
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Association between number of Barrett’s esophagus risk factors and disease prevalence
Bashar Qumseya1*; Shuang Yang2; Yi Guo2
1Division of Gastroenterology, Hepatology and Nutrition, University of Florida, Gainesville, Florida, USA.
2Department of Health Outcomes and Biomedical Informatics, College of Medicine, University of Florida, Gainesville, Florida, USA.
*Corresponding Author : Bashar Qumseya
Associate Professor, Division of Gastroenterology, Hepatology and Nutrition, University of Florida, P.O. Box 100214,
1329 SW 16th St., Suite 5251, Gainesville, FL 32610-0214, USA.
Email: bqumseya@ufl.edu
Received : Jan 08, 2024
Accepted : Feb 05, 2024
Published : Feb 12, 2024
Archived : www.jjgastro.com
Copyright : © Qumseya B (2024).
Abstract
Introduction: Current clinical practice guidelines recommend screening endoscopy for patients with multiple Barrett’s Esophagus (BE) risk factors. However, there is only indirect evidence that BE risk factors are additive. We aimed to investigate the association between BE risk factors and BE prevalence in patients with GERD.
Methods: This analysis was conducted using the electronic health record data from the One Florida Clinical Data Research Network. The primary outcome of interest was the prevalence of BE in patients, based on the number of BE risk factors. Linear regression analysis was used to assess the association between the number of risk factors and BE. We report the beta coefficients and p-values. We used the chi-square test to examine differences between proportions.
Result: The database included 6,872,194 adult patients. Overall, 5,223,305 patients had at least one BE risk factor, including GERD, male sex, white blood cell count, advanced age >50 years, or obesity. Logistic regression analysis showed that GERD was the most predictive of BE prevalence (OR=12.05 [11.6-12.5]). This was followed by age >50 years (odds ratio [OR]=2.6[2.5-2.7]), white race (OR=2.1[2.0-2.2]), and male sex (OR=1.53[1.49-1.57]). In the linear regression model, the number of BE risk factors was strongly associated with BE prevalence (beta=40, p<0.001).
Conclusion: In this multicenter, statewide, large cohort, the number of BE risk factors was positively associated with BE prevalence. These findings support the current practice guidelines that recommend screening for BE in patients multiple risk factors.
Keywords: Barrett’s esophagus; Risk factors; Prevalence; Gastroesophageal reflux disease; Obesity.
Abbrevations: BE: Barrett’s Esophagus; EC: Esophageal Cancer; GERD: Gastroesophageal Reflux Disease; NDBE: Non-Dysplastic BE; LGD: Low-Grade Dysplasia; HGD: HighGrade Dysplasia; IMC: Intramucosal Cancer; ICD: International Classification Of Disease; IRB: Institutional Review Board; OR: Odds Ratio.
Citation: Qumseya B, Yang S, Guo Y. Association between number of Barrett’s esophagus risk factors and disease prevalence. J Gastroenterol Res Pract. 2024; 4(1): 1180.
Introduction
Gastroesophageal Reflux Disease (GERD) is a common medical condition affecting up to 28% of the US general population [1]. GERD is a primary risk factor for Barrett’s Esophagus (BE) and esophageal adenocarcinoma (EAC), a leading cause of cancer mortality in Western countries [2]. The incidence of BE and EAC has increased in recent decades [2-4]. Various risk factors can be associated with BE and EAC, including GERD, white race, advanced age, obesity, smoking, and a family history of BE or EAC [5-9]. Therefore, there has been much interest in standardizing guidelines to screen for BE to stem the tide of the BE and EAC waves. Current guidelines from multiple national societies recommend screening high-risk individuals for BE. While societies vary in their definition of who is at high risk, most guidelines recommend screening patients with multiple risk factors [10- 12]. Despite near unanimous agreement on screening patients with multiple risk factors, we lack a sufficient understanding of how BE risk factors interact. However, indirect data from a meta-analysis, which we published earlier, indicate that more risk factors lead to an increased risk of BE [6]. However, this data has not been substantiated using direct evidence. Additionally, the same data suggest that different risk factors increase the risk of BE variably [6]. In a recent meta-analysis, we reported that the prevalence of BE in patients with GERD was 3%, whereas the prevalence in obese patients undergoing pre-bariatric endoscopy was only 0.9% [5]. Therefore, the risk of BE conferred by GERD appears to be greater than that of obesity alone. Analyzing the potential relationships between these risk factors may help us better understand who is at most risk for BE and, thus, better stratify patients who may benefit from screening for BE. In this study, we aimed to conduct a cross-sectional analysis of a multicenter large database to better understand the potential interactions between various BE risk factors. We hypothesized that an increased number of BE risk factors would be linearly associated with an increased prevalence of BE.
Methods
Database
This analysis was conducted using Electronic Health Record (EHR) data from the OneFlorida Clinical Data Research Network [13]. This database comprises a network of 11 healthcare systems based in Florida that provides healthcare to a large proportion of Floridians (>40%). The data include healthcare claims and EHR, including de-identified data on procedures, laboratory testing, diagnoses, vital signs, and medications.
Inclusion criteria
All adult patients (aged >18 years) with one entry in the database were included in this study. The study dates were between 2012 and 2019. Patients who reached the age threshold during the study period were included in this analysis. We used the International Classification of Disease (ICD) 9th and 10th revisions to identify patients with GERD and the Current Procedural Terminology (CPT) codes to identify patients who underwent an endoscopic procedure after their GERD diagnosis. ICD codes were also used to identify patients with BE (with or without dysplasia).
Outcomes and definitions
The primary outcome of interest was the prevalence of BE (per 100,000 patients) stratified by the number of BE risk factors. These risk factors were identified from the EHR and included age (continuous and dichotomous), race (white vs. other), smoking status (current vs. other), and obesity (defined as Body Mass Index [BMI] >30 kg/m2 ). Chronic GERD was defined as three or more GERD diagnoses during the research period, and any of the two diagnoses were at least 6 months apart. We used RxNorm Concept Unique Identified (RXCUI) and national drug code directory (NDC) codes to identify Proton-pump inhibitor (PPI) medication use. Chronic PPI use was defined as having 3 or more orders of PPI at least 30 days apart. We identified census tract-level residency (urban vs. rural), poverty-level status (poverty level <15% vs. ≥15%), and six types of payers. The data were further stratified according to sex (male vs. female). The study was approved by the IRB of the University of Florida. The definitions of all the data variables are included in the Appendix.
Statistical analysis
All statistical analyses were performed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA). We used the chi-squared test for differences between proportions and t-tests for continuous variables. Multivariable logistic regression was performed to examine the potential association between BE prevalence and age, race, obesity, sex, GERD, and chronic PPI use as predictors, adjusting for residence poverty and payer. We calculated two-sided p-values for all statistical analyses and considered a significance level of 0.05. Linear regression analysis was used to assess the association between the number of risk factors and BE prevalence. We report the beta coefficient, R2 , and p-values.
Results
Our database included 6,872,194 adult patients [43.4% (n=2,984,608) males and 56.6% (n=3,887,585) females]. Of these, 24% (n=1,648,889) had no risk factors for BE, (76% (n=5,223,305) had at least one BE risk factor. Overall, 12.1% (n=831,445) of the patients had been diagnosed with GERD, and 3.44% (n=236,517) had chronic GERD. Among patients with GERD, 19.3% (n=160,590) underwent upper endoscopy (EGD). Patient characteristics are summarized in Table 1.
The prevalence of BE was .45% (n=31,188) and was higher in males (.54%) than females (.39%), p<0.001. The prevalence of BE among patients with GERD was much higher than that in the general population (3.8% in male and 2.4% in females).
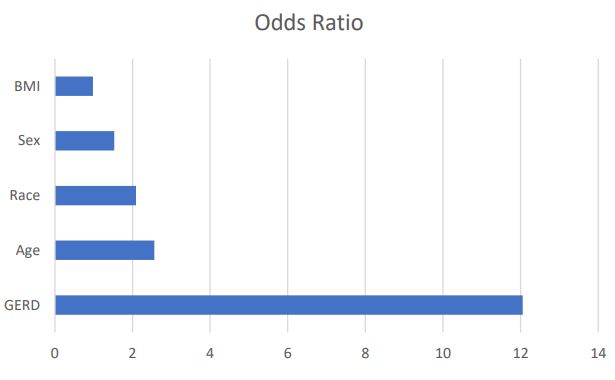
Overall, 5,223,305 patients had at least one BE risk factor, including GERD, male sex, white blood cell count, advanced age >50 years, or obesity. On logistic regression analysis, when adjusting for residence-poverty and health insurance, GERD was the most predictive of BE prevalence (OR=12.05 [11.6-12.5]). This was followed by age >50 years (odds ratio [OR]=2.6[2.5- 2.7]), white race (OR=2.1[2.0-2.2]), and male sex (OR=1.53 [1.49-1.57]). However, obesity did not confer a higher BE rate in this population (0.98 [0.96, 1.01]) (Table 2, Figure 1).
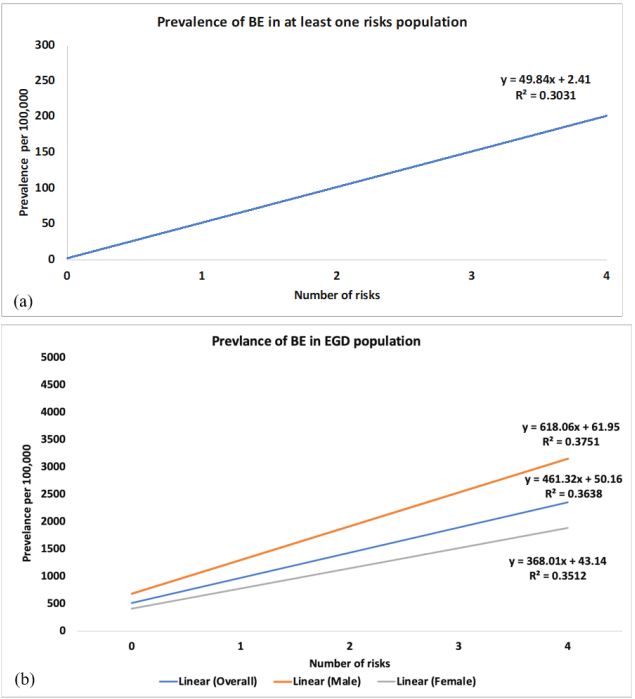
We divided the patients into risk categories based on the number of risk factors (from no risk factors to four risk factors). In the linear regression model, the number of BE risk factors was strongly associated with BE prevalence (beta=49, p<0.001, Figure 2a). Thus, for each additional BE risk factor, the prevalence of BE increased by 49 per 100,000 population, with R2 of 0.3.
In a sub-analysis, we restricted the data to patients who underwent EGD (n=160,590) because the true prevalence of BE may be underestimated in patients with GERD who did not undergo EGD. The overall trend of BE prevalence in relation to the number of risk factors remained unchanged. The prevalence of BE in males increased from 680 per 100,000 to 2,534 per 100,000 as the number of risk factors increased (beta coefficient=618, R2 =0.38 for males (Figure 2b). This translated to a 0.62% increase in BE prevalence for each additional risk factor in males.
Table 1: Baseline patient characteristics of the study cohort, adults with at least one be Barrett’s esophagus risk factor.
| Category | Value | Overall N=5,223,305 |
|---|---|---|
| Age (years) | Mean (SD) | 52.2 (26.2) |
| <50 | 2,562,582 (49.1%) | |
| >50 | 2,660,723 (50.9%) | |
| Race | White | 3,104,625 (50.3%) |
| Other | 2,118,680 (49.7%) | |
| EGD | Yes | 219,069 (4.2%) |
| No | 5,004,236 (95.8%) | |
| Chronic GERD | Yes | 234,316 (4.5%) |
| No | 4,988,989 (95.5%) | |
| Chronic PPI use | Yes | 158,241 (3%) |
| No | 5,065,064 (97%) | |
| BMI | >30 | 1,204,859 (38.3%) |
| <30 | 1,939,620 (61.7%) | |
| Missing | 2078826 | |
| Residence-Poverty | Rural, poverty<15% | 2,119,787 (52.4%) |
| Rural, poverty>15% | 1,353,526 (33.4%) | |
| Urban poverty<15% | 358,649 (8.9%) | |
| Urban poverty>15% | 215,887 (5.3%) | |
| Missing | 1,175,456 | |
| Current smoker | Yes | 222,795 (41.8%) |
| No | 310,299 (58.2%) | |
| Missing | 4,690,211 | |
| Payer | Medicare | 1,006,418 (22.9%) |
| Medicaid | 490,212 (11.2%) | |
| Private insurance | 1,708,808 (38.9%) | |
| Managed care | 4,255,615 (9.7%) | |
| No insurance | 3,530,981 (8%) | |
| Miscellaneous | 412,659 (9.4%) | |
| Missing | 826,495 |
Table 2: Multivariable logistic regression estimating prevalence of BE among adults with at least one risk factor.
| Patients with at least one risk factors (N=5,223,305) | ||
|---|---|---|
| Variables | Adjusted OR (95% CI) | p-value |
| Sex | ||
| Male vs. Female | 1.53 (1.49, 1.57) | <0.001 |
| Race | ||
| White vs. other | 2.09 (2.02, 2.16) | <0.001 |
| Age | ||
| >=50 vs. <50 | 2.56 (2.47, 2.66) | <0.001 |
| GERD | ||
| Yes vs No | 12.05 (11.64,12.48) | <0.001 |
| BMI | ||
| >=30 vs. <30 | 0.98 (0.96, 1.01) | 0.258 |
| Residence-Poverty | ||
| Rural,poverty>=15% vs Rural,poverty<15% | 086 (0.83, 0.89) | <0.001 |
| Urban,poverty<15% vs Rural,poverty<15% | 0.89 (0.85, 0.93) | <0.001 |
| Urban,poverty >=15% vs Rural,poverty<15% | 0.81 (0.77, 0.86) | <0.001 |
| Payer | ||
| Medicaid vs. Private | 0.92 (0.89, 0.95) | <0.001 |
| Medicare vs. Private | 0.80 (0.76, 0.84) | <0.001 |
| Managed care vs. Private | 0.56 (0.52,0.59) | <0.001 |
| No insurance vs. Private | 0.56 (0.51, 0.62) | <0.001 |
| Miscellaneours vs. Private | 0.62 (0.59, 0.65) | <0.001 |
Discussion
In this study, we used a multicenter, state-wide, real-world, large database to assess the strength of the association between BE risk factors and its prevalence. We reported that BE risk factors conferred variable risk of BE, with GERD being the most predictive, followed by age >50 years, white race, and male sex. Furthermore, we reported that the number of BE risk factors was positively associated with the prevalence of BE; as the number of BE risk factors increased, the risk of BE increased linearly. This trend was true for both males and females but was more pronounced in males.
Esophageal adenocarcinoma is a leading cause of cancerrelated deaths in West [14,15]. There are several risk factors for EAC, however, BE is the only treatable risk factor [16,17]. This precursor condition develops when there is a change in the normal squamous lining of the esophageal mucosa into intestinal metaplasia. There is progression from no dysplasia to Low-Grade Dysplasia (LGD), High-Grade Dysplasia (HGD), Intramucosal Carcinoma (IMC), and invasive EAC [18,19]. Despite improvements in detection and treatment options, the incidence of BE and EAC has dramatically increased in recent decades [2,3]. Most GI societies recommend BE screening of patients with multiple risk factors [10,20,21]. However, there were two major concerns regarding these recommendations. First, until now, there as only been indirect evidence showing that an increasing number of risk factors are associated with an increased risk of BE. We published data from a meta-analysis in which we showed that studies of patients with more BE risk factors were associated with a mild increase in the prevalence of BE [6]. This data was based on a meta-regression analysis. In a meta-regression, we use study-based data and not individualbased data. Therefore, we wanted to confirm these results using our current study design. We believe that the current results are an important addition to fill in the knowledge gap regarding the additivity of BE risk factors.
n the previous meta-analysis, we reported that each increase in one BE risk factor was associated with a 1.7% increase in the risk of BE. In the current study, we found that each additional BE risk factor increased the probability of BE by 0.68%. To our knowledge, this is the first study using a large database to confirm this important trend. These results support current recommendations for screening patients with multiple BE risk factors.
Although the magnitude of this increase may seem trivial, it is clinically relevant. Assuming a prevalence of .5% of BE in the general population [22,23], a population of patients with five BE risk factors (i.e., male sex, GERD, Age >50 years, white, and obesity) will have a predicted prevalence of 3.6% (0.5%+[0.62x5]). In our opinion, such BE prevalence would warrant screening for BE in this patient population, as currently recommended by most GI societies.
In addition, this study provides further evidence that BE risk factors are unequal. Therefore, current recommendations [10,12] for screening patients with multiple risk factors are not sufficiently specific. For example, a white obese female will have a much lower risk of BE than a male with chronic GERD. The former is less likely to benefit from screening, whereas the latter is. Therefore, our analysis identified GERD and age>50 as the two most important predictors. These results are in line with those of published studies showing that GERD is the most important BE risk factor. In a case-control study, Anderson et al. [24] reported an unadjusted OR of 12, which was remarkably similar to the adjusted OR reported here. In our study, the next most important factor was advanced age, which has not been reported in previous studies [25-27]. Clinically, however, this is one of the most important risk factors for BE. Based on these results, initiating screening around the age of 50 years, who also have other risk factors, would make the most sense and would be in line with colorectal cancer screening guidance. Therefore, screening criteria should be developed to reflect the varying risks inferred by each risk factor.
Strengths and limitations
Our study has several strengths. It is a multicenter, statewide, large database study of millions of patients and thus provides real-world experience on BE and its risk factors. However, as with any large-database study, there are inherent limitations. These included missing data, miscoding, and loss to follow-up, and the use of ICD and CPT codes. BE is a histologic diagnosis. Relying on ICD codes for this diagnosis introduces obvious limitations. We attempted to address these limitations in the study design and statistical analysis. Additionally, the true prevalence of BE in the population may be inaccurate since many patients are likely to have BE but have never been diagnosed. We adjusted for this in a sensitivity analysis of BE risk among patients who underwent endoscopy only, and the results were similar in trend and magnitude. Lastly, these results, despite being multicentered, originated from one state, thus questioning their generalizability to a national level. However, previous studies have already shown that the results of this large dataset are similar to those of national datasets [28]. Therefore, we believe that our results are generalizable.
Conclusion
Several risk factors are associated with BE and EAC. This study showed that more risk factors are associated with a higher prevalence of BE. These data support the current guidelines that patients with multiple risk factors are at an increased risk for BE and may benefit from screening.
Declarations
Funding: University of Florida.
Conflicts of interest/competing interests: Dr. Qumseya is a consultant for Medtronic and Assertio Management and has received travel reimbursement from Castle Biosciences.
Data transparency statement: Data, analytical methods, and study materials will be made available to other researchers, as requested by the corresponding author.
References
- El-Serag HB, Sweet S, Winchester CC, et al. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2014; 63: 871-80.
- Hur C, Miller M, Kong CY, et al. Trends in esophageal adenocarcinoma incidence and mortality. Cancer. 2013; 119: 1149-58.
- de Jonge PJ, van Blankenstein M, Grady WM, et al. Barrett’s oesophagus: epidemiology, cancer risk and implications for management. Gut. 2014; 63: 191-202.
- Schoppmann SF, Asari R, Riegler M. Barrett’s esophagus as a marker for increased risk for esophageal cancer and cardiorespiratory disease. Endoscopy. 2013; 45: 152.
- Qumseya B, Gendy S, Wallace A, et al. Prevalence of Barrett’s esophagus in obese patients undergoing pre-bariatric surgery evaluation: a systematic review and meta-analysis. Endoscopy. 2020.
- Qumseya BJ, Bukannan A, Gendy S, et al. Systematic review and meta-analysis of prevalence and risk factors for Barrett’s esophagus. Gastrointest Endosc. 2019; 90: 707-717 e1.
- Lee SW, Lien HC, Chang CS, et al. Differences of risk factors and clinical presentations in male and female Taiwanese individuals with Barrett’s esophagus. J Chin Med Assoc. 2018; 81: 860-864.
- Dong J, Buas MF, Gharahkhani P, et al. Determining Risk of Barrett’s Esophagus and Esophageal Adenocarcinoma Based on Epidemiologic Factors and Genetic Variants. Gastroenterology. 2018; 154: 1273-1281 e3.
- Yachimski P. Modifiable Risk Factors for Barrett’s Esophagus and Esophageal Adenocarcinoma: Still a Shot in the Dark. Clin Gastroenterol Hepatol. 2016; 14: 773-4.
- Asge Standards Of Practice C, Qumseya B, Sultan S, et al. ASGE guideline on screening and surveillance of Barrett’s esophagus. Gastrointest Endosc. 2019; 90: 335-359 e2.
- Shaheen NJ, Falk GW, Iyer PG, et al. Diagnosis and Management of Barrett’s Esophagus: An Updated ACG Guideline. Am J Gastroenterol. 2022; 117: 559-587.
- Muthusamy VR, Wani S, Gyawali CP, et al. AGA Clinical Practice Update on New Technology and Innovation for Surveillance and Screening in Barrett’s Esophagus: Expert Review. Clin Gastroenterol Hepatol. 2022; 20: 2696-2706 e1.
- Hogan WR, Shenkman EA, Robinson T, et al. The OneFlorida Data Trust: a centralized, translational research data infrastructure of statewide scope. J Am Med Inform Assoc. 2022; 29: 686-693.
- Njei B, McCarty TR, Birk JW. Trends in esophageal cancer survival in United States adults from 1973 to 2009: A SEER database analysis. J Gastroenterol Hepatol. 2016; 31: 1141-6.
- Sawas T, Katzka DA. Esophageal adenocarcinoma phenotypes and risk factors. Curr Opin Gastroenterol. 2022; 38: 423-427.
- Wang SE, Kendall BJ, Hodge AM, et al. Demographic and lifestyle risk factors for gastroesophageal reflux disease and Barrett’s esophagus in Australia. Dis Esophagus. 2022; 35.
- Kubota D, Takahashi Y, Yamamichi N, et al. Analysis of Barrett’s Esophagus and Its Risk Factors: A Cross-Sectional Study of 10,122 Subjects at a Japanese Health Examination Center. Digestion. 2022; 103: 411-420.
- O’Byrne LM, Witherspoon J, Verhage RJJ, et al. Barrett’s Registry Collaboration of academic centers in Ireland reveals high progression rate of low-grade dysplasia and low risk from nondysplastic Barrett’s esophagus: report of the RIBBON network. Dis Esophagus. 2020.
- Kambhampati S, Tieu AH, Luber B, et al. Risk Factors for Progression of Barrett’s Esophagus to High Grade Dysplasia and Esophageal Adenocarcinoma. Sci Rep. 2020; 10: 4899.
- Shaheen NJ, Falk GW, Iyer PG, et al. ACG Clinical Guideline: Diagnosis and Management of Barrett’s Esophagus. Am J Gastroenterol. 2016; 111: 30-50; quiz 51.
- Spechler SJ, Sharma P, et al. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology. 2011; 140: 1084-91.
- Runge TM, Abrams JA, Shaheen NJ. Epidemiology of Barrett’s Esophagus and Esophageal Adenocarcinoma. Gastroenterol Clin North Am. 2015; 44: 203-31.
- Qumseya B, Gendy S, Wallace A, et al. Prevalence of Barrett’s esophagus in obese patients undergoing pre-bariatric surgery evaluation: a systematic review and meta-analysis. Endoscopy. 2020; 52: 537-547.
- 24. Anderson LA, Watson RG, Murphy SJ, et al. Risk factors for Barrett’s oesophagus and oesophageal adenocarcinoma: results from the FINBAR study. World J Gastroenterol. 2007; 13: 1585-94.
- Cameron AJ, Lagergren J, Henriksson C, et al. Gastroesophageal reflux disease in monozygotic and dizygotic twins. Gastroenterology. 2002; 122: 55-9.
- Ford AC, Forman D, Reynolds PD, et al. Ethnicity, gender, and socioeconomic status as risk factors for esophagitis and Barrett’s esophagus. Am J Epidemiol. 2005; 162: 454-60.
- Abrams JA, Fields S, Lightdale CJ, et al. Racial and ethnic disparities in the prevalence of Barrett’s esophagus among patients who undergo upper endoscopy. Clin Gastroenterol Hepatol. 2008; 6: 30-4.
- He Z, Bian J, Carretta HJ, et al. Prevalence of Multiple Chronic Conditions Among Older Adults in Florida and the United States: Comparative Analysis of the OneFlorida Data Trust and National Inpatient Sample. J Med Internet Res. 2018; 20: e137.