
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 4
Impact of radiotherapy on rectal goblet cells
Jessica Yancey*; Xiaoqin Zhu; Shirin Sioshansi
Department of Radiation Oncology, UMass Memorial Medical Center and UMass Chan Medical School, Worcester, MA, USA.
*Corresponding Author : Jessica Yancey
Department of Radiation Oncology, UMass Memorial Medical Center and UMass Chan Medical School,
Worcester, MA, USA.
Tel: 978-343-5196 & 978-343-5151;
Email: yanceyj@umassmemorial.org
Received : Jan 04, 2024
Accepted : Jan 25, 2024
Published : Feb 01, 2024
Archived : www.jjgastro.com
Copyright : © Yancey J (2024).
Abstract
Introduction: We investigated if irreversible radiation damage to the rectum directly impacts goblet cells and if this could impart explain the pathophysiology of radiation proctitis.
Methods: We conducted a single institution retrospective review identifying two patient cohorts with rectal and anal cancers (T1-4N0-1M0). One cohort underwent external beam radiation therapy followed by resection and the other cohort underwent resection alone. Pathologic specimens were reviewed to evaluate paneth cell metaplasia, chronic colitis, active colitis, number of goblet cells per crypt, nuclei per crypt, percent of goblet cells per crypt, and hyperplastic changes. In parallel, charts were reviewed for staging, treatment details, reason for surgery, flexible sigmoidoscopy/colonoscopy findings and signs or symptoms of radiation proctitis.
Results: Surgical specimens were obtained for a total of 13 patients in the investigational (those who received radiation followed by surgery) arm and 16 patients in the control (surgery alone) arm. Radiation doses ranged from 50.4-54Gy. Time to surgery was a median of 517 days after radiation. Each surgical specimen was evaluated at the margin of the specimen and at the tissue adjacent to tumor. No differences were found between the two cohorts with respect to the number of goblet cells per crypt, nuclei per crypt and percent goblet cells per crypt.
Conclusions: There was no difference in the number of goblet cells per crypt, nuclei per crypt or percent of goblet cells per crypt between radiated and un-irradiated rectal tissue specimens.
Keywords: Radiation proctitis; Goblet cells; Radiotherapy; Rectal cancer; Anal cancer.
Citation: Yancey J, Zhu X, Sioshansi S. Impact of radiotherapy on rectal goblet cells. J Gastroenterol Res Pract. 2024; 4(1): 1178.
Introduction
Radiation therapy is often a key component of curative treatment for pelvic malignancies. With the goal of cure comes the management of treatment related toxicities. About 5-10% of patients undergoing pelvic radiation therapy experience acute radiation proctitis (radiation-induced damage to the lining of the rectum) and up to 43% experience chronic or late radiation proctitis. Endoscopic evaluation of acute rectal proctitis demonstrates mucosal ulceration, edema, erythema, and bleeding [1]. There are no treatment guidelines for management of radiation proctitis. And therefore, treatments are based on single institution experiences, such as anti-inflammatory agents, anti-oxidants, formalin application, or hyperbaric oxygen with endoscopic argon plasma coagulation and surgery reserved for refractory cases [2].
In this paper we raised the hypothesis that irreversible radiation damage in the rectum directly impacts acute and chronic mucin production, which in turn potentially contributes to and exacerbates radiation proctitis by causing a “dry” rectum. Goblet cells in the large intestine contains produce mucin, providing a barrier to pathogenic bacteria [3]. Mucin also lubricates the fecal stream [1], similar to how saliva lubricates a food bolus. A corollary can therefore be drawn to impact of radiation on glandular cells in different parts of the body. Radiation for head and neck cancers commonly leads to xerostomia. At a cellular level radiation injures plasma cell membranes of secretory cells, disrupting muscarinic receptor stimulated water secretion in addition to acinar cell loss and fibrosis of periductal and intralobular cells [4]. Radiation to vaginal tissue leading to desquamation, adhesions, thinning and dryness [5,6]. Similarly, radiation to the skin can cause xerotic skin as a result of glandular cells becoming less productive [7]. If radiation impacts the glandular cells (or Goblet cells) in the rectum similarly to how it impacts glandular cells in other parts of the body, then theoretically it could result in a decrease of mucin production leading to discomfort and difficulty passing stool. Furthermore, if such a relationship exists, better understanding the injury to the goblet cells can better guide therapies to aid in radiation proctitis.
Through evaluation of pathological specimens from patients who have completed definitive radiation treatment to rectum or anus we hope to better understand the late effects on goblet cells and mucin production.
Background on rectal anatomy
The intestinal tract plays an important role in digestion, absorption, waste production, and immunity [8]. It consists of 4 cell types: Absorptive enterocytes, goblet cells, paneth cells, and enteroendocrine cells [8]. Goblet cells arise from undifferentiated cells in the base of crypts of Lieberkühn and divide every 4-8 days. The precent of goblet cells increase from duodenum to the rectum [8]. Goblet cells produce a gel like mucin made of up 98% water, which helps to lubricate the fecal stream [1,8]. Mucin also protects the epithelium through formation of both a firmly and loosely adherent mucus layer [9]. Breakdown of mucin can lead to inflammation or injury, such as in colitis [10].
Methods & materials
We performed a single institution retrospective review at UMass Memorial Medical Center to identify patients diagnosed with non-metastatic (T1-T4N0-1M0) rectal and anal cancers who underwent external beam radiation therapy as part of definitive therapy followed by surgical resection or biopsy of rectal tissue at least 60 days after treatment completion. Surgical resection was due to recurrence in all but 2 patients. In addition, a list of control subjects were identified with early stage (T1- 2N0M0) rectal cancer who underwent surgical resection alone for definitive therapy. Patients were identified through quiring the UMass Cancer Registry for individuals over the age of 18 with rectal or anal cancer diagnosis between the years of 2011- 2021. 13 patients in the investigational (radiation followed by surgery) arm and 16 patients in the control (surgery alone) arm were identified with pathological specimens available. Pathology specimens were obtained through the UMass Pathology Department. One pathologist reviewed all specimens documenting paneth cell metaplasia, chronic colitis, active colitis, number of goblet cells per crypt, nuclei per crypt, percent of goblet cells per crypt, and hyperplastic changes. In parallel patient records were reviewed in EPIC and MOSAIQ to document cancer stage, primary site of disease (rectal or anal), age at diagnosis, date of diagnosis, start and completion dates of radiation, radiation dose to rectum, chemotherapy (if given), date of surgery, days between radiation completion and surgery, flexible sigmoidoscopy/colonoscopy findings and symptoms of rectal proctitis at time of surgery.
Results
Of the 13 patients in the investigational arm, the median age was 61. Cancer diagnosis included 8 patients with rectal cancer and 5 with anal cancer. Indication for surgery was disease progression in 11 patients and delayed standard treatment in 2. Delayed standard treatment occurred at 61 days in both of these patients. Of the 16 patients in the control arm, median age was 77. Cancer diagnosis included 15 rectal and 1 anal cancers. Indication for surgery was standard treatment for all patients. This data is represented in Table 1.
In the investigation arm, radiation doses ranged from 50.4- 54 Gy. All patients received concurrent chemotherapy. Time to surgery was at minimum 61 days and at maximum 1290 days. Median time to surgery was 517 days. Symptoms at time of surgery documented in EPIC included rectal bleeding, urgency and pain among a total of 7 patients. This data is represented in Table 2.
For each pathologic specimen, tissue was initially obtained and evaluated at the margin of the surgical specimen. However, given that the tissue at the margin may not have been within the radiation field (as margins were as large as 45 cm), additional pathological evaluation was performed on the tissue adjacent to the tumor which would have received radiation. The median distant to the mucosal margin was 24 cm in the investigational arm (range 1-45 cm) and 12 cm in the control arm (range 2.1-28 cm). Potential cofounding pathologic features included paneth cell metaplasia, chronic colitis, active colitis, and hyperplastic changes as reported in Table 3. Three variables were recorded for Goblet cells: number of goblet cells per crypt, nuclei per crypt and percent goblet cells per crypt. As demonstrated in Table 3 and Figures 1-6, all 3 variables were similar between the investigation and control arms.
Table 4 captures pathologic data on the 3 patients that had documented rectal bleeding at time of surgery. It is not known the cause of their rectal bleeding, which could be tumor or radiation related. Of note in this small subset of patients, there does appear to be a decrease in the number of goblet cells compared to the control and investigational arms, however the significance of this is unknown.
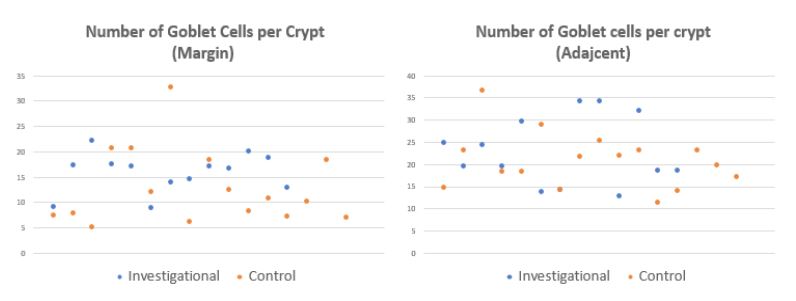
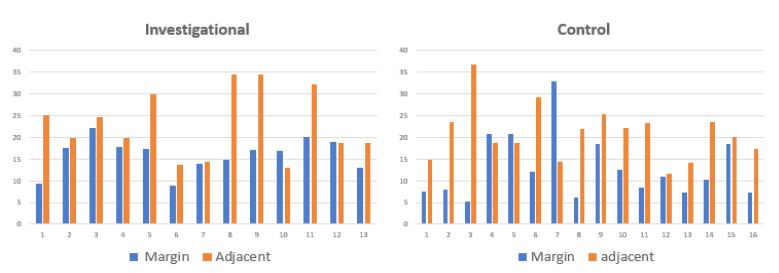
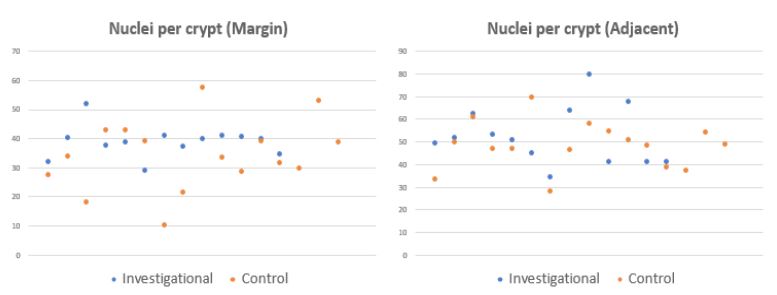
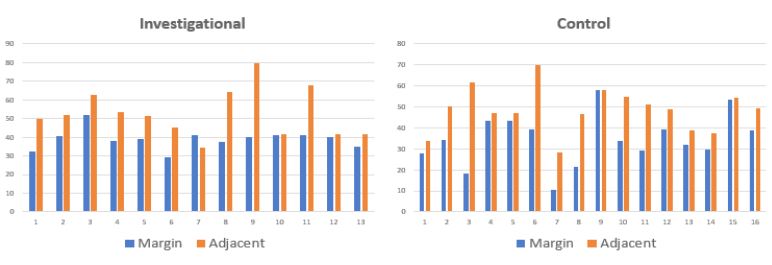
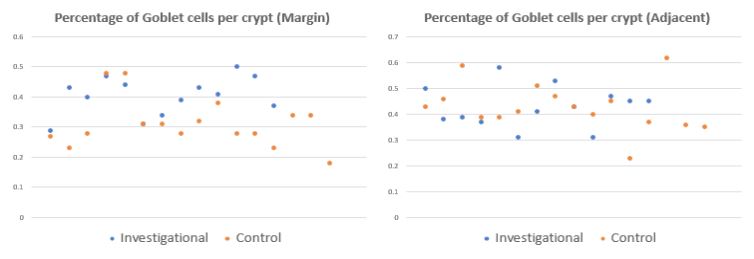
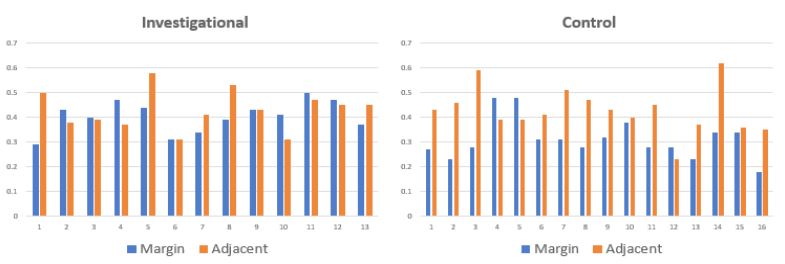
Table 1: Patient characteristics. conditions.
| Investigational (RT) | Control arm (No RT) | |
|---|---|---|
| Total number | 13 | 16 |
| Median age | 61 | 77 |
| Type of cancer | ||
| Rectal | 8 | 15 |
| Anal | 5 | 1 |
| Stage | ||
| T1-2 | 4 | 10 |
| T3 | 8 | 4 |
| T4 | 1 | 2 |
| NO or Nx | 8 | 11 |
| N1 | 4 | 4 |
| N2 | 1 | 1 |
| Reason for surgery | ||
| Standard treatment | 2 (both 61d) | 16 |
| Recurrence | 11 | N/A |
Table 2: Treatment details and symptoms in the investigational arm.
| Investigational arm | |
|---|---|
| Radiation dose | 50.4 - 54 Gy |
| Concurrent chemotherapy | 13 |
| Symptoms at time of surgery | |
| Recal Bleeding | 3 |
| Rectal Urgency | 2 |
| Rectal Pain | 5 |
| Total Pain | 7 |
| Interval between RT & Surgery | |
| Range (Days) | 6-1290 |
| Median (Days) | 517 |
Table 3: Details of pathologic features in investigation and control arms. conditions.
| Investigational (RT) | Control arm (No RT) | |||
|---|---|---|---|---|
| Margin mucosa | Adjacent mucosa | Margin mucosa | Adjacent mucosa | |
| Median distance to margin (cm) | 24 | N/A | 12 | N/A |
| Range of margin (cm) | 1-45 | N/A | 2.1 28 | N/A |
| Potential confounding pathology | ||||
| Paneth cell metaplasia | 1 | 3 | 0 | 0 |
| Chronic colitis | 0 | 2 | 0 | 0 |
| Active colitis | 0 | 0 | 0 | 0 |
| Hyperplastic changes | 3 | 5 | 2 | 9 |
| Number of goblet cells per crypt | ||||
| Range | 9.3 22.2 | 13- 34.4 | 7.6 -32.8 | 11.6 36.8 |
| Median | 17.2 | 19.8 | 10.6 | 20.9 |
| Nuclei per crypt | ||||
| Range | 29.3 52.1 | 34.6 79.8 | 10.4 57.8 | 28.4 70 |
| Median | 40.1 | 51.2 | 33.8 | 49 |
| Percentage of goblet cells per crypt | ||||
| Range | 29% 50% | 31% 58% | 18% 48% | 23% 59% |
| Median | 41% | 43% | 30% | 42% |
Table 4: Table 3 with addition of focus of 3 patients experiencing rectal bleeding at time of surgery.
| Subset of patients with rectal bleeding | ||||||
|---|---|---|---|---|---|---|
| Investigational (RT) | Control arm (No RT) | Rectal bleeding (3) | ||||
| Margin mucosa | Adjacent mucosa | Margin mucosa | Adjacent mucosa | Margin mucosa | Adjacent mucosa | |
| Median distance to margin (cm) | 24 | N/A | 12 | N/A | 18 | N/A |
| Range of margin (cm) | 1-45 | N/A | 2.1 28 | N/A | 6.5-29 | N/A |
| Potential confounding pathology | ||||||
| Paneth cell metaplasia | 1 | 3 | 0 | 0 | 0 | 0 |
| Chronic colitis | 0 | 2 | 0 | 0 | 0 | 1 |
| Active colitis | 0 | 0 | 0 | 0 | 0 | 0 |
| Hyperplastic changes | 3 | 5 | 2 | 9 | 0 | 1 |
| Number of goblet cells per crypt | ||||||
| Range | 9.3 22.2 | 13- 34.4 | 7.6 -32.8 | 11.6 36.8 | 14-17.3 | 13-29.8 |
| Median | 17.2 | 19.8 | 10.6 | 20.9 | 16.8 | 14.4 |
| Nuclei per crypt | ||||||
| Range | 29.3 52.1 | 34.6 79.8 | 10.4 57.8 | 28.4 70 | 38.9-41.1 | 34.6-51.2 |
| Median | 40.1 | 51.2 | 33.8 | 49 | 41.1 | 41.4 |
| Percentage of goblet cells/crypt | ||||||
| Range | 29% 50% | 31% 58% | 18% 48% | 23% 59% | 34% - 44% | 31% - 58% |
| Median | 41% | 43% | 30% | 42% | 41% | 41% |
Discussion
Although we hypothesized that radiation would impact goblet cells, there appeared to be no difference when quantifying the goblet cells in the radiated and un-irradiated specimens. However, there are multiple limitations to our data set. Initially, we identified 20 patients in each cohort. However, we were only able to obtain access to pathologic specimens in a total of 29 patients. In working with our pathologist 3 parameters were selected for goblet cell assessment: Number of goblet cells per crypt, nuclei per crypt, and percent of goblet cells per crypt. These parameters were selected surrogates for mucin production. In our dataset there appeared to be no difference in these parameters between the 2 arms. However, our assessment did not directly evaluate the function of the goblet cells or the degree of mucin production. Evaluation of mucin itself would have required additional mucin stains not currently available. This additional level of analysis was considered, but we not decided to pursue at this time as it would require additional resources and given our initial findings were not suggestive of a difference in outcomes.
Another challenge was correlating radiation dose to the tissue evaluated. Surgery was at time of recurrence with the general assumption the recurrence was in proximity to initial disease. However, it was not possible to directly assimilate the pathologic specimens to the exact radiation dose received by that tissue. We focused on the tissue adjacent to the tumor under the assumption this tissue was most likely within the radiation field. However, tumor effects on adjacent mucosa could also confound these results, as we do not know the impact tumor cells has on adjacent goblet cells, if any. It is possible that although radiation injures goblet cells, tumor may have the opposite effect. Many patients presenting with rectal or anal tumors report increased passage of mucous, prior to initiating any radiation therapy. Mucous production could be from the tumor cells themselves or impact on adjacent goblet cells. It is worth noting, when comparing the tissue adjacent to the tumor and tissue at the margin within each cohort there appears to be a trend towards increase in all 3 goblet cell variables within the adjacent tissue. This may be suggestive of a potential reactive response to the tumor causing an increase in goblet cells.
Despite our findings, rectal proctitis is a real and unfortunate sequalae of treatment for many patients, for which the pathophysiology remains unknown. Our inability to answer this question hopefully helps to aid in the direction of further investigation. As an improved understanding of rectal proctitis could help guide treatment approach.
Conclusion
In conclusion, we did not find a difference in the number of goblet cells per crypt, nuclei per crypt or percent of goblet cells per crypt between radiated and un-irradiated rectal tissue specimens, as proposed by our hypothesis. Further investigation is needed to further understand the pathophysiology of radiation proctitis which in turn will optimize treatment modalities.
References
- Fajardo, Luis Felipe et al. Radiation Pathology. Oxford University Press. 2001.
- Tabaja, Lameese, Shafik M. Sidani. Management of Radiation Proctitis.” Digestive Diseases and Sciences. 2018; 63(9): 2180-88.
- Jang Hyosun, Sunhoo Park, Janet Lee, Jae Kyung Myung, WonSuk Jang, et al. Rebamipide Alleviates Radiation-Induced Colitis through Improvement of Goblet Cell Differentiation in Mice. Journal of Gastroenterology and Hepatology. 2018; 33(4): 878-86.
- Jensen SB, Vissink A, Limesand KH, Reyland ME. Salivary Gland Hypofunction and Xerostomia in Head and Neck Radiation Patients. J Natl Cancer Inst Monogr. 2019; 2019(53): lgz016. doi: 10.1093/jncimonographs/lgz016.
- White ID. Sexual Difficulties after Pelvic Radiotherapy: Improving Clinical Management. Clin Oncol (R Coll Radiol). 2015; 27(11): 647-55. doi: 10.1016/j.clon.2015.06.018.
- Barraclough LH, Routledge JA, Farnell DJ, Burns MP, Swindell R, et al. Prospective analysis of patient-reported late toxicity following pelvic radiotherapy for gynaecological cancer. Radiother Oncol. 2012; 103(3): 327-32. doi: 10.1016/j.radonc.2012.04.018.
- Fitzgerald TJ, Jodoin MB, Tillman G, Aronowitz J, Pieters R, et al. Radiation therapy toxicity to the skin. Dermatol Clin. 2008; 26(1): 161-72, ix. doi: 10.1016/j.det.2007.08.005.
- Kim YS, Ho SB. Intestinal goblet cells and mucins in health and disease: recent insights and progress. Curr Gastroenterol Rep. 2010; 12(5): 319-30. doi: 10.1007/s11894-010-0131-2.
- Pelaseyed T, Bergström JH, Gustafsson JK, Ermund A, Birchenough GM, Schütte A, van der Post S, Svensson F, Rodríguez-Piñeiro AM, Nyström EE, Wising C, Johansson ME, Hansson GC. The mucus and mucins of the goblet cells and enterocytes provide the first defense line of the gastrointestinal tract and interact with the immune system. Immunol Rev. 2014; 260(1): 8-20. doi: 10.1111/imr.12182.
- McGuckin Michael A, Rajaraman Eri, Lisa A Simms, Timothy HJ Florin, Graham Radford-Smith. Intestinal Barrier Dysfunction in Inflammatory Bowel Diseases. Inflammatory Bowel Diseases. 2009; 15 (1): 100-113.