
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Metformin reverses the effect of high glucose on mesenteric artery relaxation in normal rats
Raúl Rojas-Martinez*; Carlos Alberto Zúñiga Cruz; María Esther Ocharan Hernandez
Graduate Studies and Research Section, School of Medicine, National Polytechnic Institute, Plan de San Luis and Díaz Mirón, Santo Tomas neighborhood, Miguel Hidalgo delegation, Mexico City, 11340, Mexico.
*Corresponding Author : Raúl Rojas-Martinez
Graduate Studies and Research Section, School of Medicine, National Polytechnic Institute, Plan de San Luis and
Díaz Mirón, Santo Tomas neighborhood, Miguel Hidalgo
delegation, Mexico City, 11340, Mexico.
Tel: +55-57296300;
Email: rrojasma@ipn.mx
Received : Mar 02, 2024
Accepted : Apr 09, 2024
Published : Apr 16, 2024
Archived : www.jjgastro.com
Copyright : © Rojas-Martinez R (2024).
Abstract
Elevated glucose produces alterations in the cardiovascular system, which affect the health of subjects with these increases, which affect systems such as the gastrointestinal, since the mesenteric arteries play an important role for the proper development of the individual. These diseases are related and cause great morbidity and mortality worldwide. Metformin is a biguanide used to control blood glucose levels. This study assessed the effect of metformin on arterial tension and endothelial function on rat normal mesenteric arteries. Arteries incubated in glucose (30 mM) demonstrated a profoundly impaired endothelium-dependent relaxation to acetylcholine. The treatment with metformin (1 mM) produced the change in the vascular activity, like the control group. These results indicated that the action of metformin in the vascular activity is recovered to normal condition, which is important in patients with diabetes mellitus type 2, already the cardiovascular alterations were presents in these patients. Glucose modified the effect of Nitric oxide synthase and CYTP450, decreasing the production of Nitric Oxide and hyperpolarizing factor, in arteries relaxed with acetylcholine, where metformin reversed to normal conditions. On the other hand, the used of metformin plus indomethacin produced inhibition on metformin, effects inducing a mayor inhibition on the vascular relaxation to acetylcholine. Also, metformin presented a minimum effect on K+ channels, when are inactivated with TEA, recovering of manner partial the action of this channel, increased relaxation effect by acetylcholine. Metformin effect is not due to osmotic control or oxidative stress. An important effect is the use of analgesics such as indomethacin, which produces dysfunction of the vascular endothelium, generating the presence of diseases due to the state of hypertension obtained in the mesenteric arteries, affecting the proper functioning of the gastrointestinal system, decreasing the uptake of nutrients and presenting various diseases.
Keywords: Metformin; Mesenteric arteries; Endothelium vascular; Glucose; Diabetes.
Citation: Rojas-Martinez R, Cruz CAZ, Hernandez MEO. Metformin reverses the effect of high glucose on mesenteric artery relaxation in normal rats. J Gastroenterol Res Pract. 2024; 4(3): 1191.
Introduction
Vascular diseases are the mayor cause of mobility and mortality in patients with high glucose, as patients with type 2 diabetes mellitus (non-insulin-dependent Diabetes Mellitus, DM2), but is not fully explained by the presence of traditional cardiovascular risk factors [1-37]. In this sense, the interaction of multiple metabolic, genetic, and other factors results in microvascular complications during diabetes [38-42]. There is variability in the susceptibility to microvasculature disease which in individual patients, cannot be predicted from the glycemic pattern [21,37]. Studies in vitro determinate the effects of glucose on dependents responses of endothelium and the productions of vasoactive prostanoids realized in aortas of normal rabbits in high glucose (25 and 44 mM for 6 and 12 hrs), in comparison with control group (glucose 25 mM or 11 mM), these effects produced dysfunctions of muscarinic receptors that produced dependent relaxation of endothelium, then producing increase in the vasoconstrictors prostanoids for activations of the PKC. In this sense, mannitol as an osmolar control, produced a similar relaxation to arteries relaxed with acetylcholine with a normal concentration of glucose [39]. Seven days of exposition in high glucose (25 mM); on endothelial coronary cells of human produced the decrease of nitric oxide production. One-hour incubation of aorta rings of control group with high glucose (30 mM), produced decrease of nitric oxide production, alternated the activity of the GMPc, with consequent decrease of vasorelaxation [38]. A variety of oral active antihyperglycemic agents are frequently used to help the manager of intolerance and resistance of glucose of patients with type 2 diabetes mellitus. Metformin, a biguanide, has been shown to improve insulin resistance and lower blood pressure in hypertensive patients [1-7]. In addition, metformin improves lipid profiles and lowers blood pressure in patients and animal models with impaired glucose tolerance and type 2 diabetes mellitus [1-3,5,15]. Metformin has also been shown to have direct vascular effects. Thus, it is currently not clear whether the hypotensive effect of metformin is due to a direct vascular effect, its ability to improve insulin sensitivity, its ability to improve lipids, or a combination of mechanisms.
The aim of the present study was: (i) to assess the hypotensive effect of metformin on the vasorelaxation on rat mesentery arteries, incubated with high concentrations of glucose; and (ii) to investigate the possible mechanisms involved.
Materials and methods
All procedures and handling of the animals were om accordance with Mexican Federal Regulations for animal Experimentation and Care (NOM-’62-ZOO-1999, Ministry of agriculture, Mexico). Adult (250-300 g) male Sprague Dawley rats were killer by asphyxia with CO2 . Then, the mesenteric arteries were removed and rapidly placed in Krebs-Ringer solution. Of the following composition (mM): NaCl (118.3), KCl (4.7), CaCl2 (2.5), MgSO4 (1.2), KH2 PO4 (1.2), NaHCO3 (25), D-glucose (11.1), Ethylenediamine-Tetra-Acetic Acid disodium salt (EDTA) (0.026). A section of the third branch mesenteric artery (internal diameter of approximately 250 µm) was dissected, and cleaned of fat, blood and connective tissue under a light microscope and horizontally mounted in organ bath chambers containing 10 mL Krebs solution at 37°C. The solution was continuously bubbled with 95% O2 -5% CO2 , resulting in a pH of 7.4. Changes in arterial tension were recorder isometrically by a force-displacement transducer (Model 500A with software Myosight version 1.21 (JP Trading Co., Aarhus, Denmark). The dates were registered on a computer and were reported as changes in the tension. Arteries were incubated for 30 min with glucose at 5.8 mM for the control group or with 30 mM in the high glucose group, before the arteries were contracted with phenylephrine (1 M) and relaxed with Ach (10-9 to 10-4 M).
Experimental protocols
In separate groups of experiments, the arteries were incubated for 30 minutes with solutions containing normal (5.8 mM) or high concentration (30 mM) of glucose, in presence or absence of metformin (I µM). The mesenteric arteries were pre-contracted with Noradrenaline (NE, 1 µM), and the effect of Acetylcholine (Ach, 10-9 to 10-4 M) was determinate. Doseresponses curve to the effects of endothelium-dependent (acetylcholine, Ach) and independent (Sodium Nitroprusside, SNP) agents, were constructed. Additional experiments were performed in the presence of L-NAME (competitive inhibitor of nitric oxide synthase, 10-6 M); TEA (Tetraethylammonium, nonspecific K+ channel inhibitor, 10 mM); clotrimazole (inhibitor of the CYTP450, 10-6M) indomethacin (inhibitor of the COX2, 10-5 M); or losartan AT1 receptor inhibitor, 10-6 M), simultaneously with high glucose (30 mM) and metformin (1 µM). Additional experiments were realized with ascorbic acid (85 µM), to determinate the effect of oxidative stress, or sucrose (30 mM), as osmotic control, in comparison with high glucose (30 mM).
Glucose concentrations
The glucose concentrations used in the present study corresponding to previous reports [31,38], where were proved 30 mM of glucose for 1 hour. These concentrations are presents in patients with DM2. On the other hand, to determinate the possible mechanism of action of metformin, we needed high concentrations of glucose. We realized determinations with glucose 10 and 30 mM at 30 and 60 minutes of incubation, where we observed that the mayor effects was with glucose 30 mM at 30 minutes of incubation (dates not shown).
Drugs
All chemicals were obtained from Sigma (St. Louis, MO, USA). Metformin was kindly donated by Merck laboratories, acetylcholine and D-glucose from Sigma. The Chemicals were prepared as stock solutions dissolved in control solution. Fresh solutions were prepared for each experiment. The doses of all compounds refer to their free base.
Statistical analysis of data
All values obtained represent the mean ± S.E.M. In all the experiments, n equal the number of rats from which the mesenteric segments were obtained. The statistical comparations were made by one-way ANOVA and a Turkey post-hoc test to determinate significant differences. All cases a p value ≤ 0.05 was considerate statistically significant.
Effects of glucose in relaxation
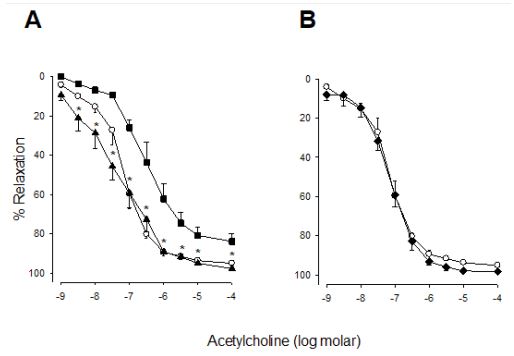
Initial levels of vascular tone were similar in all experimental groups (relaxation of Ach (10-9 to 10-4 M), control group. On Figure 1A the control group as the baseline values are showed. The effects of high glucose (30 mM), produced alteration on the vasorelaxation to acetylcholine (10-9 to 10-4 M), decrease of 20% with respect to control group (p<0.5). On the other hand, the time of incubation with high glucose 30 minutes, produced differences with respect to control group, decrease of 20% in the relaxation (p<0.05).
Effects of metformin
The effects of metformin on the arterial vasorelaxation incubate with high glucose (30 mM for 30 minutes), is shows on the Figure 1A, we observed that metformin decreased the high glucose effect, increased the relaxation at Ach (10-9 to 10-4 M) at normal values. Metformin did not modify vasorelaxation by Ach, in arteries incubated with normal glucose (5.8 mM) (Figure 1B). Metformin (10-9 to 10-4 M) did not modify vasorelaxation with respect at control group (data not shown).
Effect of endothelium
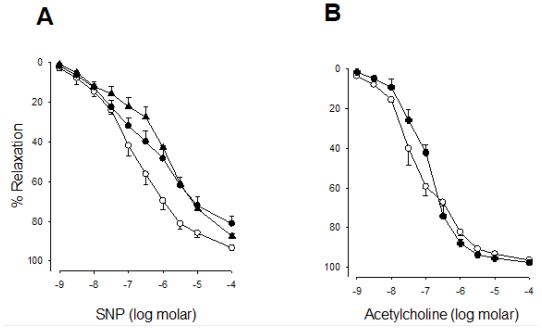
Figure 2A shows the participation of vascular endothelium on metformin effect. The arteries without endothelium produced a similar effect of high glucose (30 mM), and there were no differences with sodium nitroprusiate (10-9 to 10-4 M) relaxation. Sucrose (30 mM) did not modify vasorelaxation by Ach (10-9 to 10-4 M), without differences with respect to control group (glucose 5.8 mM) (Figure 2B).
Effect of L-NAME, losartan or indomethacin
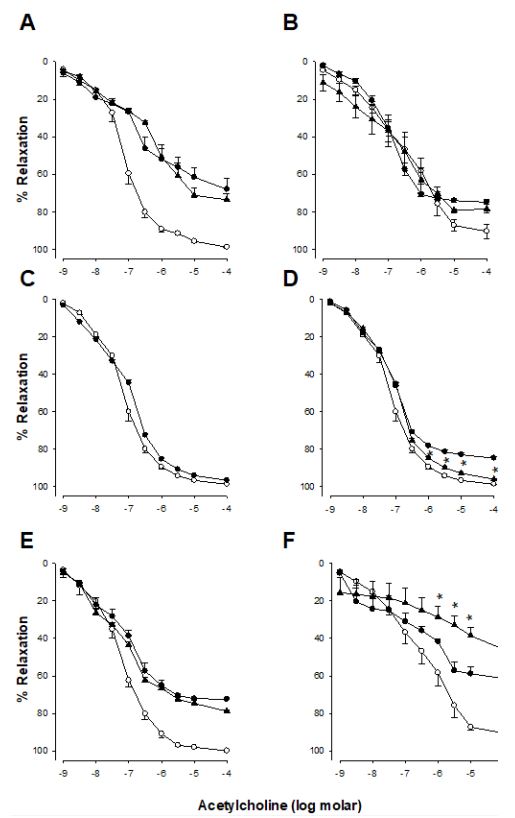
L-NAME (a nitric oxide synthase inhibitor, 10-6 M) (Figure 3A and B), losartan (an inhibitor AT1 receptor, 10-6 M) (Figure 3C and D) or indomethacin (inhibitor of the COX, 10-5M) (Figure 3E and F), did not modify the action of metformin on relaxation by ACh with high glucose (30 mM). On normal glucose conditions (5.8 mM). We are determinate that losartan did not involve in the mechanisms of the action of metformin. L-NAME inhibited the metformin action in high glucose, it indicates that L-NAME has an interaction with NOS, that low the bioavailability of NO, producing the decrease of relaxation to acetylcholine.
Effect of tetraethylammonium and clotrimazole
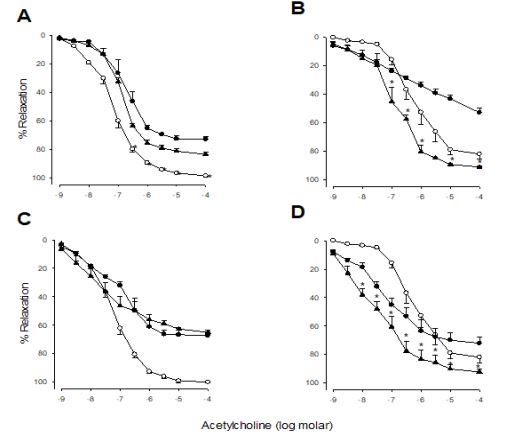
The Figure 4A y C show the effect of tetraethyl Ammonium (potassium channel inhibitor, 10-6 M) and Clotrimazole (cytochrome P450 inhibitor, 10-6 M) in glucose 5.8 M, produced decrease of relaxation to Ach (10-9 to 10-4 M) in approximately 20% with respect to control group (glucose 5.8 mM) respectively. High glucose (30 mM) group presented similar effects with respect to normal glucose group (5.8 mM), (Figure 4B and D). In contrast, in the high glucose (30 mM) and metformin (10-6 M) incubation, produced an inhibitory effect and reverted to normal glucose levels, This results indicates that metformin action is due to the CYP450, increasing the production of the hyperpolarizing factor, recovering the relaxation to acetylcholine and inhibiting the effects of high glucose.
Discussion
The results taken together, demonstrate that metformin leads to protective effect on the vasodilatation endothelium dependent of the rats normal mesenteric arteries, observed after acute exposure to high glucose concentrations corresponding to postprandial levels in patients with type 2 diabetes. We used the in vitro experimental model of isolated mesenteric arteries, which represents the major functionality of the circulatory system, and is a useful tool to evaluate a disease, as diabetes, that produces important alterations on the arterial pressure. The used of these preparations it has been demonstrated by Mulvany et al. [18,33,34], on various studies on the function of the micro vessel in different physiological and biochemicals aspects of the cardiovascular function.
Studies in vitro of high glucose effects on endothelium dependents responses and the productions of vasoactive prostanoids realized on aortas of normal rabbits (25 and 44 mM for 6 and 12 hrs), with control group (glucose 25 mM or 11 mM), indicated that glucose modified endothelium dependent relaxation where muscarinic receptors are involved, via the increase in prostanoids vasoconstrictors by activations of the PKC. Mannitol produced a relaxation similar in arteries relaxed with acetylcholine with a normal concentration of glucose [36,39].
This model can demonstrate the control of the arterial pressure in a pathological condition as diabetes, without interactions of the influence neuro-humoral and the blood cell. Gomes [25] demonstrated that metformin produced protection of high glucose effect on rabbit isolate perfused kidneys, restore the vasorelaxation by Acetylcholine. Gomes demonstrated that high glucose modified the nitric oxide effect, producing a relaxation decreased. Ozyazgan in 2001 [35] demonstrated that metformin produced protective effect on endothelial dysfunction in the rat thoracic aorta. The directly vascular effect of metformin was due to the action of both endothelium and vascular smooth muscle [27]. Several studies proposed the cellular mechanisms that involved the action of the metformin, such as a diminution of calcium in the vascular smooth muscle and a decreased of reactive oxygen species and vasodilation of NO-dependent, which results in increased of NO bioavailability [20,22,27,32,40]. We realized experiments with mesenteric arteries of male rats, in order to avoid hormonal effects, that existing between male and female, which are in relationship with the vascular activity.
Metformin has been shown to induced directly effect on the blood vessel wall, increasing the vasodilatation and diminution of the hypertensive activity in animal with high blood pressure [19,43], and patients [29]. The result of the present study indicated that the high concentration of glucose (30 mM), is on the range of patients and animal model after the oral administration of glucose (postprandial hyper-glycemic), that produced alterations in the vascular relaxations, therefore as the time of exposition to high glucose (30 minutes), where there are not differences in the vascular relaxation. For this, we realize experiments with high glucose 30 mM and 30 minutes of incubation. On the other hand, the effects of metformin (10-6M) on high glucose (30 mM), produced inhibitions on vascular reactivity by high glucose, responding to normal values. We determined if the glucose effect was not for changes in the osmolarity, through the use of sucrose (30 mM), where we determinate that relaxation was directly effect by glucose. Metformin did not produced changes in relaxation to acetylcholine in normal conditions (5.8 mM). Metformin induces a direct effect on the vascular endothelium, in view that in presence of endothelium the high glucose effect is reverted.
Metformin inhibited the action of high glucose, producing the recovering of the nitric oxide effect, when we utilized LNAME it produced an inhibition of metformin effect, but the action of indomethacin produced interaction with metformin, already metformin did not revert the effect of high glucose. Bhalla in 1996 [19] reported that metformin can also increases the NO production in the absence of NOS activity via alternative metabolic pathway in the vascular smooth muscle.
In endothelial cells of human and animals, the hyperglycemic produced an increased in the expression of the nitric oxide synthase but decreased nitric oxide [26,38]. Endothelial coronary cells of human, in exposition for 7 days in high glucose (25 mM), produced diminutions of production of the nitric oxide. In aorta rings of normal rats with high glucose (30 mM) for 1 hour, diminutions of the production of nitric oxide alternated the activity of the GMPc, inducing relaxation [38]. High glucose on arterioles of normal rats (30 and 50 mM for 1 hours), produced decrease of relaxation to acetylcholine, but indomethacin restored the relaxation to acetylcholine [31].
The infusion of 300 mg/dL i.v. of glucose for 6 hours in health human produced a decrease of relaxation to methacholine in the period of hyperglycemic. The acute hyperglycemic alternated the relaxation endothelium depend in health humans in vivo. The high glucose produced endothelial dysfunction in patients with diabetes mellitus [28].
Feletou 2004 [23], indicated that prostanois and EDHF (endothelium derived hyperpolarizing factor) could be implicated in the vascular relaxation. In this context, the result of the present study, demonstrated that high glucose (30 mM) interaction with CYTP450, produced decrease of acetylcholine relaxation, were metformin reverted the effect. On the other hand, metformin on the TEA (a nonspecific K+ channel inhibitor) effect, activated K+ -channels, inhibiting TEA effect on glucose 5.8 mM. However, this effect is not related to the action of metformin. This effect is relevant because K+ -channels play an important role on the vascular relaxation. On the vascular endothelium are three mechanisms that are involve on the ON relaxation, prostacyclin and hyperpolarizing factor endothelium derived, that produced most of 90% of relaxation to acetylcholine (dates not show). These mechanisms are alternated with high glucose but is most important the effect that produces on the NOS and cytochrome P450, producing decreases of the relaxation by vascular endothelium.
Conclusion
Metformin restored normal activity of vascular endothelium of mesenteric arteries in high glucose (30 mM), we were determinate that glucose interacted with NOS; this interaction produced a decrease o-f NO bioavailability, and with cytochrome P450, produced decrease vasorelaxation to acetylcholine. The effect of metformin is on the vascular endothelium and only in conditions of high glucose, already that in normal condition (glucose 5.8 mM), the metformin did not produce changes at acetylcholine vasorelaxation. Also, metformin presented minimum effect on K+ channel when were inhibited to TEA in normal condition and high glucose. These mechanisms are important, already that metformin had a protective action of high glucose in patients with diabetes mellitus type 2, these patients could have hypertensive events, with high frequency of death. These effects can be caused by the uncontrolled use of analgesics such as indomethacin, generating dysfunction of the vascular endothelium, increasing hypertensive events that affect health when glucose increases occur. The use of analgesics can cause the vascular endothelium to present a long-term dysfunction, affecting the health of the subjects.
Conflict of interest: The authors declare that they have no conflict of interest.
References
- Alvarez-Guisola F, Orozco-Beltran D, Cebrian-Cuenca AM, Ruiz Quintero MA, Angullo Martinez E, et al. Manejo de la hiperglucemia con fármacos no insulínicos en pacientes adultos con diabetes tipo 2. Atención Primaria. 2019; 51: 442-451.
- Edelmiro Menendez Torre E, Lafta Tejedor FJ, Artola Menendez S, Nuñez-Cortes JM, Alonso Garcia A, et al. Recomendaciones para el tratamiento farmacológico de la hiperglicemia en la diabetes tipo 2., Atención Primaria. 2011; 43: 202.e1-202.e9.
- Orozco-Beltran D, Brotons Cuixart C, Banegas Banegas JR, Gil Guillen VF, Cebrian Cuenca AM, et al. Recomendaciones preventivas cardiovasculares. Actualizacion PAPPS 2022, Atención Primaria. 2022; 54: 102444.
- Lv Z, Guo Y. Metformin and its benefits for various diseases, Frontiers in endocrinology. 2020; 11: 191.
- Goldberg RB, Orchard TJ, Crandall JP, Boyko EJ, Budoff M, et al. Diabetes Prevention Program Research Group. Effects of longterm metformin and lifestyle interventions on cardiovascular events in the diabetes prevention program and its outcome study, Circulation. 2022; 145(22): 1632-1641.
- Chen S, Gan D, Lin S, Zhong Y, Chen M, et al. Metformin in aging and aging-related diseases: clinical applications and relevant mechanisms. Theranostics. 2022; 12(6): 2722-2740.
- Foretz M, Guigas B, Viollet B. Metformin: Update on mechanisms of action and repurposing potential, Nature reviews endocrinology. 2023; s41574-023-00833-4.
- He M, Lu B, Opoku M, Zhang L, Xie W, et al. Metformin prevents or delays the developmen and progression of osteoarthritis: New insight and mechanism of action, Cells. 2022; 11: 3012.
- Cwynar, Zajac L. Metformin. A new approach, Pediatric endocrinology Diabetes and Metabolism. 2021; 27(2): 134-140.
- Flory J, Lipska K. Metformin in 2019, JAMA. 2019; 321(19): 1926-1927.
- Pierog M, Socala K, Nieozym D, Wyska E, Samorek-Pierog M, et al. Anticonvulsant profile of selected medium-chain fatty acids (MCFAs) co-administered with metformin in mice in acute and chronic treatment, Molecules. 2023; 28: 3810.
- Mohammed I, Hollenberg MD, Ding H, Triggle CR. A critical review of the evidence that metformin is a putative anti-aging drug that enhances healthspan and extends lifespan, Frontiers in endocrinology. 2021; 12-718942. doi: 10.3389/fendo.2021.718942
- Cejuela M, Martin-Castillo B, Menendez JA, Pernas S. Metformin and breast cancer: Where are we now?, Inrternational journal of Molecular Sciences. 2022; 23: 2705.
- Nojima I, Wada J. Metformin and its immune-mediated effects in various diseases. International Journal of Molecular Sciences. 2023; 24: 755.
- Alshahrani MY, Ebrahim HA, Alqahtani SM, Bayoumy NM, Kamar SS, et al. Metformin suppresses thioacetamide-induced chronic kidney disease in association with the upregulation of AMPK and downregulation of oxidative stress and inflammation as well as dyslipidemia and hypertension. Molecules. 2023; 28: 2756.
- Artasensi A, Mazzolari A, Pedretti A, Vistoli G, Fumagalli L. Obesity and type 2 diabetes: Adiposopathy as a triggering factor and therapeutic options. Molecules. 2023; 28: 3094.
- Li J, Zhang H, Ouyang H, Xu W, Sun Y, et al. Pueraria thomsonni Radix Wáter Extract Alleviate Type 2 Diabetes Mellitus in db/db Mice Through Comprehensive Regulation of Metabolism and Gut Microbiota. Molecules. 2023; 28: 7471.
- Aalkjaer CE, Mulvany MJ. Human and rat resistance vessels: A comparison of their morphological and pharmacological characteristics. Gen Pharmacol. 1993; 14: 85-87.
- Bhalla RC, Toth KF, Tan E, Batí RA, Mathias E, et al. Vascular effect of metformin. Possible mechanism for it’s antihypertensive action in the spontaneously hypertensive rat. Am J Hypertens. 1996; 9: 570-576.
- Dandona P, Aljada A, Chaudhuri A, Mohanty P. Endotelial dysfuntion, inflammation and diabetes. Rev Endocr Metab Disord. 2004; 5: 189-197.
- Ding Y, Vaziri ND, Coulson R, Kamanna VS, Roh DD. Effects of simulated hyperglycemia, insulin and glucagon on endothelial nitric oxide synthase expression. Am. J. Pysiol. Endocrinol. Metab. 2000; 279: E11-E17.
- Dominguez LJ, Davidoff AJ, Srinivas PR, Standley PR, Walsh MF, et al. Effect of metformin on tyrosine kinase activity, glucose transport and intracellular calcium in rat vascular smooth muscle. Endocrinology. 1996; 137: 113-121.
- Feletou M, Vanhouttle PM. EDHF: New therapeutic targets? Pharmacol Res. 2004; 49: 565-580.
- Giugliano D., Marfella R., Coppola L. Vascular effects of acute hyperglycemia in humans are reverse by L-arginine. Circulation. 1997; 95: 1783-1790.
- Gomes MB, Cailleaux S, Tibaricá. Metformin prevents the impairment of endothelium-dependent vascular relaxation induced by high glucose challenge in rabbit isolated perfused kidneys, Naunyn-Schmiedeberg’s Arch Pharmacol. 2005; 372: 24-30.
- Hulthen UL, Endre T, Mattiasson I, Berglund G. Insulin and forearm vasodilation in hypertensive-prone men. Hypertension. 1995; 25: 214-218.
- Katakam PV, Ujhelyi MR, Hoenig M, Miller AW. Metformin improve vascular function in insulin-resistant rats. Hypertension. 2000; 35: 108-112.
- Laakso M, Edelman SV, Brechtel G, Baron A.D. Impaired insulinmediated skeletal muscle blood flow in patients with NIDDM. Diabetes. 1992; 41: 1076-1083.
- Landin-Wilhelmsen K. Metformin and blood pressure. J Clin Pharm Ther. 1992; 17: 75-79.
- Lash JM, Nase GP, Bohlen HG. Acute hyperglycemia depresses arteriolar NO formation in skeletal muscle. Am J Physiol. 1999, 227:H1513-H1520.
- Lembo G, Rendina V, Laccarino G, Lamenza F, Volpe M, et al. Insulin reduces reflex forearm sympathetic vasoconstriction in healthy humans. Hypertension. 1993; 21: 1015-1019.
- Marfella R, Acampora R, Verrazzo G, Ziccardi P, De Rosa N, et al. Metformin improves hemodynamic and rheological responses to L-Arginine in NIDDM patients. Diabetes Care. 1996; 19: 934-939.
- Mulvany MJ, Halpern W. Contractile properties of small arterial resistance vessel in spontaneously hypertensive and normotensive rats. Circ Res. 1977; 41: 19-26.
- Mulvany MJ, Aalkjaer C. Structure and function of small arteries. Physiol. Rev. 1990; 70: 941-961.
- Ozyazgan S, Ince E, Senses V, Sultuybek G, Akkan AG. Effect of hyperoxia and metformin on vascular responses to vasoactive compounds in rats. J. Basis Clin Physiol Pharmacol. 2001; 12: 249-261.
- Page MM, Watkins PJ. Provocation of postural hypotension by insulin in diabetic autonomic neuropathy. Diabetes. 1976; 25:90-95.
- Pieper G.M., Meier D.A. and Hager S.R.: Endothelial dysfunction in a model of hyperglycemia and hyperinsulinemia. Am. J. Physiol. 1995; 269: H845-H850.
- Saki K., Imaizumi T., Masaki H., Takeshita A.: Intra-arterial infusion of insulin attenuates vasoreactivity in human forearm. Hypertension. 1993; 22: 67-73.
- Scott AR, Bennett T, Wallace P, Brechtel G, Olefsky JM, et al. Effects of hyperinsulinaemia on the cardiovascular responses to graded hypovolaemia in normal and diabetic patients. Clin Sci. 1988; 75: 85-92.
- Sharma RV, Bhalla RC. Metformin attenuate agonist-stimulated calcium transients in vascular smooth muscle cells. Clin Exp Hypertens. 1995; 17: 913-929.
- Taylor PD, Poston L. The effect of hyperglycaemia on function of rat isolated mesenteric resistance artery. Br. J. Pharmacol. 1994; 113: 801-808.
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. New England J Medicine. 1993; 329: 977-986.
- Verma S, Bhanot S, McNeill JH. Metformin decrease plasma insulin levels and systolic blood pressure in spontaneously hypertensive rats. Am J Physiol. 1994; 267: H1250-H1253.