
Journal of Gastroenterology Research and Practice
Research Article - Open Access, Volume 3
Patient survival based on temporal relationships between metastatic pancreatic cancer and brain metastases treated in a single institution: An opportunity for early detection
Susan Haag1*; Derek Cridebring2
1Honor Health, Scottsdale Osborn Medical Center, Scottsdale Arizona, 85251, USA.
2Vice President, Molecular Medicine Division and Clinical Partner Relations, Translational Genomics Research Institute (TGen), Phoenix AZ 85004, USA.
*Corresponding Author : Susan Haag
Honor Health, Scottsdale Osborn Medical Center,
Scottsdale Arizona, 85251, USA.
Email: susan.haag@ymail.com
Received : Oct 03, 2023
Accepted : Nov 01, 2023
Published : Nov 08, 2023
Archived : www.jjgastro.com
Copyright : © Haag S (2023).
Abstract
Introduction: Brain metastasis (BM) is an inauspicious finding in patients with pancreatic cancer (PC) and significantly increases morbidity and mortality. Because the presentation is rare, there is a dearth of information on patient characteristics, treatments, and disease progression. If PC patients who are most likely to develop BM can be detected earlier, there is an opportunity for better prognosis.
Methods: This retrospective, non-interventional study was conducted on PC patients. A subset of the data identifying patients with BM was used as an exploratory cohort. Cox regression analysis determined patient survival based on the temporal relationship between PC and BM treated in a single institution.
Results: 926 patient records were identified with PC, of which 31 (3.3%) had metastasized to the brain. Of the patients with BM, 48% were female, with a median age of 67 years; stage at diagnosis revealed 37% diagnosed at Stage II and Stage III. BM was the first diagnosed metastasis in 13 of the 31 patients, and five of those were with-in 100 days of PC diagnosis. The median overall survival in the BM group was 29 months. Increased survival time with PC was not associated with increased risk of developing BM. BM may develop from PC in initial stages of the primary disease and was not dependent on increased survival time with PC.
Discussion: BM in PC is rare and typically represents a fatal outcome. Yet, recent advances in patient-specific and multimodal treatments could signal better prognosis, making earlier detection critical. To our knowledge, this study with 31 PC patients with BM is the largest to date. From this rare analysis of metastasis patterns and survival in PC patients, the authors recommend routine cerebral imaging for PC patients to detect brain metastases. Future, multicenter studies are planned to investigate the role of patient characteristics in disease progression and earlier detection strategies for enhanced decision making and improved survival.
Keywords: Pancreatic cancer; Brain metastasis; Early detection; Cancer survival; Neurosurgery; Neuro-oncology.
Citation: Haag S, Cridebring D. Patient survival based on temporal relationships between metastatic pancreatic cancer and brain metastases treated in a single institution: An opportunity for early detection. J Gastroenterol Res Pract. 2023; 3(8): 1166.
Introduction
Pancreatic Cancer (PC) is highly metastatic, aggressive, and often found in an advanced stage [1,2]. PC is difficult to diagnose due to its location and the commonality of the symptoms. Further, it shows resistance to tradi-tional and newer therapies making treatment of distant metastatic lesions exceptionally problematic [3]. Metastatic PC is most frequently seen in the liver, lymph nodes, and lung while, in contrast, brain metastases (BM) are more rare [4-7]. A recent article reported 25 cases of BM from pancreatic cancer, which has been the largest study to date [8]. Jordan and colleagues examined 5824 patients with PC and found 25 patients (0.4%) with BM. The study identified a speculative association of germline BRCA1/2 alterations with BM in PC and noted that survival after BM development was poor [8].
Low prevalence may be due to poor survival leading to death before BM develops [8,9]. Others speculate that life expectancy and length of time living with PC may increase the chance of metastasis to the brain. This could arise due to the cancer cells’ ability to exist in latency for prolonged periods of time [10].
The incidence rate of brain metastases from all cancers ranges from 9 to 17% in population-based studies of can-cer patients [11]. This is likely an underestimate of the actual incidence rate, due to a myriad of factors including incomplete data sets and misdiagnosis resulting in patients with brain metastases infrequently undergoing autopsies [11]. Ductal adenocarcinomas tend to extend into adjacent structures such as the duodenum, the portal vein, or superior mesenteric vessels. This could potentially aid in the transport and metastasis of cancer in distant areas of the body, including the brain. Most patients are diagnosed in an advanced stage of cancer and may al-ready have distant metastases growing [12].
Brain metastases in patients with PC significantly increase mortality as the diagnosis of a BM has been associat-ed with a survival period of weeks to months [13]. Because of the rarity of BM from PC, the extant literature lacks an adequate representation of patient characteristics, treatments, and disease progression [14]. Therefore, research is needed to include these factors and to inform strategies for early detection. Based on patientspecific and treatment-related factors, optimal treatment could be tailored specifically for each patient, signaling better prognosis [14]. If we understand the patterns that indicate the occurrence of brain metastases, we can look for treat-ments that not only target the primary tumor but also metastases to the brain [15].
The purpose of this current investigation was to assess survival based on temporal relationships between PC and BM and to determine opportunity for earlier detection for better prognosis. This research has the potential to inform future studies as increased awareness of brain involvement is critical when neurological disorders emerge in patients with PC at earlier stages.
Methods
We performed a retrospective, non-interventional study using de-identified data, which included data from the electronic medical record (EMR) system and laboratory information management systems. A BM subset of the data from adult patients treated within a single site with PC was identified as an exploratory cohort. For this study, the eligible participants were adults who had been diagnosed with metastatic pancreatic cancer since 2005. Demographic and clinical data, such as age at pancreatic cancer diagnosis, location of primary pancreas tumor, and stage at diagnosis were collected. Data were extracted, refined, and analyzed to a set of 926 patients. The aim was to study patient survival based on the temporal relationships between pancreatic cancer and brain metastases treated in a single institution. The hypothesis was, PC patients with BM can be detected earlier.
Statistical analysis
This retrospective study had institutional review board approval (IRB# 1453699-1). We employed descriptive statistics, an analysis of data that helped describe, show or summarize data in a meaningful way such that, for example, patterns might emerge from the data. Frequencies and percentages are reported for categorical variables. Medians or means with standard deviations are reported for continuous variables, as appropriate.
Overall survival was calculated from the date of diagnosis to either date of last follow-up or death. Cox regression was used for time-to-event analyses. We used a Cox regression on overall survival time with an indicator variable for patients who ultimately got a brain metastasis. The model was also adjusted for age at diagnosis. This is a departure from the usual use of the regression, where one is trying to explain differences in survival time using factors known at the beginning of the study time period. If brain metastases were associated with extended survival time, the BM indicator variable would suggest a lower hazard ratio.
Results
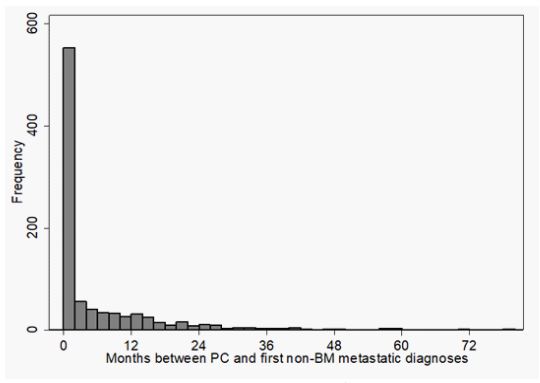
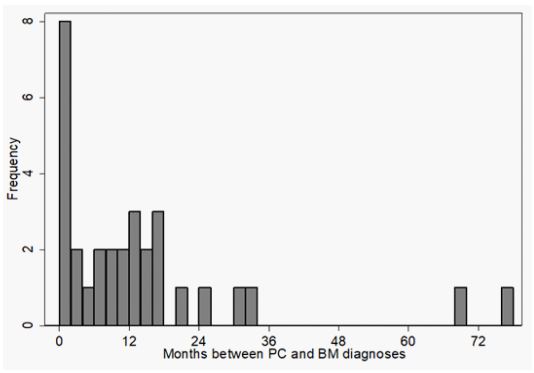
From a total of 926 patients with PC, 31(3.3%) had brain metastases BM, 65% of patients had liver metastases, and 17% had lung metastases. Of the patients with PC, 20% were non-white, 47% female, and the median age was 67. The site of the primary tumor within the pancreas was acquired from ICD10 codes: 35% located in the head of the pancreas, 15% in the body, 14% in the tail, and 36% were in overlapping sites and unspecified loca-tions. Stage at diagnosis included: 76% Stage IV, 6% Stage III, 15% Stage II, and 3% Stage I computed tomography or magnetic resonance imaging was used to detect BM. Of the patients with BM, 21% were non-white, 48% were female, with a median age at PC diagnosis of 67 years (range 31 to 84 years). Site of the primary tumor: 33% were located in the head of the pancreas, 15% in the body, 13% in the tail, and 39% in overlapping sites and unspecified locations. Stage at diagnosis included: 14% Stage II, 23% Stage III, and 63% Stage IV. The median time to the development of brain metastases from initial diagnosis of PC was 304 days. Figure 2 shows the 31 patients and number of months between PC and BM diagnosis. The median overall sur-vival in this group of 31 patients with a brain metastasis was 29 months.
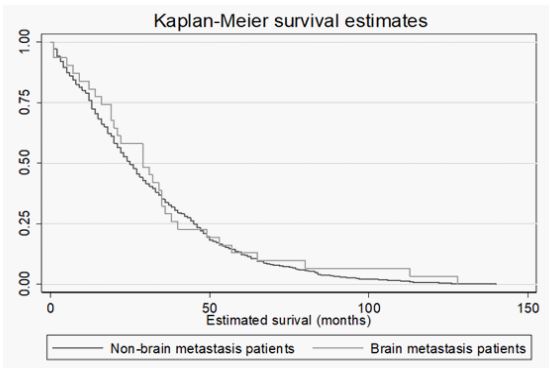
Regression analysis showed no relationship between extended PC survival time and brain metastasis development. BM was the first diagnosed metastasis in 13 of the 31 patients, and five of those were within 100 days of pancreatic cancer diagnosis. The brain metastasis patients revealed the following hazard ratio (HR=0.91, p=0.60). There was no evidence of association between age at diagnosis of the BM and age at PC diagnosis, grouping patients by whether the brain metastasis was the first metastasis or a subsequent one. BM may develop from PC in initial stages of the primary disease and was not dependent on increased survival time with PC (Figure 3).
Discussion
Metastasis, the spread of cancer cells in blood and lymphatic vessels enabling them to colonize in distant organs, has been a clinical challenge [16]. Although BM are rare in general, they are especially rare for gastrointestinal cancers [14]. This is also true for PC as our study, yielding 31 patients with lesions in the brain is, to our knowledge, the largest study to date.
Discerning patterns in the information gathered from patients with PC and BM revealed insightful similarities between them. Pancreatic cancer is diagnosed most commonly among people ranging from 65 to 74 years of age [1]. Similarly, patients we analyzed with PC had a median diagnosis age of 67. Pancreatic cancer is more common in men than women and our PC sample was consistent with national data as we had 53% male and 47% female. The age and sex of the patients in the BM group were also consistent with national data. For both the total sample set and the sample of patients with BM, the most common location for the primary tumor was in the head of the pancreas.
Metastasis continues to be one of the greatest challenges in cancer therapy, is a leading cause of cancer mortality, and thus, earlier detection is critical for improved treatment [17]. This current study showed the median overall survival of 31 BM patients was 29 months and revealed that a BM was the first diagnosed metastasis in 13 of the 31 patients (42%); five of those were within 100 days of pancreatic cancer diagnosis. An opportunity for early detection emerged in this study, and with earlier detection, patient-specific and treatment-related factors could signal better prognosis. Serres and colleagues [17] showed BMs were detectable in vivo using VCAM-1 targeted MRI 5 d after induction, noting clinics could use early detection methods and increase therapeutic options to be optimally effective; earlier detection will go beyond a hypothesis when diagnostic methods are the standard, opening a new window of opportunity for treatments and survival [17].
Diverse variables, such as the number and size of brain lesions, status of primary disease, tumor histology, and general condition of the patient at time of BM diagnosis are important factors in disease management [14]. If we understand the patterns and processes that indicate the occurrence of BM, we can pursue earlier detection and treatments that not only target the primary tumor but also metastases to the brain [15]. Future studies are war-ranted to highlight multimodal therapy and survival to suggest a more personalized decision-making process [14].
There are several limitations to the study. First, there is a chance the metastases are related to a primary cancer other than the pancreatic one, since we don’t have pathology information from the BM. It is also important to recognize that data were not collected for the intention of epidemiological analysis. Challenges included miss-ing data points and lack of information on outcomes after the end of clinical care.
Conclusion
To our knowledge, this is the largest reported study to date comprising 31 patients with BM of pancreatic origin. Future studies that include patient-specific and treatment-related factors could signal better prognosis. Larger, multicenter studies are planned to investigate the role of patient characteristics in disease progression and earlier detection strategies for enhanced decision making and improved survival.
Acknowledgements: We acknowledge the Helios Scholar Internship Program, within the Translational Genomics Research Institute (TGen).
References
- Siegel, RL, Miller, KD., Fuchs, H. E., and Jemal, A. CA: A Cancer Journal for Clinicians. 2021; 71(1): 7-33.
- Neoptolemos JP, Kleef J, Michl P. Costello E. Therapeutic developments in pancreatic cancer: Current and future perspectives. Nat Rev Gastroenterol Hepatol. 2018; 15: 333-345-348.
- Mucciolo G, Roux C, Scagliotti A, Brugiapaglia S, Novelli F, Cappello P. The dark side of immunotherapy pancreatic cancer. Cancer Drug Resist 2020; 3: 491-520. Doi: 10.20517/cdr.2020.13.
- Johnson WR, Theeler BJ, Van Echo D, Young P, Kwok M. Treatment of Leptomeningeal Carcinomatosis in a Patient with Metastatic Pancreatic Cancer: A Case Report and Review of the Literature. Case Rep Oncol. 2018; 11(2): 281-288. doi: 10.1159/000489085. PMID: 29867436; PMCID: PMC5981627.
- Kang Y, Pantel K. Tumor cell dissemination: emerging biological insights from animal models and cancer pa-tients. Cancer Cell. 2013; 23(5): 573-81. doi: 10.1016/j.ccr.2013.04.017. PMID: 23680145; PMCID: PMC3667710.
- Oweira H, Petrausch U, Helbling D, Schmidt J, Mannhart M, Mehrabi A, Schöb O, Giryes A, Decker M, Ab-del-Rahman O. Prognostic value of site-specific metastases in pancreatic adenocarcinoma: A Surveillance Epi-demiology and End Results database analysis. World J Gastroenterol. 2017; 23(10): 1872-1880. doi: 10.3748/wjg.v23.i10.1872. PMID: 28348494; PMCID: PMC5352929.
- Sasaki T, Sato T, Nakai Y, Sasahira N, Isayama H, Koike K. Brain metastasis in pancreatic cancer: Two case re-ports. Medicine (Baltimore). 2019; 98(4): 14227. doi: 10.1097/MD.0000000000014227. PMID: 30681602; PMCID: PMC6358345.
- Jordan EJ, Lowery MA, Basturk O, Allen PJ, Yu KH, Tabar V, Beal K, Reidy DL, Yamada Y, Janjigian Y, Abou-Alfa GK, O’Reilly EM. Brain Metastases in Pancreatic Ductal Adenocarcinoma: Assessment of Molecular Genotype-Phenotype Features-An Entity With an Increasing Incidence? Clin Colorectal Cancer. 2018; 17(2): 315-e321. doi: 10.1016/j.clcc.2018.01.009. Epub 2018 Feb 7. PMID: 29496399; PMCID: PMC6759921.
- Perni S, Wang TJ, Lesser J, Mandigo C, Isaacson SR, Horowitz DP. Gamma Knife treatment of recurrent CNS metastases of pancreatic origin: a case report and review of the literature. CNS Oncol. 2017; 6(2): 111-118. doi: 10.2217/cns-2016-0026. PMID: 28530445; PMCID: PMC6020876.
- Hoshide R, Jandial R. The role of the neural niche in brain metastasis. Clin Exp Metastasis. 2017; 34(6-7): 369-376. doi: 10.1007/s10585-017-9857-7. Epub 2017 Sep 13. PMID: 28905151.
- Yogendran LV, Kalelioglu T, Donahue JH, Ahmad H, Phillips KA, Calautti NM, Lopes MB, Asthagiri AR, Purow B, Schiff D, Patel SH, Fadul CE. The landscape of brain tumor mimics in neuro-oncology practice. J Neu-rooncol. 2022; 159(3): 499-508. doi: 10.1007/s11060-022-04087-4. Epub 2022 Jul 20. PMID: 35857249.
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014; 74(11): 2913-21. doi: 10.1158/0008-5472.CAN-14-0155. Erratum in: Cancer Res. 2014 Jul 15;74(14):4006. PMID: 24840647.
- Sperduto PW, Mesko S, Li J, Cagney et al. Survival in Patients with Bran Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Defntion of the Eligibility Quotient. J Clinical Oncol. 2020: 38(32): 3773-3784.
- De Stafano FA, Morell A, Marks K, et al. Brain Metastasis from Pancreatic Cancer: Our Experience and Sys-tematic Review. World Neurosurg. 2022; 166: 590-598. Doi:10.1016/j.wneu.2022.07.060. Epub 2022 Jul 19. PMID: 35863644.
- Dong J, Wu L, Wang F, Huang J, Hu P, Zhang B, Xia LP, The choice of local treatment modalities Patients with Brain Metastases from Digestive Cancers. J Oncology. 2019; 20191568465. PMID: 31871456;PMCID PMC6907058.
- Jones D. Parallels of Resistance between Angiogenesis and Lymphangiogenesis Inhibition in Cancer Therapy. Cells. 2020; 9(3): 762. doi: 10.3390/cells9030762. PMID: 32244922; PMCID: PMC7140636.
- Serres S, Soto MS, Hamilton A, McAteer MA, Carbonell WS, Robson MD, Ansorge O, Khrapitchev A, Bristow C, Balathasan L, Weissensteiner T, Anthony DC, Choudhury RP, Muschel RJ, Sibson NR. Molecular MRI enables early and sensitive detection of brain metastases. Proc Natl Acad Sci U S A. 2012; 109(17): 6674-9. doi: 10.1073/pnas.1117412109. Epub 2012 Mar 26. PMID: 22451897; PMCID: PMC3340084.https://doi.org/10.1073/pnas.1117412109.