
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Influence of protein intake on clinical and nutritional parameters in pancreatic cancer
Aline Emanuel1; Friederike Rosenberger2; Julia Krampitz3; Christiane Decker-Baumann4; Angela Märten5 ; Dirk Jäger4; Ingeborg Rötzer4,6*
1Division of Nutrition Sciences, German University of Applied Sciences for Prevention and Health Management (DHfPG), 66123 Saarbruecken, Germany.
2Division of Health Sciences, German University of Applied Sciences for Prevention and Health Management (DHfPG), 66123 Saarbruecken, Germany.
3Division of Psychology and Pedagogy, German University of Applied Sciences for Prevention and Health Management (DHfPG), 66123 Saarbruecken, Germany.
4Department of Medical Oncology, National Center for Tumor Diseases (NCT), Heidelberg University Hospital, 69120 Heidelberg, Germany.
5Boehringer Ingelheim International GmbH, Ingelheim am Rhein, Germany.
6Clinic for Oncology and Haemotology, Northwest Hospital, UCT-Cancer University Center, 60488 Frankfurt am Main, Germany.
*Corresponding Author : Ingeborg Rötzer
Department of Medical Oncology, National Center for
Tumor Diseases (NCT), Heidelberg University Hospital,
69120 Heidelberg, Germany.
Tel: +49-6221-5638233;
Email: ingeborg.roetzer@med.uni-heidelberg.de
Received : Jan 09, 2024
Accepted : Feb 06, 2024
Published : Feb 13, 2024
Archived : www.jjgastro.com
Copyright : © Rötzer I (2024).
Abstract
Introduction: Nutritional status is an important determinant of survival in patients with advanced pancreatic cancer. However, the effects of protein intake on nutritional status are largely unknown. This analysis examined the influence of guidelineconsistent protein intake over 13 weeks on clinical outcomes (survival, adverse events, modification of chemotherapy regimes) and nutritional status (body weight, phase angle, handgrip strength, prealbumin, albumin, and C-reactive protein) in patients with advanced pancreatic cancer.
Methods: 15 patients in the PANUSCO study received nutritional counselling and some received additional parenteral nutrition. Patients were retrospectively divided into two groups: high protein (n=7) (≥1.5 g/kg body weight (including parenteral nutrition)) and normal protein (n=8) (<1.5 g/kg body weight (including parenteral nutrition)) over time.
Result: There were no differences in clinical outcomes and no differences or changes in nutritional status between groups. Only C-reactive protein showed a decrease in normal protein group (p=0.031) and mGPS an improvement in high protein group (p=0.048) over time. There was a correlation between a lower mean protein intake and an increase in the modification of chemotherapy regimes (p=0.002).
Conclusion: Although, protein intake above the guideline recommendations may not have further beneficial effects on clinical outcomes and nutritional status, we could stabilize nutritional outcome parameters in both groups.
Keywords: Nutritional status; Protein intake; Pancreatic cancer; Malnutrition; Cachexia; Survival.
Abbrevations: AE: Adverse Events; BCM: Body Cell Mass; BIA: Bio Impedance Analysis; BMI: Body-Mass-Index; BSNC: Best Supportive Nutritional Care; BW: Body Weight; CRP: C-Reactive Protein; Ctx: Chemotherapy; ECM: Extracellular Mass; FA: Folinic Acid; HEN: Home Enteral Nutrition; HP: High Protein; mGPS: Modified Glasgow-Prognostic-Score; NP: Normal Protein; ONS: Oral Nutritional Supplement; PAL: Physical Activity Level; PN: Parenteral Nutrition; SAE: Serious Adverse Event; 5-FU: 5-Fluorouracil.
Citation: Emanuel A, Rosenberger F, Krampitz J, Baumann DC, Rötzer I, et al. Influence of protein intake on clinical and nutritional parameters in pancreatic cancer. J Gastroenterol Res Pract. 2024; 4(1): 1181.
Introduction
Patients with advanced pancreatic cancer are often characterized by weight loss [1,2] tumor cachexia [3] malnutrition [4-7] and systemic inflammation [8]. This weight loss is associated with poor treatment outcome and survival time [9-14]. In addition, weight loss and malnutrition lead to reduced quality of life [13].
Common symptoms associated with weight loss in patients with advanced cancer are decreased body fat and lean body mass, decreased protein levels (especially albumin and prealbumin), decreased caloric and protein intake, decreased total caloric expenditure with increased resting caloric expenditure, increased inflammatory markers and other non-specific findings such as pain, fatigue or edemas [15]. Furthermore, patients often experience loss of appetite [16].
The European Palliative Care Research Collaborative confirms that there is sufficient evidence to support the relationship between nutritional interventions, nutritional status, and quality of life in people with cancer [17]. Adequate protein intake is considered particularly important in the prevention and treatment of malnutrition. Insufficient protein intake has been identified as an independent poor prognostic factor in patients with unresectable pancreatic cancer receiving chemotherapy (CTx) [18]. A daily protein-/amino acid intake of 1.2-1.5 g/kg of Body Weight (BW) is recommended for cancer patients, with up to 2 g/kg of BW in cases of severe inflammation [13].
In contrast, a recent RCT in mechanically ventilated nutritionally high-risk patients (not exclusively cancer patients in intensive care unit) raised doubt in the benefits of very highdose protein intake. High-dose protein intake (parenteral & enteral) (≥2.2 g/kg/day) compared with usual-dose protein intake (parenteral & enteral) (≤1.2 g/kg/day) did not improve time to hospital discharge and no difference in 60-day mortality rate. A subgroup analysis showed even worse outcomes in patients with acute renal failure and high organ failure scores [19].
Several studies have analyzed the effect of protein intake on various parameters of survival and nutritional status in pancreatic cancer patients. A previously published observational study of patients with unresectable pancreatic cancer receiving CTx showed that daily protein intake was significantly higher in the surviving group (survival >12 months) than in the deceased group one month after the start of CTx, while baseline dietary intake was similar in both groups [18]. However, no parameters of nutritional status were obtained in addition to survival. Another study showed a significant increase in BW when patients with unresectable pancreatic cancer had a high compliance with a protein- and energy- dense oral nutritional supplement enriched with or without n-3 fatty acids [20]. Another trial of a protein and energy dense supplement enriched with n-3 fatty acids and antioxidants versus an isocaloric and isonitrogenous control supplement showed significant correlations in a posthoc-dose-response analysis between supplement intake and weight gain and an increase in lean body mass in the n-3 fatty acid enriched supplement group [21]. However, a recent review shows that previous studies tend to focus on a very short intervention period of a few days before (two days) and after (five days) surgery [22].
Therefore, we aimed at investigating whether protein intake above the guideline recommendations over a longer period of 13 weeks affects clinical outcomes (survival, Adverse Events (AE), modification of CTx regimes) and nutritional status (BW, phase angle, handgrip strength, prealbumin, albumin, C-Reactive Protein (CRP)) in patients with advanced pancreatic cancer undergoing CTx. To do so, we retrospectively divided subgroups of an RCT according to the actual protein intake irrespective of how these proteins were supplied (oral, -supplements (ONS) or parenteral).
Materials & methods
Design and patient population
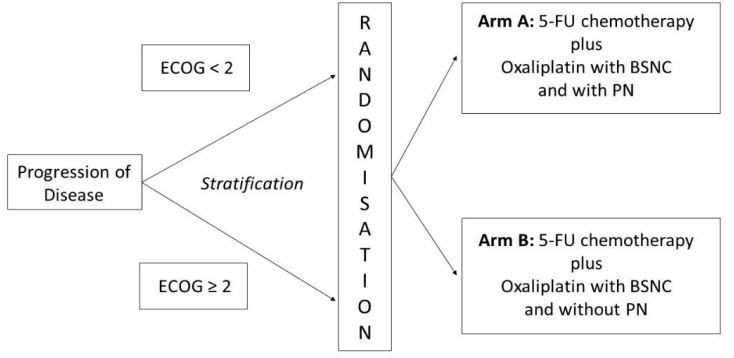
The data for this analysis are from the PANUSCO trial (NCT01362582). PANUSCO was a controlled, open-label, prospective, randomized, phase IIIb, multicenter trial with two parallel arms to investigate the effects of Parenteral Nutrition (PN) versus best supportive nutritional care (BSNC) on event-free survival in patients with advanced pancreatic cancer (Supplementary Figure S1) [23].
The study was terminated prematurely because the calculated sample size of 120 patients could not be achieved. In this secondary analysis, the available datasets from our center were evaluated in an exploratory way. Data sets from weekly visits from baseline (t1) to week 13 (t13) were analyzed.
Patients over 18 years of age with histologically confirmed advanced pancreatic adenocarcinoma who had received at least one prior CTx (gemcitabine-based) and experienced disease progression on this prior CTx were screened for participation. At enrolment, all patients received 5-fluorouracil (5-FU), folinic acid (FA) and oxaliplatin as second or higher line CTx [23].
Detailed inclusion and exclusion criteria are given in Table 1.
Endpoints
Primary endpoints of this exploratory analysis were clinical outcomes and the nutritional status. Clinical outcomes were defined as survival, AE and modification of CTx regimes. Nutritional status was defined as BW, phase angle, handgrip strength, prealbumin, albumin and CRP. Secondary outcomes were bodymass-index (BMI), body composition as the ratio of extracellular mass to body cell mass (ECM/BCM ratio), biceps size, modified Glasgow-Prognostic-Score (mGPS) and prognostic inflammatory and nutritional index (PINI). All values were assessed at week 1, 4, 7, 10 and 13.
All patients received BSNC, defined as weekly nutritional consultation (face-to-face or by phone) and recommendation by experienced nutritionists (PANUSCO intervention and control group). All types of ONS were allowed. Some patients (PANUSCO intervention group) received an additional PN (SMOFKabiven®, Omegaven®, Frekavit fat soluble®, Frekavit water soluble novum® and Tracitrans plus®). The infusions contained 1150 kcal, 50 g amino acids, 125 g glucose and 43 g fat with fish oil, soybean oil, medium chain triglycerides and olive oil. The detailed compositions are given in Supplementary Table S1.
The actual administration of PN was recorded. All patients received the same composition of PN, it was considered supplemental. The infusion frequency per protocol was six times per week. PN was discontinued on the day of CTx.
The nutritional intervention as well as the CTx was administered until individual discontinuation criteria were met. For both arms, individual stopping criteria for the nutritional intervention were met if two of the following three criteria were present:
(1) Weight loss >2% within the last seven days or caloric intake ≤500 kcal expected within the next five days,
(2) Bio impedance analysis (BIA) phase angle and BCM with a deterioration >10% (in both parameters) compared to baseline assessment,
(3) PINI-index >10 (only in patients with no sign of acute inflammation) [23].
Anthropometric data
The BW was recorded independently by the patients at home and asked at weekly visits. BMI was calculated from weight and height (weight [kg] / (height [m]²)). Handgrip strength was measured using a Jamar Hand Dynamometer (Sammons Preston, Bolingbrook, IL). Subjects performed three maximum force trials with the non-dominant hand. The maximum value of the non-dominant hand (in kg) was used for documentation. The biceps size was measured with a standard tape measure on the relaxed non-dominant arm at the midpoint of the upper arm between the acromion and olecranon. BIA was performed using a bioelectrical impedance analyzer (Data Input GmbH, Darmstadt) and conducted while patients were lying supine on a bed or examination table, with legs apart and arms not touching the torso. Electrodes were placed on the dorsum of the right foot and hand; the current-introducing electrodes were placed beyond the detector electrodes on the right hand. Resistance (R) and capacitance (Xc) was directly measured in ohms (0-1300) at 50.000 kHz, 0.8 mA for the estimation of phase angle and ECM/ BCM ratio. The phase angle was calculated using the following equation: Phase angle = (R/Xc) x (180/Π).
Blood markers
Venous blood samples of 7.5 mls were analyzed for prealbumin, albumin and CRP.
PINI is a scoring system that has been used to evaluate the nutritional status in critically ill subjects (24). PINI was calculated with alpha 1-acid glycoprotein (AAGP (mg/l) x (CRP (mg/l)) / (albumin (g/l) x prealbumin (mg/l)). A score >30 indicates a lifethreatening risk. High risk is present at 21-30, medium risk at 11-20, low risk at 1-10 and a minimal risk at less than one [25].
The mGPS is a combination of CRP and albumin levels; it reflects systematic inflammation and nutritional status. It has also been shown to have prognostic value in several tumours. A scoring system is used to define different score levels (26). Score zero is defined as CRP ≤10 mg/l, score one as CRP >10 mg/l and score two as CRP >10 mg/l and a albumin <35 g/L [27].
Dietary protocol
Protein and caloric intake were documented weekly by nutritionists with 24-hour recall. Analysis was performed using the nutrition software DGE professional. Basal metabolic rate was calculated using the Harris/Benedict equation [28]. The basal metabolic rate was multiplied by a Physical Activity Level (PAL) factor of 1.5 to determine the estimated total caloric requirement.
Adverse events
The documentation of National Cancer Institute “Common Terminology Criteria for Adverse Events version 4.0” (CTCAE v4.0) was used to monitor symptomatic AE. AE were classified into five grades. Grade one stands for a mild AE, grade two for a moderate AE, grade three for a severe AE, grade four stands for life-threatening or disabling AE and grade 5 stands for death related to an AE. Independent of this classification, a Serious Adverse Event (SAE) was defined as one that at any dose results in death, is life-threatening, requires subject hospitalization or prolongation of existing hospitalization, results in persistent or significant disability/incapacity or was a congenital anomaly/ birth defect.
Sample size
A total of 31 patients were enrolled in PANUSCO at our center, and data on protein intake were available for 27 patients. Data from patients who participated in the study for more than 12 weeks were analysed. Therefore, 15 patients were included in this secondary analysis.
Retrospective grouping
Two cluster sample groups were formed retrospectively to examine the effect of protein intake above the guideline recommendations on our defined outcomes. According to the ESPEN guideline [13], the first group (“High Protein” HP) was defined as ≥1.5 g protein/kg of BW on average over the 13 week analysis period and the second group (“normal protein” NP) as <1.5 g protein/kg of BW on average.
Of the 15 analysed patients, seven patients (47%) had an intake of ≥1.5 g protein/kg of BW and were assigned to the HP group. Of these, four patients were from the original PANUSCO intervention group (with PN). Eight patients (53%) had an intake of <1.5 g protein/kg of BW and were allocated to the NP group. All these patients were from the original PANUSCO control group (without additional PN).
Statistical analysis
Descriptive statistics (means and standard deviations) were performed for all outcome parameters. Missing data were imputed with the last available data. The data set did not meet the requirement for parametric statistical procedures. Wilcoxon tests were performed for all nutritional status outcomes and for each group to show the changes over the course of the 13- week intervention. Mann-Whitney U-Tests were performed for all nutritional status outcomes to show differences between the groups at baseline (t1), at the end of the analysis period (t13) and for change from t1 to t13 (delta). Mann-Whitney UTests were also performed for differences between the groups in number of AE and SAE. Survival was estimated using a Kaplan Meier curve and the log rank test. Fisher’s exact tests were used for comparison of some patients’ characteristics and for comparison of the frequency distribution of the present mGPS, AE, SAE and modification of CTx regimes. Spearman’s rank correlation test was performed to test the correlation between mean protein intake over time with a) the changes in all outcome variables of nutritional status, b) AE and c) modification of CTx regimes. All tests were performed with exact significance and were two-tailed. P<0.05 indicates statistical significance. TheIBM SPSS version 28.0 software, Chicago, IL, USA, was used.
Results
Patients’ characteristics
The clinical characteristics of the patients at t1 are shown in Table 2. There were no significant baseline differences between the groups in terms of gender, age, body weight, BMI and surgery.
Outcomes
Clinical outcomes
Survival: A 13-week protein supplementation above guideline recommendations did not result in a survival benefit (p=0.502, Figure 1).
Adverse events: There were various AE in both groups, including diarrhea, fatigue, nausea, anemia or vomiting. Only two patients (both HP) showed no AE over 13 weeks. The mean number of AE per person was 6.86±9.512 in HP and 8.00±4.840 in NP. There were no significant differences between groups in presence of SAE (p=0.467) and AE (p=0.200). In addition, there were no significant correlations between the number of SAE or AE (grade 1-5) and the mean protein intake over time. The number of AE and SAE is shown in Table 3.
Modification of chemotherapy regimes: There was a significant correlation between more modification of CTx with lower mean protein intake over time in g (p=0.031) and g/kg BW (p=0.002). There was a trend towards more modification of CTx in NP (p=0.077). There was no modification of CTx in HP. In NP, four patients experienced interruptions (two times) and reductions (five times) (reasons: low platelet count, toxicity, diarrhea, tooth extraction).
Nutritional status: The primary outcome measures of nutritional status are shown in Table 4.
Body weight: BW did not change in either group, and the development over time was not significantly different between groups (p=0.121).
Phase angle: Phase angle did not change in either group, and the development over time was not significantly different between groups (p=0.889).
Handgrip strength: Handgrip strength did not change in either group, and the development over time was not significantly different between groups (p=0.888).
Prealbumin: Prealbumin did not change in either group, and the development over time was not significantly different between groups (p=0.757).
Albumin: Albumin did not change in either group, and the development over time was not significantly different between groups (p=0.979).
CRP: CRP did not change in HP. In NP there was a significant decrease from t1 to t13 (p=0.031). The development over time was significantly different between groups (p=0.039). There was a significant correlation between a higher mean protein intake (g/kg BW) during t1 to t13 and an increase in CRP during t1 to t13 (p=0.016) (Figure 3).
All other correlations were not significant.
Secondary outcomes
In HP and NP, mean BMI showed no significant change between t1 and t13. There were no significant differences between the groups at t1 and t13 and no significant difference in the change of BMI (p=0.128). In HP and NP, mean ECM/BCM showed no significant change between t1 and t13. There were no significant differences between the groups at t1 and t13 and no significant difference in change of ECM/BCM ratio (p=0.444). In HP and NP, mean biceps size showed no significant change between t1 and t13. There were no significant differences between the groups at t1 and t13, but a trend towards a smaller biceps size in HP at t1 (p=0.064) and there was no significant difference in change in biceps (p=0.128). In HP there was a significant worsening in mGPS from t1 to 13 (p=0.048). In NP there was no significant change from t1 to t13. Furthermore, there were no significant differences in mGPS in HP versus NP at t1 and t13 and there was no significant difference in change in mGPS (p=0.221). In HP, mean PINI showed no significant change between t1 and t13. In NP, mean PINI showed a trend towards a decrease (p=0.063). There were no significant differences between the groups at t1 and t13 and no significant difference in the change of PINI (p=0.157).
Caloric intake from all sources
In HP, mean caloric intake was 2601±748 kcal at t1 and 2815±663 kcal at t13. The mean change in caloric intake from t1 to t13 was 214±540 kcal/day. Mean difference from calculated energy requirement was 621±639 kcal at t1 and 796±662 kcal at t13. Mean change in difference to calculated energy requirement from t1 to t13 was 174±520 kcal/day.
In NP, mean caloric intake was 2083±725 kcal at t1 and 2213±719 kcal at t13. The mean change in caloric intake from t1 to t13 was 130±838 kcal/day. Mean difference from calculated energy requirement was 28±491 kcal at t1 and 171±736 kcal at t13. The mean change in difference to calculated energy requirement from t1 to t13 was 143±852 kcal/day.
Caloric intake was not significantly different between groups at t1 (p=0.232) and t13 (p=0.152). There were no significant changes in caloric intake from t1 to t13 within HP (p=0.453) and NP (p=0.547). The difference to calculated energy requirement was not significantly different, but there were trends between groups at t1 (p=0.094) and t13 (p=0.094). There were no significant changes in the difference to calculated energy requirement from t1 to t13 within HP (p=0.375) and NP (p=0.547).
Protein intake
In HP, mean protein intake was 115.0±34.5 g at t1 and 116.8±43.5 g at t13. The mean change in protein intake from t1 to t13 was 1.7±17.2 g. The mean protein intake in g/kg BW was 1.8±0.6 at t1 and 1.8±0.7 g at t13. The mean change in protein intake from t1 to t13 was 0.0±0.3 g/kg BW.
In NP, mean protein intake was 87.4±36.5 g at t1 and 79.1±26.2 g at t13. The mean change in protein intake from t1 to t13 was -8.3±39.3. The mean protein intake in g/kg BW was 1.3±0.4 at t1 and 1.2±0.3 g at t13. The mean change in protein intake from t1 to t13 was -0.1±0.6 g/kg BW.
Protein intake in gram was not significantly different between groups at t1 (p=0.189) and t13 (p=0.152). There were no significant changes in protein intake from t1 to t13 with-in HP (p=0.938) and NP (p=0.945). Protein intake in g/kg BW was significantly different between groups at t1 (p=0.040) and t13 (p=0.036). There were no significant changes in protein intake in g/kg BW from t1 to t13 within HP (p=0.563) and NP (p=0.781).
Figure 4 shows the individual protein intakes including PN. It is interesting to note that protein intakes varied widely over the 13 weeks.
The patients with PN(n=4) received this intervention 5.05±0.92 times per week over the complete intervention period. PN contributed to 37.3% (mean) (28.6-56.1 %) of the total protein intake. As PN was not taken regularly, mean values were calculated over the course of the 13 weeks. These values were added to the oral protein intake. With regard to the administration of PN, it was found that the dose described in the methods was not consistently given. The protocols showed deviations from the study protocol in the infusion frequency. This inconsistency is due to individual patient tolerances and adherence.
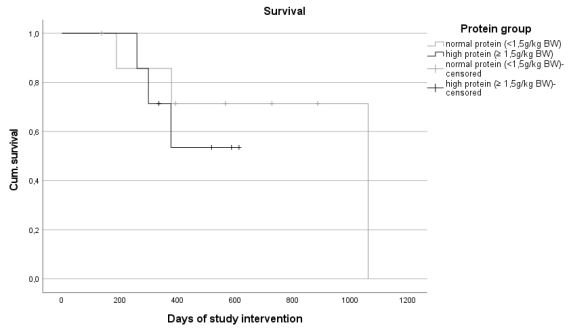
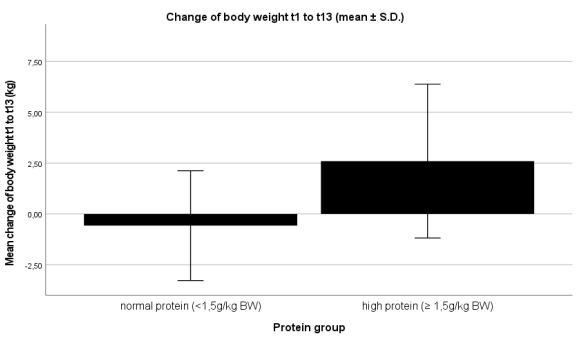
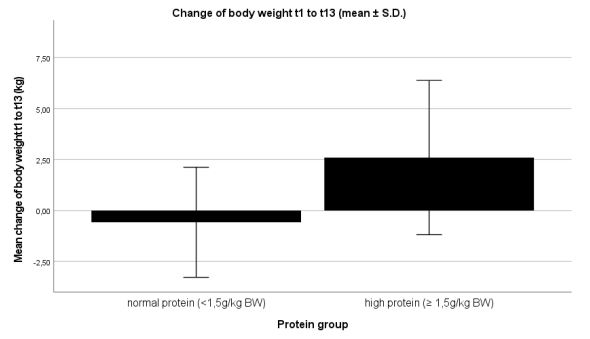
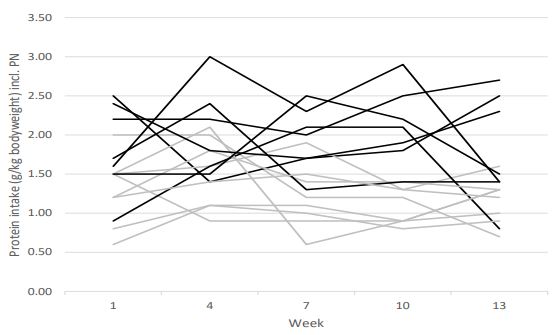
Table 1: Eligibility criteria [23].
| Inclusion criteria | Exclusion criteria |
|---|---|
| Written informed consent | Major surgery <4 weeks prior to enrolment |
|
Histological confirmed ad- vanced pancreatic adenocar- cinoma |
Weight loss >2% within the last seven days or caloric intake ≤500 kcal expected within the next five days |
|
At least one previous chemo- therapy (gemcitabine-based) |
PINI1 >10 |
| ≥18 years old | Pregnancy or breastfeeding |
| Body weight ≥50 and ≤95 kg |
>4 weeks of PN within the last 6 months PN <4 weeks prior to enrolment |
| Body-Mass-Index ≥19 kg/m² |
Vulnerable populations (e.g. subjects incapa- ble of giving consent personally) |
|
Willingness to perform double-barrier contraception during study |
Subject selection conflicts with warnings, pre- cautions and contraindications stated for any investigational product |
| Expected life expectancy >3 months | |
1PINI: Prognostic Inflammatory and Nutritional Index.
Table 2: Patient characteristics (t1).
| High protein n=7 |
Normal protein n=8 |
P Value | |
|---|---|---|---|
| Gender (M/F) | 5/2 | 4/4 | 0.6081 |
| Age (years) | 67±4.4 | 68±6.5 | 0.5922 |
| Body weight (kg) | 63.3±7.7 | 68.5±15.3 | 0.7792 |
| Body-Mass-Index (kg/m²) | 21.7±2.4 | 24.4±2.8 | 0.1612 |
| Surgery (yes/no) | 5/2 | 6/2 | 1.0001 |
| PANUSCO intervention/ control group (n) | 4/3 | 0/8 | 0.0261 |
| Ø Protein intake (g) t1-t13 | 125.1±20.7 | 84.3±22.2 | 0.0042 |
| Ø Protein intake (g/kg BW) t1-t13 | 1.9±0.3 | 1.2±0.2 | <0.0012 |
Values are given as mean ± S.D. except for gender (males (M) and fe- males (F)) and surgery. Values for protein intake included parenteral nutrition. 1Pearson-Chi-Square; 2Mann-Whitney U-Test.
Table 3: Number of adverse events.
| Grade | High protein (n) | Normal protein (n) | P Value |
|---|---|---|---|
| 1 | 21 | 33 | 0.290 |
| 2 | 16 | 22 | 0.604 |
| 3 | 10 | 9 | 0.600 |
| 4 | 1 | 0 | 0.467 |
| 5 | 0 | 0 | 1.000 |
| SAE | 0 | 6 | 0.467 |
Mann-Whitney U-Test.
Table 4: Nutritional outcome parameters.
| High protein | Normal protein | |||||||
|---|---|---|---|---|---|---|---|---|
| T1 | T13 | Sign.1 | T1 | T13 | Sign.1 | Sign.2 | Sign. | |
| Primary endpoints | ||||||||
| Body weight (kg) | 63.3±7.7 | 65.9±8.7 | 0.156 | 68.5±15.3 | 67.9±15.3 | 0.531 | 0.779 | 0.929 |
| Phase angle (°) | 4.6±0.6 | 4.8±0.5 | 0.344 | 4.6±0.9 | 5.0±0.6 | 0.453 | 0.956 | 0.761 |
| Handgrip strength (kg) | 30.9±6.6 | 30.1±10.1 | 0.563 | 24.9±9.2 | 24.8±9.7 | 0.938 | 0.161 | 0.447 |
| Prealbumin (mg/L) | 186±61 | 207±63 | 0.500 | 160±53 | 189±61 | 0.172 | 0.377 | 0.575 |
| Albumin (g/L) | 39.0±1.3 | 38.3±3.9 | 1.000 | 38.5±3.4 | 38.7±1.7 | 0.945 | 0.843 | 0.799 |
| CRP (mg/L) | 7.7±5.9 | 11.0±14.2 | 0.438 | 13.2±14.7 | 3.9±3.3 | 0.031 | 0.440 | 0.978 |
| Secondary endpoints | ||||||||
| BMI (kg/m²) | 21.7±2.4 | 22.6±2.6 | 0.156 | 24.4±2.8 | 24.2±3.1 | 0.578 | 0.161 | 0.268 |
| ECM/BCM ratio | 1.3±0.2 | 1.2±0.2 | 0.156 | 1.4±0.4 | 1.3±0.3 | 1.000 | 0.955 | 0.867 |
| Biceps size (cm) | 24.5±3.3 | 25.9±3.3 | 0.156 | 27.5±2.3 | 25.8±4.7 | 0.453 | 0.064 | 0.931 |
| mGPS 0 (n) | 5 | 5 | 0.0484 | 4 | 7 | 0.5005 | 0.6086 | 0.3237 |
| mGPS 1 (n) | 2 | 0 | 2 | 1 | ||||
| mGPS 2 (n) | 0 | 2 | 2 | 0 | ||||
| PINI | 1.2±1.2 | 2.4±4.2 | 0.813 | 4.4±8.9 | 0.5±0.7 | 0.063 | 0.405 | 0.915 |
Values, except mGPS, are given as mean ± S.D. 1Wilcoxon Test for changes from t1 to t13 within group; 2 Mann-Whitney U-Test for differences between the groups at t1; 3 Mann-Whitney U-Test for differences between the groups at t13; 4Fisher’s exact test t1 to t13 in HP; 5Fisher’s exact test t1 to t13 in NP; 6Fisher’s exact test t1 HP vs. NP; 7Fisher’s exact test t13 HP vs. NP.
Supplementary materials.
Supp Table 1: Nutritional composition.
| Nutrition | Dosing |
|---|---|
| SMOFKabiven® |
was administered overnight, containing 1100 kcal in 986 ml.
986 ml emulsion for infusion contained: Amino acids (50 g),
glucose (125 g) and fat (38 g) with 30% soybean oil, 30% medium chain triglycerides, 25% olive oil and 15% fish oil. The parentally prescribed calorie intake of 1100 kcal was the same for all subjects in original PANUSCO intervention group and did not depend on body weight or nutritional status. This was not a total PN. The recommended infusion rate was 0.25 g glucose/kg body weight/hour and should not exceed 0.15 g glucose/kg body weight/hour, which was equiva- lent to 0.75 ml SMOFKabiven® /kg body weight/hour. |
| Omegaven® |
50 ml (=5 g fish oil) containing 50 kcal was administered
together with SMOFKabiven® as an omega-three fatty acid
supplement. The compatibility of SMOFKabiven® and Omegaven® was guaranteed by the manufacturer Fresenius Kabi Deutschland GmbH. |
| Frekavit fat-soluble® |
was administered overnight together with SMOFKabiven®. For
adult patients, the recommended daily dose was 10 ml (one
ampoule). 10 ml emul- sion for infusion contained: Retinol palmitate (1.941 mg) corresponding to retinol (0, 99 mg), phyto-menadione (150 mg), ergocalciferol (5 mg) and all-rac-α-tocopherol (10 mg). The parenteral intake of Frekavit fat-soluble® was the same for all subjects in original PANUSCO intervention group and did not de-pend on body weight or nutritional status. The infusion should be completed within 24 hours of preparation to avoid microbiological contamination. The remaining contents of the ampoules were to be discarded and not stored for later use. |
| Frekavit water-soluble novum® |
was an infusion concentrate of water-soluble vitamins. It
was administered overnight together with SMOFKabiven®. The
recommended daily dose for adult patients was the content of one ampoule. One ampoule contained: Thiamine mononitrate (3.1 mg), riboflavin sodium phosphate (4.9 mg), nicotinamide (40 mg), pridoxine hydrochloride (4.9 mg), sodium pantothenate (16.5 mg), sodium ascorbate (113 mg), biotin (60 μg), folic acid (0.40 mg) and cyanocobalamin (5.0 μg). The parenteral intake of Frekavit fat-soluble® was the same for all subjects in original PANUSCO intervention group and did not depend on body weight or nutritional status. |
| Tracitrans plus® |
was a concentrate for the preparation of an infusion
solution to cover the basal to moderately increased a
requirement of trace elements. The rec- ommended daily dose of Tracitrans plus® in adult patients was 10 ml (one ampoule). 10 ml concentrate for the preparation of an infusion solution contained: Zn++ (100 μmol), Mn++ (5 μmol), Cu++ (20 μmol), Fe+++ (20 μmol), MoO4 - (-0.2 μmol), SeO3 - (-0.4 μmol), I- (1 μmol), F- (50 μmol), Cr+++ (0.2 μmol), Na+ (<65 μmol), K+ (<10 μmol) abd Cl- (351 μmol). |
Discussion
The aim of this secondary analysis was to analyze whether protein intake above the guideline recommendations affects clinical outcomes (survival, AE, modification of CTx regimes) and nutritional status (BW, phase angle, handgrip strength, prealbumin, albumin and CRP) in patients with advanced pancreatic cancer undergoing CTx who were followed up for 13 weeks. There were no differences in clinical outcome parameters and no differences or changes in nutritional status parameters between the groups. However, there was a significant correlation between an increasing number of modification of CTx regimes and a lower mean protein intake over time.
Protein intake was focused in this analysis, as this macronutrient is thought to contribute to improved clinical outcomes. As all patients received weekly nutritional consultations as BSNC and were allowed to supplement freely, no difference in protein and caloric intake could be guaranteed. Therefore, in this secondary analysis, new groups were created according to protein intake. So, two distinct groups could be compared.
The cut-off value of 1.5 g protein/kg BW was chosen because various guidelines recommend 1.2 to 1.5 g for cancer or other clinical conditions [13,29-31]. This is because of the increased whole-body protein turnover [32] and the net protein loss [33] (e.g. due to inactivity or inflammation) in cancer patients. However, other recommendations are even higher (1.2-2.0 g/kg BW) [34]. It has not yet been clarified what the actual protein and amino acid requirements are, or whether higher intakes are beneficial. In tumour patients, it is thought that the anabolic resistance that often occurs is due to a higher threshold for stimulation of the protein synthesis than in healthy individuals [35]. A protein intake of less than 1.2 g/kg BW is associated with muscle wasting during treatment [36]. Other studies using PN and high protein intakes (2 g/kg BW) in severely malnourished cancer patients also showed no negative effects on metabolism [37]. If renal function is normal, these high doses are considered safe [38]. An umbrella review also showed no risk to renal health with protein intakes above 0.8 g/kg BW (the official German recommendation) in healthy and sick people [39]. Studies in weight training suggest protein intake of 0.4-0.5 g/kg BW per meal to build muscle mass. With 3-6 meals per day, this results in recommendations of 1.2-3.0 g/kg BW [40,41]. Another study of resistance training shows no significant difference between very high protein intakes (4.4 g/kg BW) and high protein intakes (1.8 g/kg BW) and no significant change in BW, fat mass, fat-free mass and body fat over an 8-week intervention [42]. This suggests that pancreatic cancer patients need a high protein intake to stabilize muscle mass and minimize the effects of cachexia and weight loss.
One patient in our study had an exceptionally high protein intake of 3.0 g/kg BW at week four. He also showed a stable high protein intake at all other points of time. Beyond our analysis period, he showed a protein intake of 5.91 g/kg BW at week 34. As he was part of the original PANUSCO control group that did not receive PN, it must be concluded that he supplemented. Supplementation beyond the intervention was not recorded. There have been some studies with extremely high protein intakes (3.0-4.4 g/kg BW) in healthy, trained individuals showing no adverse effects [42-45], but no change in body composition with a mean protein intake of 2.9 g/kg BW over 16 weeks of intervention [44]. Therefore, it is important to record actual oral protein intake, rather than simply setting a protein intake target.
Clinical outcomes showed no differences. Our results are in line with a RCT (n=200) on this topic with a shorter intervention time of eight weeks [21]. The study investigated a high-protein and high-energy supplement enriched with omega-3 fatty acids and antioxidants versus an isocaloric and isonitrogenic supplement. In the intervention group, significantly higher protein intake was achieved through improvement in dietary intake. No differences in survival and occurrence of AE and SAE could be shown. Interestingly, we found a significant correlation between an increasing number of modification of CTx regimes and a lower mean protein intake over time. Therefore, it could be an indication that there is a higher treatment tolerance with higher mean protein intake. This is in line with two other trials showed that a nutritional intervention had a positive effect/ improvement on treatment-tolerance [46,47]. A further study showed a lower risk for CTx toxicity, which could be seen as an improvement in treatment tolerance when patients got a whey protein supplementation [48]. In the context of these studies, we can assume that our findings point in the right direction.
Outcome parameters of nutritional status also showed no differences between groups and did not change over time. BW, phase angle, handgrip strength, prealbumin and albumin remained stable. Our results are in line with another RCT which showed no association of higher energy- and protein intake and improvements in body weight and hand-grip strength [49]. In contrast, another RCT showed a positive correlation between protein intake and hand grip strength [50]. Looking at parenteral nutrition alone, a RCT showed no weight change when PN (energy, macro- and micronutrients) was compared with an isotonic electrolyte solution in patients with pancreatic cancer on fasting days (3 days) in hospital [51]. In contrast, a RCT showed a significant difference in BW between a Home Enteral Nutrition (HEN) versus nutritional counselling. While patients with HEN remained their BW stable after two months, patients with nutritional counselling lost BW [52]. Due to the different interventions, the results are difficult to compare. However, CRP showed a significant decrease from t1 to t13 in NP and a value below 10 mg/l at t13, which does not represent an acute inflammatory response [53]. Furthermore, we found a significant correlation of high protein intake and rising CRP. However, the observed effects might not be attributable to protein intake alone, but to the disease itself, acute infections, individual outliers or, therapy-related. The two extreme values in Figure 3 with a marked increase and a marked decrease in CRP showed no signs of infection on further study assessment. Therefore, the change in values could be attributed to the disease itself. In contrast to our findings, a RCT in non-cancer patients showed that a higher protein intake compared with a normal protein intake led to a significant reduction in CRP [54]. This confirms our suspicion that there is probably no real advantage of normal compared to high protein intake in terms of CRP. Therefore, this statistical result should not be considered as clinically relevant. Above all, it should not be used as a basis for protein intake recommendations.
Looking at the secondary outcome parameters, mGPS showed a significant decrease from t1 to t13 in HP. Two patients with mGPS1 changed to mGPS2, during the intervention, which is considered to be a sign of worsening inflammation and nutritional status. The deterioration of mGPS can be explained by the increase in CRP and the associated deterioration of albumin as a negative acute-phase protein. No changes in mGPS scores were observed in NP. As the mGPS score is a relevant predictor of desease progression and survival [55], this can be considered success. While this is unusual in our patient population without additional intervention, it might be attributable to the weekly BSNC.
Taken all clinical and nutritional outcomes together, our analysis showed that there were no significant differences and changes in both groups. However, we could show a stabilization in several parameters, which could be seen as a success in patients with pancreatic cancer. It was probably due to the good Nutritional Care (BSNC) of both groups that no differences could be observed. Therefore, BSNC might be recommended for this patient group. Whether a protein intake above the current guideline recommendations could be useful needs to be investigated in a study with a larger sample and a larger difference in protein intake. A protein intake of more than 2 g protein /kg/BW is recommended in inflammatory conditions [13]. We could not form our groups according to the 2 g recommendation because there were not enough people who reached this target. Furthermore, in future studies, protein quality could be assessed in addition to protein quantity to learn whether it is relevant in the nutritional therapy of these patients.
A weakness of our analysis was the small sample size. Due to this, a possible existing effect might not have been demonstrated. A further limitation was the recording of the BW. The latter was only asked at the time of measurement and was not measured with a defined scale. This may have led to variations between participants. However, this is not relevant for the longitudinal analysis, as each patient always used the same scale and longitudinal analysis is based on within-patient changes. The basal metabolic rate was multiplied by a PAL factor of 1.5 in this analysis. This may have been a high factor. For patients with advanced pancreatic cancer, a PAL factor of 1.24 is recommended [56]. A positive and unique characteristic of this analysis was the long observation and analysis period. While most studies only looked at a few days before and after surgery [22], this analysis looked at the long-term effects of 13 weeks.
Conclusion
In summary, our 13-week analysis of patients with advanced pancreatic cancer revealed no benefit of protein intake above guideline recommendations (>1.5 g/kg BW) on clinical outcomes and the development of nutritional status. Both groups stayed stable in all parameters of nutritional status, which can be considered as success in this patient group. Both groups received nutritional counselling, which might be the reason for this success. However, we investigated only small groups. Therefore, larger studies are needed to confirm our findings.
Declarations
Conflicts of interest: The authors declare no conflict of interest.
Acknowledgements: We thank all patients of PANUSCO. Furthermore, we thank Sabine Kind for her support with the methodological design and statistical analysis.
Funding: This study was supported by the foundation ‘Leben mit Krebs’.
References
- Davidson W, Ash S, Capra S, Bauer J. Weight stabilisation is associated with improved survival duration and quality of life in unresectable pancreatic cancer. Clin Nutr. 2004; 23(2): 239-47.
- Richter E, Denecke A, Klapdor S, Klapdor R. Parenteral Nutrition Support for Patients with Pancreatic Cancer - Improvement of the Nutritional Status and the Therapeutic Outcome. Anticancer Research. 2012; 32: 2111-8.
- Fearon KC, Baracos VE. Cachexia in pancreatic cancer: new treatment options and measures of success. HPB (Oxford). 2010; 12(5): 323-4.
- Bosaeus I, Daneryd P, Svanberg E, Lundholm K. Dietary intake and resting energy expenditure in relation to weight loss in unselected cancer patients. International Journal of Cancer. 2001; 93(3): 380-3.
- Fearon KC, Barber MD, Falconer JS, McMillan DC, Ross JA, et al. Pancreatic cancer as a model: Inflammatory mediators, acutephase response, and cancer cachexia. World J Surg. 1999; 23(6): 584-8.
- Tisdale MJ. Cachexia in Cancer Patients. Nature. 2002; 2: 862-71.
- Laviano A, Meguid MM, Inui A, Muscaritoli M, Rossi-Fanelli F. Therapy insight: Cancer anorexia-cachexia syndrome--when all you can eat is yourself. Nat Clin Pract Oncol. 2005; 2(3): 158-65.
- Prokopchuk O, Steinacker JM, Nitsche U, Otto S, Bachmann J, et al. IL-4 mRNA Is Downregulated in the Liver of Pancreatic Cancer Patients Suffering from Cachexia. Nutrition and Cancer. 2017; 69(1): 84-91.
- Valentini L, Volkert D, Schütz T, Ockenga J, Pirlich M, et al. Leitlinie der Deutschen Gesellschaft für Ernährungsmedizin (DGEM). Aktuel Ernahrungsmed. 2013; 38(2): 97-111.
- Rock CL, Doyle C, Demark-Wahnefried W, Meyerhardt J, Courneya KS, et al. Nutrition and physical activity guidelines for cancer survivors. CA Cancer J Clin. 2012; 62(4): 243-74.
- Fearon K, Strasser F, Anker SD, Bosaeus I, Bruera E, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011; 12(5): 489-95.
- Bozzetti F, Arends J, Lundholm K, Micklewright A, Zurcher G, et al. ESPEN Guidelines on Parenteral Nutrition: non-surgical oncology. Clin Nutr. 2009; 28(4): 445-54.
- Arends J, Bertz H, Bischoff S, Fietkau R, Herrmann H, et al. S3-Leitline der Deutschen Gesellschaft für Ernährungsmedizin e. V. (DGEM) in Kooperation mit der Deutschen Gesellschaft für Hämatologie und Onkologie e. V. (DGHO), der Arbeitsgemeinschaft Supportive Maßnahmen in der Onkologie, Rehabilitation und Sozialmedizin der Deutschen Krebsgesellschaft (ASORS) und der Österreichischen Arbeitsgemeinschaft für klinische Ernährung (AKE). Aktuel Ernahrungsmed. 2015; 40(05): e1-e74.
- Bozzetti F. Nutritional support in patients with oesophageal cancer. Supportive Care in Cancer. 2010; 18 Suppl 2: S41-50.
- Erickson N, Schaller N, Berling-Ernst A, Bertz H. Ernährungspraxis Onkologie: Behandlungsalgorithmen, Interventions-Checklisten, Beratungsempfehlungen. Stuttgart: Schattauer. 2017.
- Argilés JM, Meijsing SH, Pallarés-Trujillo J, Guirao X, López-Soriano FJ. Cancer cachexia: A therapeutic approach. Medicinal Research Reviews. 2001; 21(1): 83-101.
- Radbruch L, Elsner F, Trottenberg P, Strasser F, Fearon KC. Clinical practice guidelines on cancer cachexia in advanced cancer patients with a focus on refractory cachexia. Aachen: Department of Palliative Medicine/ European Palliative Care Research Collaborative. 2010.
- Hasegawa Y, Ijichi H, Saito K, Ishigaki K, Takami M, et al. Protein intake after the initiation of chemotherapy is an independent prognostic factor for overall survival in patients with unresectable pancreatic cancer: A prospective cohort study. Clin Nutr. 2021; 40(7): 4792-8.
- Heyland DK, Patel J, Compher C, Rice TW, Bear DE, et al. The effect of higher protein dosing in critically ill patients with high nutritional risk (EFFORT Protein): An international, multicentre, pragmatic, registry-based randomised trial. The Lancet. 2023; 401(10376): 568-76.
- Bauer J, Capra S, Battistutta D, Davidson W, Ash S. Compliance with nutrition prescription improves outcomes in patients with unresectable pancreatic cancer. Clinical Nutrition. 2005; 24(6): 998-1004.
- Fearon KCH, Meyenfeldt MFv, Moses AGW, van Geenen R, Roy A, et al. Effect of a protein and energy dense n-3 fatty acid enriched oral supplement on loss of weight and lean tissue in cancer cachexia: a randomised double blind trial. Gut. 2003; 52(10): 1479-86. Available from: URL: https: //gut.bmj.com/content/gutjnl/52/10/1479.full.pdf.
- Emanuel A, Krampitz J, Rosenberger F, Kind S, Rötzer I. Nutritional interventions in pancreatic cancer: A systematic review. Cancers 2022. Available from: URL: https://www.mdpi.com/2072-6694/14/9/2212.
- Märten A, Wente MN, Ose J, Büchler MW, Rötzer I, et al. An open label randomized multicentre phase IIIb trial comparing parenteral substitution versus best supportive nutritional care in subjects with pancreatic adenocarcinoma receiving 5-FU plus oxaliplatin as 2ndor higher line chemotherapy regarding clinical benefit - PANUSCO. BMC Cancer. 2009; 9(1): 225.
- Walsh D, Mahmoud F, Barna B. Assessment of nutritional status and prognosis in advanced cancer: interleukin-6, C-reactive protein, and the prognostic and inflammatory nutritional index. Support Care Cancer. 2003; 11(1): 60-2.
- Serón-Arbeloa C, Labarta-Monzón L, Puzo-Foncillas J, MallorBonet T, Lafita-López A, et al. Malnutrition Screening and Assessment. Nutrients. 2022; 14(12).
- McMillan DC. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc Nutr Soc. 2008; 67(3): 257-62.
- Zürcher G, Arends J, Pirlich M. Tumorkachexie und Ernährungstherapie bei Krebserkrankungen. In: Biesalski HK, Bischoff SC, Pirlich M, Weimann A, editors. ErnährungsmedizinNach dem Curriculum Ernährungsmedizin der Bundesärztekammer. 5., vollständig überarbeitete und erweiterte Auflage. Stuttgart: Georg Thieme Verlag KG. 2018; 757.
- Harris JA, Benedict FG. A Biometric Study of Human Basal Metabolism. Proc Natl Acad Sci U S A. 1918; 4(12): 370-3.
- Guadagni M, Biolo G. Effects of inflammation and/or inactivity on the need for dietary protein. Curr Opin Clin Nutr Metab Care. 2009; 12(6): 617-22.
- Deutz NEP, Bauer JM, Barazzoni R, Biolo G, Boirie Y, et al. Protein intake and exercise for optimal muscle function with aging: recommendations from the ESPEN Expert Group. Clin Nutr. 2014; 33(6): 929-36.
- Bauer J, Biolo G, Cederholm T, Cesari M, Cruz-Jentoft AJ, et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J Am Med Dir Assoc 2013; 14(8): 542-59.
- Heber D, Chlebowski RT, Ishibashi DE, Herrold JN, Block JB. Abnormalities in glucose and protein metabolism in noncachectic lung cancer patients. Cancer Research. 1982; 42(11): 4815-9.
- Shaw JH, Humberstone DM, Wolfe RR. Energy and protein metabolism in sarcoma patients. Annals of Surgery. 1988; 207(3): 283-9.
- Nitenberg G, Raynard B. Nutritional support of the cancer patient: issues and dilemmas. Crit Rev Oncol Hematol. 2000; 34(3): 137-68. Available from: URL: https://pubmed.ncbi.nlm.nih.gov/10838261/.
- Haran PH, Rivas DA, Fielding RA. Role and potential mechanisms of anabolic resistance in sarcopenia. J Cachexia Sarcopenia Muscle. 2012; 3(3): 157-62.
- Capitão C, Coutinho D, Neves PM, Capelas ML, Pimenta NM, et al. Protein intake and muscle mass maintenance in patients with cancer types with high prevalence of sarcopenia: A systematic review. Supportive Care in Cancer. 2022; 30(4): 3007-15.
- Bozzetti F, Bozzetti V. Is the intravenous supplementation of amino acid to cancer patients adequate? A critical appraisal of literature. Clin Nutr. 2013; 32(1): 142-6. Available from: URL: https: //pubmed.ncbi.nlm.nih.gov/23218120/.
- Martin WF, Armstrong LE, Rodriguez NR. Dietary protein intake and renal function. Nutr Metab (Lond). 2005; 2: 25.
- Remer T, Kalotai N, Amini AM, Lehmann A, Schmidt A, et al. Protein intake and risk of urolithiasis and kidney diseases: an umbrella review of systematic reviews for the evidence-based guideline of the German Nutrition Society. Eur J Nutr. 2023.
- Schoenfeld BJ, Aragon AA. How much protein can the body use in a single meal for muscle-building? Implications for daily protein distribution. J Int Soc Sports Nutr. 2018; 15: 10.
- Helms ER, Aragon AA, Fitschen PJ. Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. J Int Soc Sports Nutr. 2014; 11: 20.
- Antonio J, Peacock CA, Ellerbroek A, Fromhoff B, Silver T. The effects of consuming a high protein diet (4.4 g/kg/d) on body composition in resistance-trained individuals. J Int Soc Sports Nutr. 2014; 11: 19.
- Antonio J, Ellerbroek A, Silver T, Orris S, Scheiner M, et al. A high protein diet (3.4 g/kg/d) combined with a heavy resistance training program improves body composition in healthy trained men and women--a follow-up investigation. J Int Soc Sports Nutr. 2015; 12: 39.
- Antonio J, Ellerbroek A, Silver T, Vargas L, Peacock C. The effects of a high protein diet on indices of health and body composition--a crossover trial in resistance-trained men. J Int Soc Sports Nutr. 2016; 13: 3.
- Antonio J, Ellerbroek A, Silver T, Vargas L, Tamayo A, et al. A High Protein Diet Has No Harmful Effects: A One-Year Crossover Study in Resistance-Trained Males. J Nutr Metab. 2016; 2016: 9104792.
- Odelli C, Burgess D, Bateman L, Hughes A, Ackland S, et al. Nutrition support improves patient outcomes, treatment tolerance and admission characteristics in oesophageal cancer. Clin Oncol (R Coll Radiol). 2005; 17(8): 639-45.
- Paccagnella A, Morello M, Da Mosto MC, Baruffi C, Marcon ML, et al. Early nutritional intervention improves treatment tolerance and outcomes in head and neck cancer patients undergoing concurrent chemoradiotherapy. Supportive Care in Cancer. 2010; 18(7): 837-45.
- Cereda E, Turri A, Klersy C, Cappello S, Ferrari A, et al. Whey protein isolate supplementation improves body composition, muscle strength, and treatment tolerance in malnourished advanced cancer patients undergoing chemotherapy. Cancer Med. 2019; 8(16): 6923-32.
- Uster A, Ruefenacht U, Ruehlin M, Pless M, Siano M, et al. Influence of a nutritional intervention on dietary intake and quality of life in cancer patients: A randomized controlled trial. Nutrition. 2013; 29(11-12): 1342-9.
- Leedo E, Gade J, Granov S, Mellemgaard A, Klausen TW, et al. The Effect of a Home Delivery Meal Service of Energy- and Protein-Rich Meals on Quality of Life in Malnourished Outpatients Suffering from Lung Cancer: A Randomized Controlled Trial. Nutrition and Cancer. 2017; 69(3): 444-53.
- Krüger J, Meffert PJ, Vogt LJ, Gärtner S, Steveling A, al. Early Parenteral Nutrition in Patients with Biliopancreatic Mass Lesions, a Prospective, Randomized Intervention Trial. PLOS ONE. 2016; 11(11): e0166513.
- Gavazzi C, Colatruglio S, Valoriani F, Mazzaferro V, Sabbatini A, et al. Impact of home enteral nutrition in malnourished patients with upper gastrointestinal cancer: A multicentre randomised clinical trial. European journal of cancer (Oxford, England: 1990). 2016; 64: 107-12. Available from: URL: https: //pubmed.ncbi.nlm.nih.gov/27391922/.
- Laird BJ, Kaasa S, McMillan DC, Fallon MT, Hjermstad MJ, et al. Prognostic factors in patients with advanced cancer: a comparison of clinicopathological factors and the development of an inflammation-based prognostic system. Clin Cancer Res. 2013; 19(19): 5456-64.
- Porter Starr KN, Orenduff M, McDonald SR, Mulder H, Sloane R, et al. Influence of Weight Reduction and Enhanced Protein Intake on Biomarkers of Inflammation in Older Adults with Obesity. J Nutr Gerontol Geriatr. 2019; 38(1): 33-49.
- McMillan DC. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat Rev. 2013; 39(5): 534-40.
- Moses AW, Slater C, Preston T, Barber MD, Fearon KC. Reduced total energy expenditure and physical activity in cachectic patients with pancreatic cancer can be modulated by an energy and protein dense oral supplement enriched with n-3 fatty acids. British Journal of Cancer. 2004; 90(5): 996-1002