliographiques colligées dans des ouvrages de référence ayant trait à la gastroentérologie
- Peterson GM, Naunton M. Valproate: A simple chemical with so much to offer. J. Clin. Pharm. Ther. 2005; 30: 417-421.
- Chapman SA, Wacksman GP, Patterson BD. Pancreatitis associated with valproic acid: A review of the literature. Pharmacotherapy. 2001; 21: 1549-1560.
- Yazdani K, Lippmann M, Gala I. Fatal pancreatitis associated with valproic acid: Review of the literature. Medicine. 2002; 81: 305-310.
- Kelley RI. The role of carnitine supplementation in valproic acid therapy. Pediatrics. 1994; 93: 891-892.