
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 3
Endoscopic features of helicobacter pylori-uninfected gastric malt lymphoma
Misako Tohata*; Yorimasa Yamamoto; Erika Yoshida; Kuniyo Gomi; Masatsugu Nagahama
Division of Gastroenterology, Department of Internal Medicine, Showa University Fujigaoka Hospital, Yokohama, Kanagawa, Japan.
*Corresponding Author : Misako Tohata
Division of Gastroenterology, Department of Internal Medicine, Showa University Fujigaoka Hospital,
Yokohama, Kanagawa, Japan.
Tel: +81-45-9711151;
Email: tohata335@gmail.com
Received : Oct 26, 2023
Accepted : Nov 20, 2023
Published : Nov 27, 2023
Archived : www.jjgastro.com
Copyright : © Tohata M (2023).
Abstract
Introduction: Mucosa-associated lymphoid tissue (MALT) lymphoma is a low-grade lymphoma that develops in extranodal organs (e.g., gastrointestinal tract, thyroid gland, and lungs) against the background of chronic inflammation. Approximately 80%-90% of gastric MALT lymphomas have Helicobacter pylori infection, but the percentage recently decreased to 30% in Europe and the United States. We often encountered H. pylori–uninfected gastric MALT lymphomas. Thus, we examined the characteristics of the endoscopic findings of H. pylori–uninfected gastric MALT lymphoma in affected patients admitted to our hospital, and compared them with H. pylori–positive cases and previously infected cases.
Methods: We retrospectively reviewed 15 patients (29 lesions) diagnosed with gastric MALT lymphoma via upper gastrointestinal endoscopy between February 2017 and February 2022. We classified 5 patients (10 lesions; 3 H. pylori–positive cases [8 lesions] and 2 previously infected cases [2 lesions]) as the HP group and 10 H. pylori–uninfected patients (19 lesions) as the non-HP group.
Results: MALT lymphoma that developed in the non-HP group had mainly discolored, depressed lesions with fold convergence on the greater curvatures of the body compared with that in the HP group. Importantly, more than 80% of patients in both groups had a tree-like appearance in the lesion under narrow-band imaging (NBI). Many received radiotherapy, and all were in remission.
Conclusions: Endoscopic findings of H. pylori–uninfected gastric MALT lymphoma included discolored lesions with fold convergence in the middle greater curvature of the body. NBI is useful for differentiating this malignancy from early gastric cancer.
Keywords: Endoscopy; Helicobacter pylori; Mucosa-associated lymphoid tissue lymphoma; Radiotherapy; Stomach.
Abbreviations: MALT: Mucosa-associated lymphoid tissue; NBI: Narrow-band imaging; TLA: Tree-like appearance.
Citation: Tohata M, Yamamoto Y, Yoshida E, Gomi K, Nagahama M. Endoscopic features of helicobacter pylori-uninfected gastric malt lymphoma. J Gastroenterol Res Pract. 2023; 3(9): 1169.
Introduction
In 1983, Isaacson first reported gastric lymphoma arising from mucosa-associated lymphoid tissue (MALT) as a low-grade gastric lymphoma [1]. However, MALT lymphoma can also develop in extranodal organs, such as the gastrointestinal tract, thyroid gland, and lungs, against the background of chronic inflammation. Helicobacter pylori infection was found in approximately 80%-90% of gastric MALT lymphomas [2], but in in Europe and the United States, the percentage declined to 30% in recent years [3]. Lately, we often encountered H. pylori–uninfected gastric MALT lymphomas. Endoscopic images of gastric MALT lymphoma are very diverse, and often show a morphology very similar to early gastric cancer or gastritis, making it one of the difficult diseases to diagnose. Currently, the characteristics of endoscopic findings of H. pylori–uninfected gastric MALT lymphoma are still seldom reported [4,5]. Thus, this study aimed to examine the characteristics of endoscopic findings of H. pylori–uninfected gastric MALT lymphoma from affected patients admitted to our hospital, and compared them with H. pylori–positive cases and previously infected cases.
Materials and methods
Patients: The institutional review board of Showa University approved this study (approval number: 22-242-A). We retrospectively reviewed 15 patients (29 lesions) diagnosed with gastric MALT lymphoma through upper gastrointestinal endoscopy at our hospital between February 2017 and February 2022. Of these patients, 5 (10 lesions; 3 H. pylori–positive cases (8 lesions) and 2 previously infected cases (2 lesions) were classified as the HP group, and the remaining 10, who were not infected with H. pylori (19 lesions), were classified as the non-HP group. All patients provided written informed consent for endoscopy.
Diagnosis of MALT lymphoma: The lesions of all patients were biopsied at our hospital and diagnosed with MALT lymphoma by hematoxylin-eosin staining and immunostaining.
Diagnosis of H. pylori infection:
H. pylori–positive cases: Two or more of the urea breath test, serum anti-H. pylori antibody test, stool antigen test, rapid urease test, histology, and endoscopic findings were positive.
Previously infected cases: A history of H. pylori infection was previously diagnosed with eradication therapy, and negative results of two or more of the following: urea breath test, serum anti–H. pylori antibody, stool antigen, rapid urease test, tissue microscopy, and endoscopic findings.
H. pylori-uninfected cases: A negative result in two or more of the urea breath test, serum anti-H. pylori antibody, stool antigen, and rapid urease test. In addition, Giemsa staining of gastric biopsy specimens showed no evidence of not only H. pylori but also other Helicobacter spp., no atrophy in endoscopic findings, and no history of eradication.
Evaluation of endoscopic findings: In all patients, Olympus EVIS-ELITE and GIF-H290Z were used as endoscopic systems. Before treatment, two specialists from the Japan Gastroenterological Endoscopy Society evaluated the endoscopic findings. The lesion location and gross type were assessed according to the Japanese Gastric Cancer Treatment Guidelines (15th edition). Fold convergence referred to multiple folds running toward the center of one or more points within the lesion.
In cases where narrow-band imaging (NBI) magnifying endoscopy was performed (HP group (6/10 lesions: 60%), non-HP (10/19 lesions: 53%), VS (vessel plus surface) classification [6], corkscrew pattern [7], and tree-like appearance (TLA) [8] were also evaluated.
Evaluation of clinical findings: As clinical findings, age, sex, opportunity for discovery, clinical stage, treatment method, and average observation period were evaluated using the medical records.
Statistical analysis: All statistical data were analyzed using JMP Pro® 16 (SAS Institute Japan). Continuous and categorical data were analyzed using Mann–Whitney U test and χ2 test, respectively. Furthermore, p<0.05 was considered significant.
Results
Background
Table 1 summarizes the patients’ background. The mean (range) age of patients was 54(25-79) years in the HP group and 57(44-73) years in the non-HP group. Males and females accounted for 2 and 3 in the HP group and 4 and 6 in the nonHP group, respectively. Regarding the opportunity of discovery (screening or presentation of symptoms), 3 of the 5 patients in the HP group and 6 of the 10 patients in the non-HP group were diagnosed through screening. Furthermore, we found single lesions in 3 and 6 patients from the HP and non-HP groups, and multiple (range) lesions in 2(1-5) and 4(1-4) patients, respectively. All results showed no significant differences.
White-light findings (Figures 1a, 1b, 2a, 2b)
Table 2 lists the white-light findings. Lesions were located in the L region in all patients from the HP group (10 lesions), but in the non-HP group, the M region was the most frequent (9 lesions), showing a significant difference (p=0.001). Between the greater curvature, lesser curvature, anterior wall, and posterior wall, the lesser curvature was most the frequent in the HP group (6 lesions), and the greater curvature in the non-HP group (9 lesions), with a significant difference (p=0.010). The median tumor diameter was significantly larger in the non-HP group than in the HP group (median (range): 5(5-20) vs. 10(5-50) mm; p=0.004). In addition, a discoloration was observed in 5 of 10 lesions from the HP group and in 17 out of 19 lesions from the non-HP group; thus, the non-HP group had significantly more lesions with discoloration (p=0.018). The macroscopic type was IIc like: IIc+IIa like in 7 lesions in the HP group and 11 lesions in the non-HP group, with no significant difference. Lastly, the non-HP group had significantly more lesions with fold convergence than the HP group (1(10%) vs. 14(73.7%); p=0.001).
NBI-magnified observation (Figures 1c, 2c)
Table 2 enumerates the findings obtained by NBI-magnified observation. All patients who underwent such a procedure showed no demarcation line, no irregular microsurface or microvascular pattern, and no characteristic corkscrew pattern indicating undifferentiated-type cancer. TLA, which is a characteristic of gastric MALT lymphoma, was observed in 5 out of 6 lesions (83.3%) in the HP group and in 8 out of 10 lesions (80%) in the non-HP group, but the difference was not significant.
Treatment
All cases were classified as Lugano classification stage I. In the HP group, 2 of the 3 H. pylori–positive patients achieved remission with eradication therapy (vonoprazan fumarate 40 mg/ day, amoxicillin hydrate 1500 mg/day and clarithromycin 400 mg/day for 7 days) alone, whereas the remaining 1 achieved remission with additional radiotherapy. Two patients with preinfected H. pylori were in remission with radiotherapy. Initially, in 8 of the 10 patients in the non-HP group, eradication therapy was given, but lesions remained. Nonetheless, after radiotherapy, remission was achieved. Meanwhile, the two remaining patients who did not desire eradication therapy achieved remission with radiotherapy without eradication therapy. In all patients, radiation therapy was performed as an outpatient at 2 Gy for 15 times.
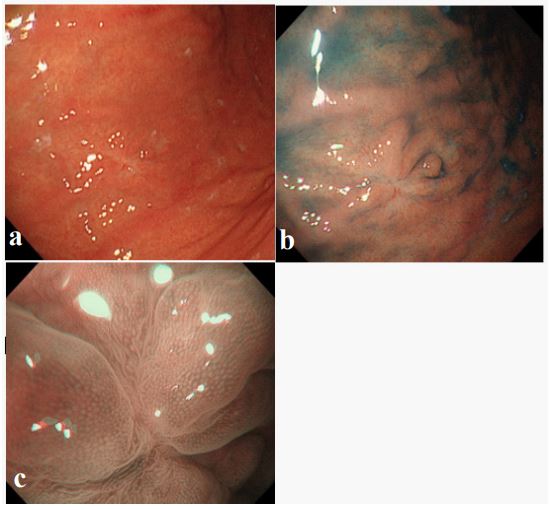
a) White-light view. The lesion was located in the middle of the greater curvature of the body. The gross type was 0-IIc like, and the tumor size was 10 mm.
b) Indigocarmine spraying view. Lesion and fold convergence became clearer.
c) NBI-magnified observation. Discolored lesions (−); tree-like appearance (−); microsurface (MS) pattern, regular; microvascular (MV) pattern, regular; corkscrew pattern (−)
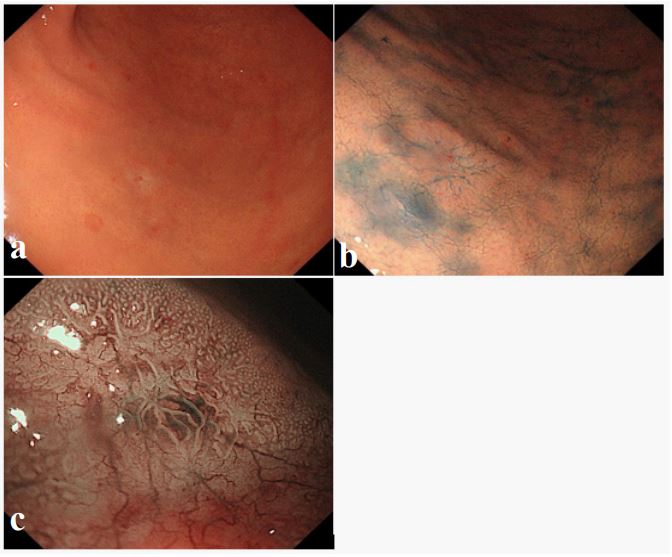
a) White-light view. The lesion was located in the anterior wall of the lower gastric body. The gross type was 0-IIc like, and the tumor size was 10 mm. Fold convergence (−).
b) Indigocarmine spraying view. Recognized as a depressed lesion, but the borders are rather indistinct.
c) NBI-magnified observation. DL (−); TLA (+); MS, absent; MV, regular; corkscrew (−).
Table 1: Characteristics of patients and lesions (n=15).
| HP(n=5) | Non-HP(n=10) | P-value | |
|---|---|---|---|
| Age(mean,(range)),years | 54(25-79) | 57(44-73) | 0.378 |
| Sex (%) | 1 | ||
| Male | 2(40) | 4(40) | |
| Female | 3(60) | 6(60) | |
| Opportunity for discovery (%) | 1 | ||
| Screening | 3(60) | 6(60) | |
| Symptomatic | 2(40) | 4(40) | |
| The number of lesions | 0.558 | ||
| Single | 3(60) | 6(60) | |
| Multiple (range) | 2(40,1-5) | 4(40,1-4) | |
| Clinical stage, Lugano classification stage | 1 | ||
| I | 5(100) | 10(100) | |
| II | 0 | 0 | |
| III | 0 | 0 | |
| IV | 0 | 0 | |
| Treatment method | 0.039 | ||
| H.pylori eradication alone | 2(40) | 0 | |
| H. pylori eradication and radiation |
1(20) | 8(80) | |
| Radiation alone | 2(40) | 2(20) | |
| Observation period, median, months | 24 | 30 | 0.388 |
Table 2: Characteristics of endoscopy Findings.
| White light findings | HP(n=10) | Non-HP(n=19) | P-value |
|---|---|---|---|
| Location of lesion(%) | 0.001 | ||
| U | 0 | 5(26.3) | |
| M | 0 | 9(47.4) | |
| L | 10(100) | 5(26.3) | |
| Location of lesion(%) | 0.01 | ||
| Greater curvature | 1(10) | 9(47.4) | |
| Lesser curvature | 6(60) | 1(5.3) | |
| Anterior | 2(20) | 7(36.8) | |
| Posterior | 1(10) | 2(10.3) | |
| Tumor size (median, range), mm | 5(5-20) | 10(5-50) | 0.004 |
| Color | 0.018 | ||
| Discolored | 5(50) | 17(89.3) | |
| Red | 5(50) | 2(10.3) | |
| Gross type | 0.523 | ||
| II c like | 7(70) | 11(57.9) | |
| II c+ II a like | 3(30) | 8(42.1) | |
| Fold convergence | 0.001 | ||
| (+) | 1(10) | 14(73.3) | |
| (-) | 9(90) | 5(26.3) | |
| NBI findings | HP (n=6) | Non-HP (n=10) | P-value |
| DL(%) | |||
| (+) | 0 | 0 | |
| (-) | 6(100) | 10(100) | |
| IMSP(%) | |||
| (+) | 0 | 0 | |
| (-) | 6(100) | 10(100) | |
| IMVP(%) | |||
| (+) | 0 | 0 | |
| (-) | 6(100) | 10(100) | |
| TLA(%) | 0.869 | ||
| (+) | 5(83.3) | 8(80) | |
| (-) | 1(16.3) | 2(20) | |
| Corkscrew pattern(%) | |||
| (+) | 0 | 0 | |
| (-) | 6(100) | 10(100) |
DL: demarcation line; IMSP: Irregular microsurfacepattern;
IMVP: Irregular microvascular pattern; TLA: Tree like appearance.
Discussion
H. pylori infection has attracted attention as the main cause of gastric MALT lymphoma, but in recent years, the percentage decreased to 30% in Europe and the United States [3]. In this study, only 5 of 15 cases (33%) had gastric MALT lymphoma with current or past H. pylori infection. A decrease in the H. pylori infection rate and the widespread use of eradication therapy suggest an increase in the number of patients with H. pylori–uninfected gastric MALT lymphoma.
In Japan, Sano’s classification (superficial, ulcer, protuberance, ulcer, and giant fold) and Yao’s classification (superficial enlargement, tumor formation, and giant fold) have been used as macroscopic classifications of gastric malignant lymphoma. In gastric MALT lymphoma, the superficial-type is common. However, endoscopic images are very diverse, and in many cases, the morphology seemingly resembles that of early gastric cancer or gastritis, making it one of the difficult diseases to differentiate. Gastric MALT lymphoma lesions in H. pylori–negative patients are similar to those observed in H. pylori–positive participants.
In particular, gastric MALT lymphoma reportedly resembles early gastric cancer [4]. However, reports on the characteristics of endoscopic findings in H. pylori–uninfected gastric MALT lymphoma are still few [4,5]. In this study, white-light was characterized by discolored lesions with fold convergence in the greater curvature of the UM region. In H. pylori–uninfected stomachs, differentiating gastric MALT lymphoma from undifferentiatedtype cancer and gastric adenocarcinoma of the fundic gland type, which also exhibit discolored lesions in white-light findings, is necessary.
TLA is an endoscopic finding of gastric MALT lymphoma via NBI. It is an abnormal blood vessel image that looks like branches branching from the trunk of a tree, seen in shiny mucous membranes with a tendency to lose glandular structures. In particular, TLA is reportedly useful in distinguishing MALT lymphoma from undifferentiated-type cancer presenting with discolored and depressed lesions. A previous study of TLA incidence in H. pylori–positive and -negative cases reported that approximately 75% of cases were recognized as TLA [8]. In the present study, NBI-magnified observation detected TLA in more than 80% of patients regardless of H. pylori infection, indicating a useful finding. In addition, TLA is useful for selecting biopsy sites and assessing therapeutic effects [9]. According to previous reports based on the presence or absence of H. pylori infection, H. pylori–negative cases were more frequent in the upper gastric body (70%), were less surface-type (40%), and were more likely to invade deeper than the submucosa (70%) [5]. Our study is different in that only the superficial-type cases were examined, but it is consistent with the previous study in which cases of H. pylori–uninfected gastric MALT lymphoma are more likely to occur in the upper gastric body.
In our study, lesion discoloration and fold convergence in the greater curvature of the UM region concurrently were characteristics of the non-HP group. Lymphoma is the main site of lesions in the subepithelial region, and the muscularis mucosa is easily destroyed. Perhaps, lymphoma likely develops in the greater curvature of the body without atrophy; thus, fold convergence is likely to occur as the lesion develops. To avoid overlooking such lesions, we need to fully extend the greater curvature of the body and check for any abnormalities in the running of folds.
Endoscopic images of gastric MALT lymphoma are diverse, and making a diagnosis based on endoscopic findings alone is often difficult. First, we need to include MALT lymphoma in the differential diagnosis. However, despite the suspicion, the diagnosis may still hardly be made after multiple biopsies. Approximately 11%-22% of cases on initial endoscopy and 50%-75% of cases on subsequent biopsies were diagnosed with MALT lymphoma [10]. Regardless of H. pylori infection, we need to differentiate MALT lymphoma, confirm the presence or absence of TLA by NBI magnifying endoscopy (if possible), and actively perform biopsy.
In this study, none of the H. pylori–uninfected stomachs showed remission after eradication therapy, but after radiotherapy, all of them achieved remission. In cases without Helicobacter spp. and in cases with unsuccessful eradication therapy, radiation therapy is effective in the early stage [11]. However, given that eradication therapy causes only minor adverse events and the progression of gastric MALT lymphoma is slow, eradication therapy may be tried first [12]. The limitations of this research were as follows. The number of cases is small, given that data were only collected from a single institution. This was a retrospective study and only stage I patients were included; hence, the evaluation of endoscopic findings may be biased. Moreover, MALT lymphoma can relapse after remission for a long time; however, the observation period of this study might be too short to show long-term results. H. pylori–uninfected MALT lymphoma is rare, and prospective studies remain difficult. Thus, we need to accumulate a large number of cases from multiple institutions and examine the endoscopic findings accordingly.
Conclusion
The proportion of patients with gastric MALT lymphoma with H. pylori infection or past infection remained at 33%, whereas that of H. pylori–uninfected gastric MALT lymphoma was increasing. This malignancy was characterized by discolored lesions with fold convergence on the greater curvature of the middle or upper body of the stomach.
TLA was observed in 80% of cases who received NBI-magnified observation, even in H. pylori-uninfected gastric MALT lymphoma. Hence, NBI-magnified observation may be a useful tool for differentiating such a malignancy from early gastric cancer. Given that the H. pylori infection rate is currently decreasing, the opportunities for H. pylori–uninfected gastric endoscopy are increasing. Therefore, we need to understand the characteristics of the endoscopic findings of this H. pylori-uninfected gastric MALT lymphoma.
Declarations
Conflict of interests: The authors declare no conflicts of interest for this article.
Funding sources: None.
Acknowledgment: The authors wish to thank the clinical staff for their participation and contribution to this report.
References
- Isaacson P, Wright DH. Malignant lymphoma of mucosa-associated lymphoid tissue. A distinctive type of B-cell lymphoma. Cancer. 1983; 52: 1410-1416.
- Nakamura S, Sugiyama T, Matsumoto T, Iijima K, Ono S, Tajika M, et al. Long-term clinical outcome of gastric MALT lymphoma after eradication of Helicobacter pylori: a multicentre cohort follow-up study of 420 patients in Japan. Gut. 2012; 61: 507-513.
- Cook JR. Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma). Swerdlow SH In: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon: IARC. 2017; 259-262.
- Asano N, Iijima K, Koike T, Imatani A, Shimosegawa T. Helicobacter pylori-negative gastric mucosa-associated lymphoid tissue lymphomas: a review. World J Gastroenterol. 2015; 21: 8014-8020.
- Nakamura S, Matsumoto T, Ye H, Nakamura S, Suekane H, Matsumoto H, et al. Helicobacter pylori-negative gastric mucosaassociated lymphoid tissue lymphoma: a clinicopathologic and molecular study with reference to antibiotic treatment. Cancer. 2006; 107: 2770-2778.
- Yao K, Takaki Y, Matsui T, Iwashita A, Anagnostopoulos GK, Kaye P, et al. Clinical application of magnification endoscopy and narrow-band imaging in the upper gastrointestinal tract: new imaging techniques for detecting and characterizing gastrointestinal neoplasia. Gastrointest Endosc Clin N Am. 2008; 18: 415-433.
- Nakayoshi T, Tajiri H, Matsuda K, Kaise M, Ikegami M, Sasaki H. Magnifying endoscopy combined with narrow band imaging system for early gastric cancer: correlation of vascular pattern with histopathology (including video). Endoscopy. 2004; 36: 1080-1084.
- Nonaka K, Ishikawa K, Shimizu M, Sakurai T, Nakai Y, Nakao M, et al. Education and imaging. gastrointestinal: gastric mucosaassociated lymphoma presented with unique vascular features on magnified endoscopy combined with narrow-band imaging. J Gastroenterol Hepatol. 2009; 24: 1697.
- Nonaka K, Ohata K, Matsuhashi N, Shimizu M, Arai S, Hiejima Y, et al. Is narrow-band imaging useful for histological evaluation of gastric mucosa-associated lymphoid tissue lymphoma after treatment? Dig Endosc. 2014; 26: 358-364.
- Taal BG, Boot H, van Heerde P, de Jong D, Hart AA, Burgers JM. Primary non-Hodgkin lymphoma of the stomach: endoscopic pattern and prognosis in low versus high grade malignancy in relation to the MALT concept. Gut. 1996; 39: 556-561.
- Schmelz R, Miehlke S, Thiede C, Brueckner S, Dawel M, Kuhn M, et al. Sequential H. pylori eradication and radiation therapy with reduced dose compared to standard dose for gastric MALT lymphoma stages IE & II1E: a prospective randomized trial. J Gastroenterol. 2019; 54: 388-395.
- Zullo A, Hassan C, Ridola L, De Francesco V, Rossi L, Tomao S, et al. Eradication therapy in Helicobacter pylori-negative, gastric low-grade mucosa-associated lymphoid tissue lymphoma patients: a systematic review. J Clin Gastroenterol. 2013; 47: 824-827.