
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 3
Which tumor came first: Liver or the colon?
Charbel Karam1,2*; Mina Sarofim1,2; Miriam Fewtrell3; Matthew Morgan1,2
1Department of Colorectal Surgery, Bankstown-Lidcombe Hospital, NSW Australia.
2School of Medicine, University of New South Wales, NSW Australia.
3Department of Anatomical Pathology, Liverpool Hospital, NSW Australia.
*Corresponding Author : Charbel Karam
Department of Colorectal Surgery, Bankstown-Lidcombe
Hospital, NSW Australia.
Email: charbeljk@gmail.com
Received : Nov 05, 2023
Accepted : Dec 08, 2023
Published : Dec 15, 2023
Archived : www.jjgastro.com
Copyright : © Karam C (2023).
Citation: Karam C, Sarofim M, Fewtrell M, Morgan M. Which tumor came first: Liver or the colon?. J Gastroenterol Res Pract. 2023; 3(10): 1172.
Introduction
We present an extremely unusual diagnosis in an asymptomatic patient with a huge invasive, non-obstructive tumor involving the right colon and right lobe of the liver.
Case
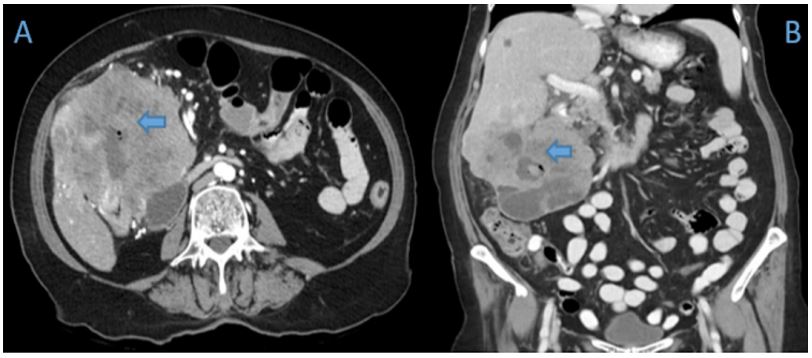
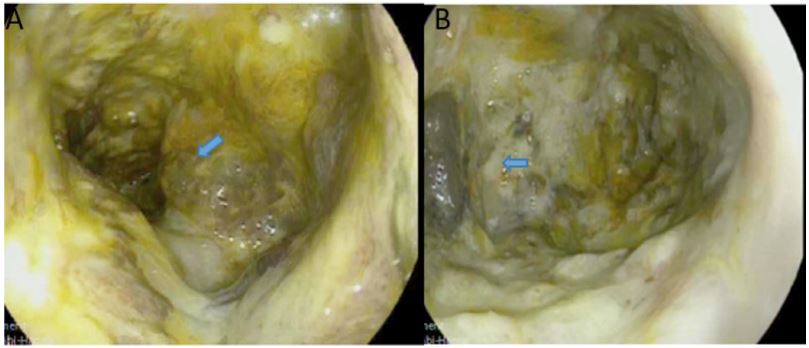
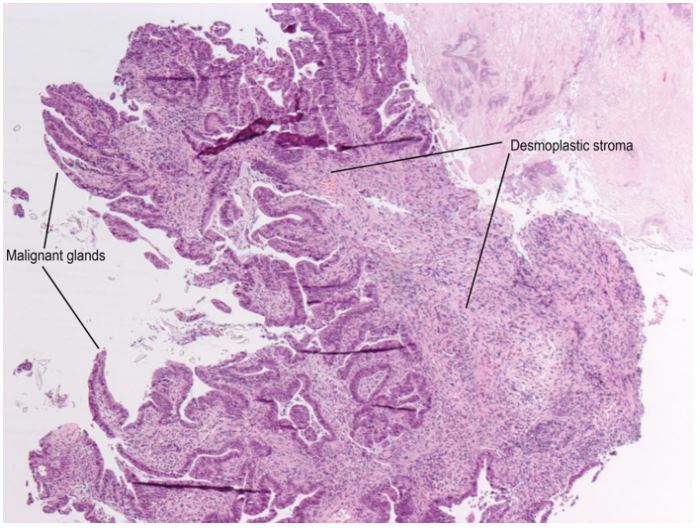
A 70-year old female was referred to the emergency department of a tertiary hospital by her general practitioner with a sixmonth history of lethargy, six-kilogram weight loss and vague right sided abdominal pain. She denied vomiting, altered bowel habit or rectal bleeding. Her relevant surgical history included cholecystectomy and thyroidectomy. There was no family history of colorectal cancer. Pertinent examination findings included a soft, non-distended abdomen with a large non-mobile palpable mass in the right upper quadrant. Her blood profile included leukocytosis (12.9 x109 /L), anaemia (Hb 79 g/L), normal bilirubin and mildly deranged liver function tests. Furthermore, she had a markedly raised CA 19.9 (5506 kU/L) and CEA (462.1 microg/L). She was admitted for a blood transfusion and further investigations. A triple phase computed tomography scan of the chest, abdomen and pelvis revealed an 11x10x10.5 cm hepatic flexure mass with invasion into the right hepatic lobe (Figure 1). Surprisingly, there was no evidence of colonic obstruction, nor distant metastatic disease. A colonoscopy demonstrated a large circumferential, fungating and partially obstructing mass extending into the ascending colon (Figure 2). Biopsy confirmed a poorly differentiated invasive adenocarcinoma (Figure 3). Following discussion at a multi-disciplinary surgical oncology meeting, she proceeded to an ileo-colonic bypass with planned adjuvant chemotherapy. Intra-operatively, the mass was invading the liver, with small amounts of ascites and no peritoneal metastasis. Proximal small and large bowel were of normal caliber. An ileo-colic side-to-side anastomosis was performed using the distal ileum and mid transverse colon. The patient made an uneventful recovery and was discharged day four post operatively with medical oncology follow up.
Discussion
Large bowel obstruction (LBO) is a surgical emergency most commonly due to colorectal neoplasms and are less frequently encountered compared with small bowel obstructions [1]. Other causes of LBO include diverticular strictures, volvulus and external compression from genitourinary malignancies. LBO can be classified as complete or incomplete. Characteristic symptoms of complete obstruction include obstipation, abdominal distension, pain and vomiting in the presence of a competent ileo-caecal valve. Symptoms of incomplete LBO are rather subtle including altered bowel habits with or without obstructive symptoms. Patients with a complete LBO are usually peritonitic, unwell and may present with colonic perforation in severe cases. Such patients require emergency surgical intervention including bowel resection with primary anastomoses, however septic patients usually warrant stoma formation or damage control surgery in the context of hostile abdominal cavities [2].
The risk of LBO in colorectal cancer increases with age and tumour size. Eighty percent of LBO are attributable to colonic neoplasms [2], 15-40% of patients presenting with obstructive symptoms [3]. The risk of perforation is 20% and is more common at the site of the tumor compared with proximal “blowout” perforations [2]. Furthermore, colonic obstruction and perforation have been shown to negatively correlate with patient outcome in the pre-operative and 5-year survivability in right sided colon cancers [4].
Most colonic neoplasms associated with LBO are less than six centimetres, however there is no correlation between tumour size and obstruction [5]. Nevertheless, larger masses are more likely to be associated with obstruction due to luminal narrowing and have an increased peritoneal metastatic potential due to a more aggressive tumour biology [6]. Interestingly, the patient in this case had a very large hepatic flexure neoplasm with hepatic invasion in the absence of obstruction, perforation and peritoneal metastases. Only one similar case has been previously reported [5].
Tumour location and growth rate may also influence the relationship between size and obstruction given that left sided colonic neoplasms are usually smaller than right sided lesions and are more often distal to the splenic flexure [7]. Furthermore, malignant colonic obstruction is more likely to involve the sigmoid colon [1] compared with the wider right colon characterised by slow growing tumours which are often advanced when associated with obstruction and may also have invaded surrounding structures. Additionally, right sided neoplasms have a higher TNM grade and biological aggressiveness in resected specimens [6].
Management of non-resectable large right colonic neoplasms can be challenging. Ileo-colic bypass surgery is recommended for intestinal continuity whilst adjuvant chemotherapy is useful for down staging large tumours, which may facilitate subsequent resection. Our decision to perform an ileo-colic anastomosis was in agreement with current guidelines [2] and of benefit to minimize the risk of complete LBO and associated mortality.
Disclosure statement: The authors declare no conflict of interest and no financial disclosure.
References
- Ramanathan S, Ojili V, Vassa R, Nagar A. Large Bowel Obstruction in the Emergency Department: Imaging Spectrum of Common and Uncommon Causes. J Clin Imaging Sci. 2017; 7: 15.
- Pisano, M, Zorcolo, L, Merli, C. et al. WSES guidelines on colon and rectal cancer emergencies: obstruction and perforation. World J Emerg Surg. 2017; 13: 36.
- Malakorn, S, Stein, S.L, Lee, J.H. et al. Urgent Management of Obstructing Colorectal Cancer: Divert, Stent, or Resect?. J Gastrointest Surg. 2019; 23: 425-432.
- Chen, T, Huang, Y. & Wang, G. Outcome of colon cancer initially presenting as colon perforation and obstruction. World J Surg Onc. 2017; 15: 164.
- Elyassi, A.R, Lin-Hurtubise, K. & Gagliano, R. Unusual sized cecal mass presenting without obstruction: a case report. Cases Journal. 2009; 2: 131.
- Saha S, Shaik M, Johnston G, Saha SK, Berbiglia L, Hicks M, Gernand J, Grewal S, Arora M, Wiese D. Tumor size predicts long-term survival in colon cancer: an analysis of the National Cancer Data Base. Am J Surg. 2015; 209: 570-S574.
- Webster, P.J, Aldoori, J. & Burke, D.A. Optimal management of malignant left-sided large bowel obstruction: do international guidelines agree?. World J Emerg Surg. 2019; 14: 23.