
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Evaluation of multiple autoantibodies to tumor-associated antigens as potential diagnostic markers for pancreatic cancer
Xiao Wang†; Cuipeng Qiu†; Jiejie Qin; Bofei Wang; Jian-Ying Zhang*; Baofa Yu*
Border Biomedical Research Center, The University of Texas at El Paso, El Paso, TX 79968, USA.
*Corresponding Author : Jian-Ying Zhang & Baofa Yu
Border Biomedical Research Center, the University of
Texas at El Paso, El Paso, TX 79968, USA.
Email: jzhang@utep.edu & bfyuchina@126.com
Received : Mar 15, 2024
Accepted : Apr 15, 2024
Published : Apr 22, 2024
Archived : www.jjgastro.com
Copyright : © Zhang JY & Yu B (2024).
Abstract
The aim of the study is to evaluate the clinical significance of autoantibodies to GNA11, MSLN, GNAS, CEBPA, MDM2, p16, Sui1, Calnuc, PTEN in Pancreatic Cancer (PC). A total of 33 sera from PC patients and 45 sera from Normal Controls (NC) were enrolled to measure nine autoantibodies by Enzyme-Linked Immunosorbent Assay (ELISA). Multiple parameters in individual or combination forms were applied for evaluation. The level of all autoantibodies except anti-GNAS and anti-Calnuc was significantly higher in PC patients than that in normal controls. Significantly increased frequencies were found for four autoantibodies to MSLN, p16, PTEN and Sui1 at 75.8%, 66.7%, 30.3% and 27.3% compared to normal controls (4.9%). The ability of these autoantibodies to distinguish PC patients from normal controls reflected by the area under ROC curve (AUC) ranged from 0.666 to 0.884, with anti-p16 (0.884 of AUC) and anti-MSLN (0.857 of AUC) showing the strongest diagnostic performance. The combination of anti-MSLN and anti-p16 could improve the diagnostic sensitivity. In addition, two autoantibodies to MSLN and Sui1 in PC patients decreased after chemotherapy. Four autoantibodies to MSLN, p16, Sui1, PTEN showed potential diagnostic markers for pancreatic cancer, with anti-MSLN and anti-p16 in best performance. The combination of these two autoantibodies showed the most economical and practical potential. The significance of the reduction of autoantibodies to MSLN and Sui1 in PC patients who were subjected to chemotherapy needs to be further explored.
Keywords: Pancreatic cancer; Autoantibody; Tumor-associated antigens; Biomarkers.
†Equal Contribution: Xiao Wang & Cuipeng Qiu equally contributed to this study.
Citation: Wang X, Qiu C, Qin J, Zhang JZ, Yu B, et al. Evaluation of multiple autoantibodies to tumor-associated antigens as potential diagnostic markers for pancreatic cancer. J Gastroenterol Res Pract. 2024; 4(4): 1193.
Introduction
Pancreatic Cancer (PC) is the seventh leading cause of cancer death at 4.7% worldwide [1]. Moreover, it is a highly lethal malignancy with less than 10% of a five-year survival rate. The poor prognosis of PC is attributed to the fast progression, early metastasis, lack of dependable biomarkers for early detection, and the fact that it is asymptomatic [2,3]. CA19.9, as a tumorspecific antigen, is the most commonly used tumor biomarker for the detection of pancreatic cancer [4]. However, an elevated expression of CA19.9 also appears in other types of gastrointestinal cancers and various benign diseases such as pancreatitis and is thus not specific for pancreatic cancer [5]. The novel circulating biomarkers including serological signatures, autoantibodies, epigenetic markers, circulating tumor cells and microRNAs were demonstrated to be used as potential tools for the screening of precursors and early stage Pancreatic Ductal Adenocarcinoma (PDAC), but they need to be practiced in clinical application [6].
Given the fact that autoantibody, as one of novel circulating biomarkers, is produced accompanying the development of cancer, the autoantibody is called Tumor Associated Autoantibody (TAAb) [7]. Elevation of autoantibodies occurs before the corresponding antigen could be detected in serum, and it acts as biological amplifiers yielding more molecules and increasing the detectable signal through the antigen-antibody reaction [8,9]. This gives the potential for autoantibodies to be used as biomarkers for tumor diagnosis or prognosis [10]. Many autoantibodies have been detected in patients with various types of cancer including PC and identified as potential biomarkers for the diagnosis of these tumors [2,9]. The mechanisms by which autoantibodies are produced with the development of cancer are complex and difficult to understand. The immune system may initate immunologic processes causing autoantibody production in response to mutations, overexpression and modification of proteins, altered antigen folding, aberrant degradation, and so on [11]. Tumor is a unique molecular entity originally from malignant transformation of normal cells, and this transformation process is driven by mutations in multiple genes [12]. Different tumors are caused by mutations in not the same genes, involving different numbers of mutated genes. Tomasetti reported that three driver gene mutations are required for the development of some common cancer types such as lung and colorectal cancer [13]. These previous findings suggested that tumorigenesis process involve multiple genes, and the protein encoded by a single mutated gene or autoantibody corresponding to a single target protein as a tumor biomarker is not effective enough to detect cancer due to a low positive rate in most cases. Additionally, tumors are highly heterogeneous even for a single type of cancer [14]. Therefore, the development of panels of multiple autoantibodies against a variety of Tumor Associated Antigens (TAAs) may provide better sensitivity and specificity, making this approach more feasible for use in immunodiagnosis of cancer [15]. Moreover, a growing number of studies employ combination of multiple autoantibodies, and this strategy does increase the sensitivity of cancer detection [16].
In this study, autoantibodies to nine proteins TAAs including Guanine Nucleotide-Binding Protein Subunit Alpha-11 (GNA11), Mesothelin (MSLN), Guanine Nucleotide Binding Protein, Alpha Stimulating (GNAS), CCAAT/Enhancer-Binding Protein Alpha (CEBPA), Murine Double Minute 2 (MDM2), Cyclin-Dependent Kinase Inhibitor 2A (CDKN2A or P16), eukaryotic translation initiation factor 1 ( eIF1 or Sui1), nucleobindin (Calnuc), Phosphatase and Tensin homolog (PTEN) which were previously studied in other types of cancer [17-22] were detected by Enzyme-Linked Immunosorbent Assay (ELISA) in serum samples from pancreatic cancer patients and normal controls, as well as serum samples collected before and after chemotherapy, with the following objectives: (1) whether the autoantibodies corresponding to the nine target proteins have positive reactions in PC patients; (2) the evaluation of the performance of individual autoantibodies and the combination of multiple autoantibodies in the detection of PC; (3) the observation of dynamic changes of the autoantibodies in PC patients before and after chemotherapy.
Materials and methods
Patients and samples
In the study, 33 serum samples from patients with Pancreatic Cancer (PC) and 45 serum samples from normal controls were obtained from the serum bank of Cancer Autoimmunity Research Laboratory at the University of Texas at El Paso (UTEP). The PC patients without surgical resection of tumors underwent treatment with chemotherapy. Sera were collected before and after chemotherapy. Of 33 PC patients, 16(48.5%) were male, and 17(51.5%) were female. Mean age was 63±9 years (range, 44-82 years). Of 45 normal control sera, 13(28.9%) were male, and 32(71.1%) were female. Mean age was 51±16 years (range, 28-82 years). Normal controls had no obvious evidence of malignancy and autoimmune diseases. Written informed consent has been obtained from all participants. The study was approved by the Institutional Review Board of University of Texas at El Paso.
Recombinant proteins and ELISA
All serum samples were detected by ELISA for autoantibodies to nine recombinant proteins GNA11, MSLN, GNAS, CEBPA, MDM2, P16, Sui1, Calnuc, PTEN. The recombinant proteins of MSLN, GNA11, CEBPA and PTEN were purchased from LD Biopharma Inc (San Diego, CA, USA), GNAS recombinant protein was purchased from Avive Systems Biology (USA), and the fourth rest recombinant proteins were purified by our research team members in our laboratory. The full length of p16 cDNA was amplified by RT-PCR from human HeLa cells, and was subcloned into the pGEX vector expressing p16 with Glutathione S Transferase (GST) fusion. The GST gene fusion system was used for the expression and purification of p16 recombinant protein. The full-length cDNAs of Sui1 and Calnuc obtained from PCR were subcloned into the pET28 expression vector producing a fusion protein with N-terminal 6× histidine and T7 epitope tags. MDM2 construct pGEX 4T MDM2 WT (plasmid ID: 16237). The recombinant proteins were expressed in E. coli BL21 (DE3) and purified using nickel column chromatography. The protocol was performed as described (Qiagen Inc., Valencia, CA). The purified recombinant proteins were examined by SDS-PAGE. Nine Purified recombinant proteins were diluted in Phosphate-Buffered saline (PBS) to a final concentration of 1.0 μg/ml for coating onto a 96 well microtiter plate (Fisher Scientific LLC, Denver, CO, USA). Human sera diluted at 1:200 were incubated in the antigen-coated wells. Horseradish peroxidase (HRP)-conjugated goat anti-human IgG (Invitrogen, Frederick, MD, USA) and the substrate 2, 2′-azino-bis (3-ethylbenzthiazoline-6-sulfonic acid) diammonium salt (Alfa Aesar, Ward Hill, MA, USA) were used as detecting reagents. Detailed procedure was seen in previous study [23]. The Optical Density (OD) value of each well was read at 405 nm.
Statistical analysis
Receiver Operating Characteristic (ROC) curves and the Area Under the ROC Curve (AUC) with sensitivity and specificity together were used to evaluate the diagnostic value of each autoantibody. The cut-off value was defined as the corresponding point of the largest Youden index, while the minimum specificity is more than 90.0% for data analysis. Non-parametric Mann– Whitney U test and Pearson Chi-square test were used for the significance analysis in level and frequency among two groups. The Wilcoxon signed-ranks test was applied for the comparison of autoantibodies in PC patients before and after chemotherapy.
Results
Autoantibody response to nine TAAs in PC patients
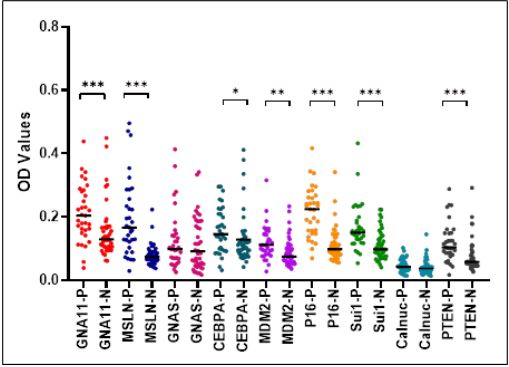
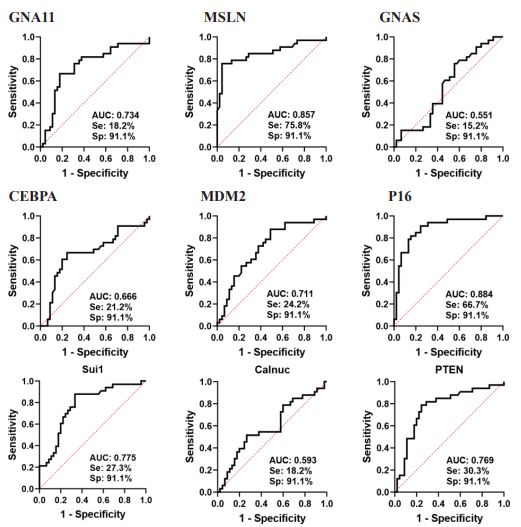
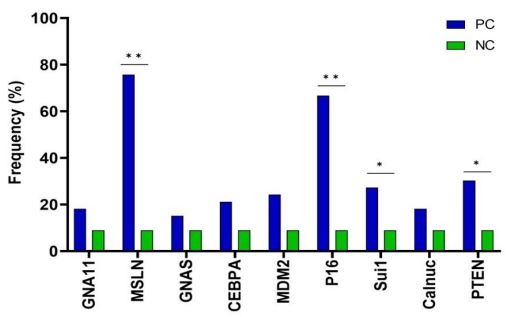
To explore the possibility of the nine individual autoantibodies as potential biomarkers in PC, Enzyme-Linked Immunosorbent Assay (ELISA) was performed to evaluate autoantibodies against GNA11, MSLN, GNAS, CEBPA, MDM2, p16, Sui1, Calnuc and PTEN in 33 sera from PC patients and 45 sera from normal controls. As shown in the light scatter plots in Figure 1, positive reactivity of autoantibodies to all TAAs except CEBPA and Calnuc in PC patients was significantly stronger than that in normal controls. Based on ROC curve analysis showing in Figure 2, the AUCs of the seven autoantibodies ranged from 0.666 to 0.884. Autoantibodies to p16 and MSLN showed the best diagnostic performance with AUC at 0.884 and 0.857, respectively. While the minimum specificity was set at 91.1%, the corresponding point of the largest Youden index was defined as the cutoff value in which the frequency of autoantibodies to nine TAAs in PC patients was ranged from 15.2% to 75.8%. As shown in Figure 3, the frequencies of four autoantibodies to MSLN, p16, Sui1 and PTEN in PC patients were significantly higher than those in normal controls (P<0.05). Among the four TAAbs, anti-MSLN and anti-p16 yielded the highest positive rates of 75.8% and 66.7% in PC patients (P<0.05), respectively.
Combination of autoantibodies
The combination of multiple auto antibodies might acquire higher sensitivity for the detection of cancer. Therefore, in order to understand if the combination of multiple autoantibodies could enhance their detection sensitivity in PC, we tried to combine the four autoantibodies that were significantly different from normal controls in both serum level and positive rate. With the successive addition of TAAs to a final total of four antigens, there was a stepwise increase in positive autoantibody reactions reaching a sensitivity of 81.8% and a specificity of 77.8% in PC patients (Table 1). Taking into account the overall performance, the combination of anti- MSLN and anti-p16 autoantibodies was an optimal panel by reaching the sensitivity of 78.8% and specificity of 82.2%, with an increase compared to a single autoantibody alone. The Positive Predictive Value (PPV), Negative Predictive Value (NPV) and Youden’sindex for this combination were 83.5%, 79.9% and 0.6, respectively.
Table 1: The performance of a panel with sequential addition of antigens.
| Antigens 1 MSLN |
Se 75.8 |
Sp 91.1 |
YI 0.7 |
FP 8.9 |
FN 25.0 |
PPV 89.4 |
NPV 78.5 |
LR+ 8.4 |
LR- 0.3 |
|---|---|---|---|---|---|---|---|---|---|
| 2 MSLN or P16 | 78.8 | 84.4 | 0.6 | 15.6 | 21.2 | 83.5 | 79.9 | 5.1 | 0.3 |
| 3 MSLN or P16 or PTEN | 78.8 | 82.2 | 0.6 | 17.8 | 21.2 | 81.6 | 79.5 | 4.4 | 0.3 |
| 4MSLN or P16 or PTEN or Sui1 | 81.8 | 77.8 | 0.6 | 22.2 | 18.2 | 78.7 | 81.0 | 3.7 | 0.2 |
Se: Sensitivity = positive/Number of HCC cancer.
Sp: Specificity = positive/Number of NC.
FP: False Positive = 1-Sp.
FN: False Negative = 1-Se.
PPV: Positive Predictive Value = Se/(Se + FP).
NPV: Negative Predictive Value = Sp/(FN + Sp).
LR+: Positive likelihood Ratio = Se/(1-Sp).
LR−: Negative likelihood Ratio = (1-Se)/Sp.
Nine autoantibody detection before and after chemotherapy
Nine autoantibodies to GNA11, MSLN, GNAS, CEBPA, MDM2, P16, Sui1, Calnuc, PTEN were also evaluated in 66 serial sera from 33 PC patients who underwent chemotherapy in this study. The results showed that seven autoantibodies in serum level showed a downward trend and only two of them in serum level significantly decreased in one month after chemotherapy, which were anti-MSLN and anti-Sui1 (P<0.001, Table 2). Figure 4 displayed the changing trend of autoantibodies to MSLN and Sui1 in PC patients before and after chemotherapy. Autoantibodies to MDM2 and p16 exhibited an upward tread without significant difference before and after chemotherapy.
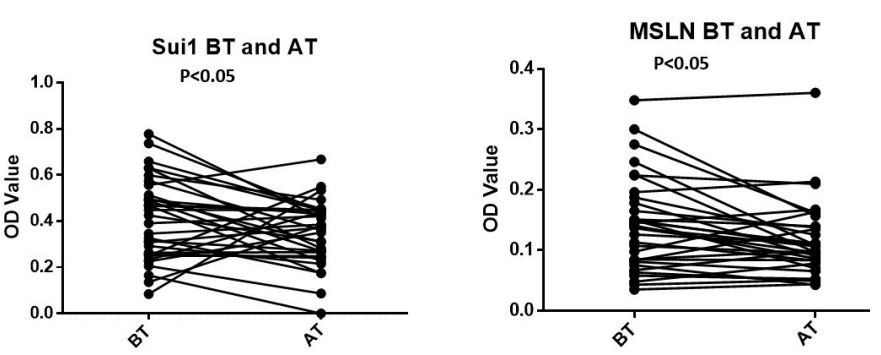
BT: Before Treatment; AT: After Treatment.
Table 2: Comparison before and after chemotherapy for 9 autoantibodies.
| Before chemotherapy | After chemotherapy | ||||||
|---|---|---|---|---|---|---|---|
| NO. of samples | Median | SD | NO. of samples | Median | SD | P Value | |
| GNA11 | 33 | 0.439 | 0.269 | 33 | 0.408 | 0.257 | 0.823 |
| MSLN | 33 | 0.138 | 0.077 | 33 | 0.1 | 0.062 | 0.011 |
| GNAS | 33 | 0.334 | 0.143 | 33 | 0.309 | 0.226 | 0.348 |
| CE-BPA | 33 | 0.198 | 0.118 | 33 | 0.186 | 0.152 | 0.195 |
| MDM2 | 33 | 0.305 | 0.256 | 33 | 0.412 | 0.194 | 0.755 |
| p16 | 33 | 0.112 | 0.106 | 33 | 0.131 | 0.101 | 0.611 |
| Sui1 | 33 | 0.426 | 0.178 | 33 | 0.372 | 0.149 | 0.048 |
| Calnuc | 33 | 0.205 | 0.12 | 33 | 0.184 | 0.101 | 0.175 |
| PTEN | 33 | 0.248 | 0.161 | 33 | 0.225 | 0.118 |
Discussion
In view of the low incidence of pancreatic cancer in the whole population, difficulty in early detection and effective treatment, and limited survival time, it is not easy to obtain a large size of serum samples from patients with pancreatic cancer. In this study, nine autoantibodies in sera from 33 patients and 45 normal controls were evaluated. Seven autoantibodies (GNA11, MSLN, CEBPA, MDM2, p16, Sui1 and PTEN) in level in pancreatic cancer group were higher than those in the normal control group, and the frequencies of the 4 autoantibodies (MSLN, p16, Sui1 and PTEN) were significantly higher in the pancreatic cancer group than those in the normal control group. These four autoantibodies also displayed the most diagnostic efficacy reflected by AUC, which is consistent with their positive rates. Among the four identified TAAbs, anti-MSLN and anti-p16 showed the best diagnostic performance with 75.8% of frequency and 0.857 of AUC, 66.7% of frequency and 0.884 of AUC alone, respectively. When combined the four autoantibodies to MSLN, p16, Sui1 and PTEN as a panel, the sensitivity of the combination did not increase a lot, which suggests that these four PC-related antigens corresponding to TAAbs included in the panel may highly be correlated in the role of triggering the production of autoantibodies. The detection of nine autoantibodies in serial sera from PC patients before and after chemotherapy was performed for exploring the change of TAAbs in level, the result demonstrated that anti-MSLN and anti-Sui1 autoantibodies significantly decreased in PC patients after chemotherapy. The development and progression of pancreatic cancer over a long time period is closely associated with the activation of oncogenes, inactivation of tumor suppressor genes, and so on [6]. Among the Tumor Associated Antigens (TAAs) corresponding to the autoantibodies detected above, there are four proteins encoded by oncogenes (MSLN, GNS11, GNAS and MDM2), four proteins encoded by tumor suppressor genes (CEBPA, p16, Sui1 and PTEN), one protein which is a tumor-associated antigen is encoded by Calnuc geneand its genetic property has not yet been characterized. Mesothelin (MSLN) is highly expressed in some solid tumors, including Ovarian Cancer (OC), PC, mesothelioma, and plays an important role in cell adhesion, tumor progression, metastasis, and chemo-resistance [24]. The high expression of MSLN in OC tissues and elevation of MSLN in OC patient sera endow it as a relatively specific marker for the diagnosis of ovarian cancer [25]. In pancreatic cancer, MSLN protein overexpression leads to PC cell proliferation and tumor progression [26]. However, the serum level of MSLN is not consistent with tumor MSLN. MSLN protein is highly expressed in most PC tissues, not elevated in PC patient sera [27]. Guanine nucleotide-binding protein subunit alpha-11 (GNA11) functions as modulators or transducers in various transmembrane signaling systems. GNA11 and GNAQ gene mutations are involved in the process of carcinogenesis by resulting in the activation of downstream signaling pathways [28]. GNAS is a member of the same family as GNA11, its mutations are found in a wider range of malignancies [29]. GNAS are more frequently mutated in welldifferentiated pancreatic tumors than in poorly differentiated pancreatic cancer [30]. As a transcriptional activator, Murine Double Minute 2 (MDM2) functionally cooperates with Numb and p53 and is involved in the development and progression of PC [31]. CCAAT Enhancer Binding Protein Alpha (CEBPA) cooperates with KDM6B and plays an important role in Pancreatic Ductal Adenocarcinoma (PDAC) phenotype [32]. p16/CDKN2 (Cyclin-Dependent Kinase Inhibitor 2) as a tumor suppressor gene plays an important role in the inhibition of the cell cycle and is involved in the development of pancreatic intraepithelial neoplasia [33]. The loss or reduced expression of p16 protein was observed in 80% of PC patients [34]. Moreover, a study indicated that the expression of p16 gene in pancreatic cancer tissue was negatively correlated with differentiation degree and clinical stage [35]. Sui1/ Eif1 (Eukaryotic translation initiation factor) maintains cell proliferation and cell cycle progression [36]. The down-regulation of Sui1 protein observed in PDAC tissues suggested the important role of Sui1 in the development of PDAC [37]. Phosphatase and Tensin Homolog (PTEN) generally prevents tumorigenesis through multiple signaling pathways including PI3K/AKT pathway which is closely associated to the tumorigenesis and progression of PC [38]. As one of the most frequently mutated or deleted genes in human cancers, PTEN mutation and deletion activate this pathway, leading to cancerization of the cells [39]. As a calcium binding protein, downregulation of Calnuc was associated with short survival of PDAC patients. Up-regulation of Calnuc can suppress proliferation and promote the anti-tumor effects of gemcitabine in pancreatic cancer cells in vitro and in vivo [40]. All targeted proteins except GNA11 included in this study were indicated to be closely related to the development of PC. As far as we know, except MSLN protein, the levels of the other 8 targeted proteins in serum from PC patients have not been reported. Moreover, the MSLN protein was only increased in the PC tissues, rarely elevated in sera from PC patients. Therefore, the MSLN protein cannot be used as a marker for real detection of PC. Even though some targeted proteins or their corresponding genes are differentially expressed between PC tissues and normal or precancerous tissues, they are still not of much value in practical operation due to difficulty in obtaining PC tissue samples. However, if autoantibodies against these target proteins are significantly elevated in the serum of patients with pancreatic cancer, they have a relatively large application value for the diagnosis of PC. Among the nine autoantibodies detected in our study, there are four autoantibodies with positive response to MSLN, p16, Sui1 and PTEN in PC patients reflected in both serum level and frequency. The highest autoantibody responses to MSLN and p16 were observed with 75.8% and 66.7% of frequencies in PC patients across 4 TAAbs. MSLN is a well-characterized ovarian cancer antigen, and the elevation of its corresponding autoantibody was reported in the most of patients with Ovarian Cancer (OC), suggesting both MSLN protein and its corresponding autoantibody are specific markers for OC [41]. Anti-MSLN antibody in combination format has been used for the immunotherapy in a variety of mesothelin-expressing solid tumors [42]. Moreover, there are many reports on this topic. However, there are few reports on the use of autoantibody to MSLN as a potential diagnostic marker of pancreatic cancer. Such a high sensitivity of autoantibody to MSLN (75.8%) in PC patients is reported for the first time in this study. Also, anti-MSLN autoantibody showed high AUC value at 0.857 to discriminate PC from controls. As a single marker, autoantibody to MSLN displayed the greatest potential to become the most attractive candidate to enter the optimal combination developed in the future for PC detection. The elevation of autoantibody to p16 has been reported as either early detection or prognostic marker in multiple malignancies such as breast, esophageal, nasopharyngeal, esophageal and hepatocellular carcinoma [43], rarely in PC. One study with multiple TAAbs including anti-p16 in PC patents indicated that autoantibody to p16 showed the highest sensitivity (30.4%) in PC patients across 6 TAAbs ( P53, p16, p62, Survivin, IMP1) [16], in which, the performance of anti-p16 is similar to that in our current study. Anti-Sui1 is [23,9]the most frequently detected and evaluated autoantibody in HCC and Okada’s study showed the highest sensitivity for the detection of HCC among six autoantibodies [21]. However, no report has been seen in PC, thus autoantibody to Sui1 is a newly discovered marker for the detection of PC. In Kuemmel’s study, the autoantibody reactivity to PTEN in lung cancer patients was associated with increased survival and lower frequency of metastasis, thus seemed to be a prognostic marker [44]. Elevation of autoantibody to PTEN was also reported in esophageal and gastric cancer [45,46], The occurrence of anti-PTEN has not been reported in PC patients. This study investigated for the first time the occurrence and prevalence of anti-PTEN in PC patients. 30.3% of PC patients had positive serological response to PTEN, suggesting that it may be a potential biomarker in the detection of PC.
Since the development and occurrence of cancer is a complex process involving multiple steps and factors, no single marker can give enough high sensitivity and specificity to completely distinguish cancer patients from normal controls [4,5]. Increasing researches focus on the discovery of combination of multiple markers with greater efficacy and clinical utility [2]. Many combinations consisting of multiple autoantibodies were discovered for PC diagnosis, a representative combination including 6 autoantibodies to p53, p16, p62, survivin, Koc and IMP1 in PC enhanced their individual sensitivity (ranging from 14.7% to 30.4%) to 60.9% at specificity of 87.0% [16]. Two newly discovered combinations of 4 TAAbs with AUC of a range from 0.76 to 0.80 in Zhuang’s study also enhanced their diagnostic performance reflected by increasing AUC at 0.82 in discriminating PC patients from normal controls [47]. In our current study, the individual sensitivity of 4 differentially expressed TAAbs varied from 27.3 to 75.8%. When they were combined in different combinations with the successive addition of TAAbs one by one to a final total of four TAAbs, there was a stepwise increase of sensitivity reaching different high values. From an economic and practical point of view, the combination of anti-MSLN and anti-p16 with sensitivity of 78.8% and specificity of 84.4% was found to be the best one across three different combinations. A previous study has shown that the dynamic changes of serum autoantibodies can reflect the burden and status of tumor in patients [48]. Hardy-Werbin M., etal. mentioned a concept that the removal of immunogen is linked with a decrease in autoantibody level, moreover, his study found that the cancer patient whose autoantibody titer decreased after treatment, had longer overall survival, suggesting that the autoantibody may be considered as prognostic markers [49]. In the present study, all 33 pancreatic cancer patients were subjected to chemotherapy. To explore the changes of nine autoantibody levels in these PC patients after chemotherapy, pair-wise analysis were performed. Of nine autoantibodies tested in PC patients, anti-MSLN and anti-Sui1 in serum levels significantly decreased after chemotherapy, showing a similar changing trend as those of autoantibodies in both studies above. This may be due to some biological processes triggered by chemotherapy, killing some tumor cells that produce and release antigenic proteins or some immune cells that secrete autoantibodies in the tumor microenvironment. This finding also suggests that these two autoantibodies might be related to the prognosis of PC patients.
Conclusion
In summary, autoantibody-positive reactions to MSLN, p16, Sui1, and PTEN were detected in PC patients, and anti-MSLN and anti-p16 with the best diagnostic performance may become the candidate members of the best combination to be established in the future. The significance of the reduction of autoantibodies to MSLN and Sui1 in PC patients after chemotherapy might be worthy of further study with a large sample size.
Declarations
Author contributions: J.Y.Z and B.Y. planned the study and revised the manuscript. X.W. conducted the study and mainly drafted the manuscript. C.Q. conducted the study and mainly analyzed data. J.Q. started the testing and provided the preliminary data. B.W. helped with data analysis. Xiao Wang and Cuipeng Qiu equally contribute to this study. Dr. Baofa Yu is an adjunct faculty member at UTEP
Funding: This work was partially supported by Border Biomedical Research Center (BBRC) at UTEP.
Conflicts of interest: No potential conflicts of interest were disclosed.
References
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A cancer journal for clinicians. 2021; 71: 209-249.
- Dumstrei K, Chen H and Brenner H. A systematic review of serum autoantibodies as biomarkers for pancreatic cancer detection. Oncotarget 2016; 7: 11151.
- Mizrahi JD, Surana R, Valle JW, et al. Pancreatic cancer. The Lancet. 2020; 395: 2008-2020.
- Kriz D, Ansari D and Andersson R. Potential biomarkers for early detection of pancreatic ductal adenocarcinoma. Clinical and Translational Oncology. 2020; 22: 2170-2174.
- Kaur S, Baine MJ, Jain M, et al. Early diagnosis of pancreatic cancer: challenges and new developments. Biomarkers in medicine. 2012; 6: 597-612.
- He X-Y and Yuan Y-Z. Advances in pancreatic cancer research: moving towards early detection. World journal of gastroenterology: WJG. 2014; 20: 11241.
- Ghassem-Zadeh S, Hufnagel K, Bauer A, et al. Novel autoantibody signatures in sera of patients with pancreatic cancer, chronic pancreatitis and autoimmune pancreatitis: a protein microarray profiling approach. International journal of molecular sciences. 2020; 21: 2403.
- Burford B, Gentry-Maharaj A, Graham R, et al. Autoantibodies to MUC1 glycopeptides cannot be used as a screening assay for early detection of breast, ovarian, lung or pancreatic cancer. British journal of cancer. 2013; 108: 2045- 2055.
- Wu J, Li X, Song W, et al. The roles and applications of autoantibodies in progression, diagnosis, treatment and prognosis of human malignant tumours. Autoimmunity Reviews. 2017; 16: 1270-1281.
- Järås K and Anderson K. Autoantibodies in cancer: prognostic biomarkers and immune activation. Expert review of proteomics. 2011; 8: 577-589.
- Brindl N, Boekhoff H, Bauer AS, et al. Use of Autoreactive Antibodies in Blood of Patients with Pancreatic Intraductal Papillary Mucinous Neoplasms (IPMN) for Grade Distinction and Detection of Malignancy. Cancers. 2022; 14: 3562.
- Van Nistelrooij AMJ, van Marion R, Biermann K, et al. Early onset esophageal adenocarcinoma: a distinct molecular entity? Oncoscience. 2016; 3: 42.
- Tomasetti C, Marchionni L, Nowak MA, et al. Only three driver gene mutations are required for the development of lung and colorectal cancers. Proceedings of the National Academy of Sciences. 2015; 112: 118- 123.
- Tan EM and Zhang J. Autoantibodies to tumor ‐associated antigens: reporters from the immune system. Immunological reviews. 2008; 222: 328-340.
- Monroy-Iglesias MJ, Crescioli S, Beckmann K, et al. Antibodies as biomarkers for cancer risk: a systematic review. Clinical and Experimental Immunology. 2022; 209: 46-63.
- Li J, Wang LJ, Ying X, et al. Immunodiagnostic value of combined detection of autoantibodies to tumor‐ associated antigens as biomarkers in pancreatic cancer. Scandinavian journal of immunology. 2012; 75: 342-349.
- Wang K, Li M, Qin J, et al. Serological biomarkers for early detection of hepatocellular carcinoma: a focus on autoantibodies against tumor-associated antigens encoded by cancer driver genes. Cancers. 2020; 12: 1271.
- Luborsky JL, Yu Y, Edassery SL, et al. Autoantibodies to mesothelin in infertility. Cancer epidemiology, biomarkers & prevention. 2011; 20: 1970-1978.
- Qiu C, Wang B, Wang P, et al. Identification of novel autoantibody signatures and evaluation of a panel of autoantibodies in breast cancer. Cancer Science. 2021; 112: 3388-3400.
- Dai L, Tsay J-CJ, Li J, et al. Autoantibodies against tumor-associated antigens in the early detection of lung cancer. Lung cancer. 2016; 99: 172-179.
- Okada R, Otsuka Y, Yokosuka O, et al. Six autoantibodies as potential differential biomarkers of hepatocellular carcinoma vs. liver cirrhosis and chronic hepatitis: A prospective multi‑institutional study. Oncology Letters. 2022; 24: 1- 9.
- Chen Y, Lin P, Qiu S, et al. Autoantibodies to Ca2+ binding protein Calnuc is a potential marker in colon cancer detection. International journal of oncology. 2007; 30: 1137-1144.
- Qiu C, Ma Y, Wang B, et al. Autoantibodies to PAX5, PTCH1, and GNA11 as Serological Biomarkers in the Detection of Hepatocellular Carcinoma in Hispanic Americans. International Journal of Molecular Sciences. 2023; 24: 3721.
- Shen J, Sun X, Zhou J. Insights into the role of mesothelin as a diagnostic and therapeutic target in ovarian carcinoma. Frontiers in Oncology. 2020; 10: 1263.
- Yu Y, Edassery SL, Barua A, et al. The hen model of human ovarian cancer develops anti-mesothelin autoantibodies in response to mesothelin expressing tumors. Journal of Ovarian Research. 2011; 4: 1-9.
- Le K, Wang J, Zhang T, et al. Overexpression of mesothelin in pancreatic ductal adenocarcinoma (PDAC). International Journal of Medical Sciences. 2020; 17: 422.
- Zhang X, Yu Y, Peer CJ, et al. Low serum mesothelin in pancreatic cancer patients results from retention of shed mesothelin in the tumor microenvironment. Translational Oncology. 2022; 21: 101440.
- Silva-Rodríguez P, Fernández-Díaz D, Bande M, et al. GNAQ and GNA11 genes: A comprehensive review on oncogenesis, prognosis and therapeutic opportunities in uveal melanoma. Cancers. 2022; 14: 3066.
- Parish AJ, Nguyen V, Goodman AM, et al. GNAS, GNAQ, and GNA11 alterations in patients with diverse cancers. Cancer. 2018; 124: 4080-4089.
- Ohtsuka T, Tomosugi T, Kimura R, et al. Clinical assessment of the GNAS mutation status in patients with intraductal papillary mucinous neoplasm of the pancreas. Surgery today. 2019; 49: 887-893.
- Sheng W, Dong M, Zhou J, et al. Cooperation among Numb, MDM2 and p53 in the development and progression of pancreatic cancer. Cell and tissue research. 2013; 354: 521-532.
- Yamamoto K, Tateishi K, Kudo Y, et al. Loss of histone demethylase KDM6B enhances aggressiveness of Pancreatic cancer through downregulation of C/EBPα. Carcinogenesis. 2014; 35: 2404-2414.
- Zińczuk J, Zaręba K, Guzińska-Ustymowicz K, et al. p16, p21, and p53 proteins play an important role in development of pancreatic intraepithelial neoplastic. Irish Journal of Medical Science (1971-). 2018; 187: 629-637.
- Tsiambas E, Karameris A, Gourgiotis S, et al. Simultaneous deregulation of p16 and cyclin D1 genes in pancreatic ductal adenocarcinoma: a combined immunohistochemistry and image analysis study based on tissue microarrays. Journal of BU ON: Official Journal of the Balkan Union of Oncology. 2007; 12: 261-267.
- Mou H, Yu L, Zheng X, et al. p16 gene expression in pancreatic cancer tissue and its importance in diagnosis. Journal of biological regulators and homeostatic agents. 2017; 31: 1043-1047.
- Sehrawat U, Koning F, Ashkenazi S, et al. Cancer-associated eukaryotic translation initiation factor 1A mutants impair Rps3 and Rps10 binding and enhance scanning of cell cycle genes. Molecular and Cellular Biology. 2019; 39: e00441-00418.
- Golob-Schwarzl N, Puchas P, Gogg-Kamerer M, et al. New pancreatic cancer biomarkers eIF1, eIF2D, eIF3C and eIF6 play a major role in translational control in ductal adenocarcinoma. Anticancer Research. 2020; 40: 3109-3118.
- Zhang Q, Li X, Li Y, et al. Expression of the PTEN/FOXO3a/PLZF signalling pathway in pancreatic cancer and its significance in tumourigenesis and progression. Investigational New Drugs. 2020; 38: 321-328.
- Downes CP, Perera N, Ross S, et al. Substrate specificity and acute regulation of the tumour suppressor phosphatase, PTEN. In: Press Ltd. 2007; 69-80
- Hua Y-Q, Zhang K, Sheng J, et al. NUCB1 suppresses growth and shows additive effects with gemcitabine in pancreatic ductal adenocarcinoma via the unfolded protein response. Frontiers in Cell and Developmental Biology. 2021; 9: 641836.
- Hellstrom I, Friedman E, Verch T, et al. Anti-mesothelin antibodies and circulating mesothelin relate to the clinical state in ovarian cancer patients. Cancer Epidemiology Biomarkers & Prevention. 2008; 17: 1520-1526.
- Hassan R, Blumenschein Jr GR, Moore KN, et al. First-in-human, multicenter, phase I dose-escalation and expansion study of anti-mesothelin antibody–drug conjugate anetumab ravtansine in advanced or metastatic solid tumors. Journal of Clinical Oncology. 2020; 38: 1824.
- Looi K, Megliorino R, Shi F-D, et al. Humoral immune response to p16, a cyclin-dependent kinase inhibitor in human malignancies. Oncology reports. 2006; 16: 1105-1110.
- Kuemmel A, Simon P, Breitkreuz A, et al. Humoral immune responses of lung cancer patients against the Transmembrane Phosphatase with TEnsin homology (TPTE). Lung Cancer. 2015; 90: 334-341.
- Sun G, Ye H, Wang X, et al. Identification of novel autoantibodies based on the protein chip encoded by cancer-driving genes in detection of esophageal squamous cell carcinoma. Oncoimmunology. 2020; 9: 1814515.
- Qin J, Wang S, Shi J, et al. Using recursive partitioning approach to select tumor‐associated antigens in immunodiagnosis of gastric adenocarcinoma. Cancer Science. 2019; 110: 1829-1841.
- Zhuang L, Huang C, Ning Z, et al. Circulating tumor‐associated autoantibodies as novel diagnostic biomarkers in pancreatic adenocarcinoma. International Journal of Cancer. 2023; 152: 1013-1024.
- Ladd JJ, Chao T, Johnson MM, et al. Autoantibody Signatures Involving Glycolysis and Splicesome Proteins Precede a Diagnosis of Breast Cancer among Postmenopausal WomenPrediagnostic Breast Cancer Autoantibody Signatures. Cancer research. 2013; 73: 1502-1513.
- Hardy-Werbin M, Arpí O, Taus A, et al. Assessment of neuronal autoantibodies in patients with small cell lung cancer treated with chemotherapy with or without ipilimumab. Oncoimmunology. 2018; 7.