
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 3
Four horsemen of the apocalypse: Human immunodeficiency virus infection, cytomegalovirus colitis, kaposi’s sarcoma and ulcerative colitis in one patient
Bayar Esra1*; Şekuri Hüseyin A2; Ergün Meltem1
1Department of Gastroenterology, Faculty of Medicine, Yeditepe University, Istanbul, Turkey.
2Department of Internal Medicine, Faculty of Medicine, Yeditepe University, Istanbul, Turkey.
*Corresponding Author : Esra Bayar
Department of Gastroenterology, Faculty of Medicine,
Yeditepe University, Içerenköy, Hastane Street No:4
D:4/1, 34752 Ataşehir/Istanbul, Turkey.
Tel: +90-505-937-66 11;
Email: ilessa_esra@hotmail.com
Received : Aug 22, 2023
Accepted : Sep 29, 2023
Published : Oct 06, 2023
Archived : www.jjgastro.com
Copyright : © Bayar E (2023).
Abstract
Kaposi’s Sarcoma (KS) is still one of the most common tumor in Human Immunodeficiency Virus (HIV)-infected patients worldwide. KS is a rare, vascular malignancy of endothelial cells caused by Human Herpesvirus-8 (HHV-8). It can be seen less frequently in Ulcerative Colitis (UC) patients receiving immunosuppressive therapy. We present a 36-year-old homosexual male patient who was admitted to the hospital with prolonged bloody diarrhea and was diagnosed with UC and HIV infection. Antiretroviral treatment and high-dose steroid therapy were prescribed for these diseases; but his symptoms worsened, and further investigations revealed Cytomegalovirus (CMV) colitis and KS due to HHV-8. Therefore, KS and CMV colitis should always be kept in mind if an HIV case with intractable UC symptoms is encountered.
Keywords: Antiretroviral therapy; Colonoscopy; Diarrhea; Immunsuppression; Steroids.
Citation: Esra B, Hüseyin AS, Meltem E. Four horsemen of the apocalypse: Human immunodeficiency virus infection, cytomegalovirus colitis, kaposi’s sarcoma and ulcerative colitis in one patient. J Gastroenterol Res Pract. 2023; 3(8): 1162.
Introduction
Kaposi’s Sarcoma (KS) is one of the most frequent malignancies in Human Immunodeficiency Virus (HIV)-infected patients. KS can start anywhere on the skin, or it can occur on gastrointestinal, genital and ocular mucous membranes. The course of the disease is highly variable; there may be small lesions that can remain stable for years; or there may be aggressive and rapidly spreading lesions and that may even lead to the death of the patient [1].
Inflammatory Bowel Diseases (IBD) may also rarely occur in HIV-positive patients, and the symptoms may be confused with KS. Immunosuppressive therapies used in Ulcerative Colitis (UC) may exacerbate HIV-associated KS, and endoscopic findings may be similar in both diseases. Therefore, endoscopic biopsies taken from HIV-positive patients should also include submucosal tissue and Herpesvirus-8 (HHV-8) should be carefull investigated histopathologically. IBD, Cytomegalovirus (CMV) colitis, and KS should be included in the differential diagnosis in HIV-positive patients; especially in patients with delayed diagnosis of HIV infection or in patients who do not comply with their treatment as this may affect the treatment and survival of the patients. In one study, antiretroviral therapy combined with liposomal doxorubicin in patients with HIV-associated KS has shown a high 5-year survival rate (85%) [2]. In HIV-positive immunosuppressed patients, more than one disease may present in the same localization, and the symptoms may overlap with each other.
Case presentation
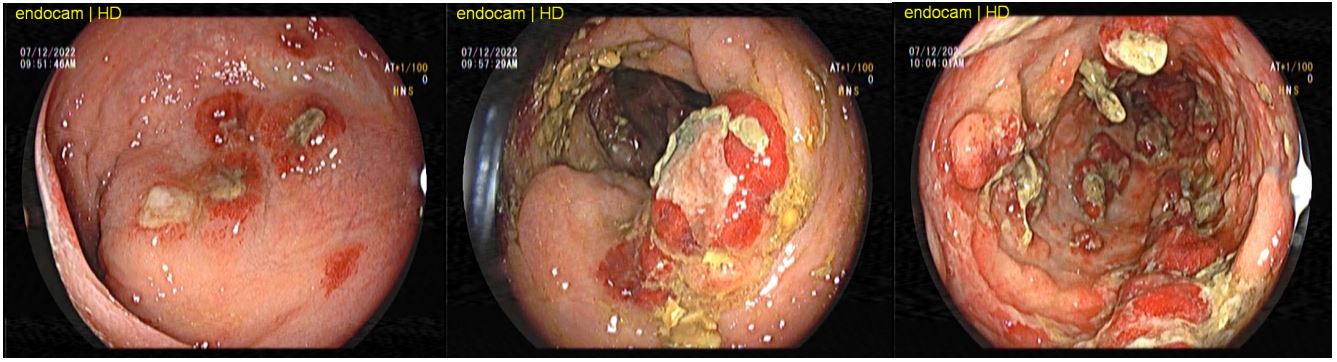
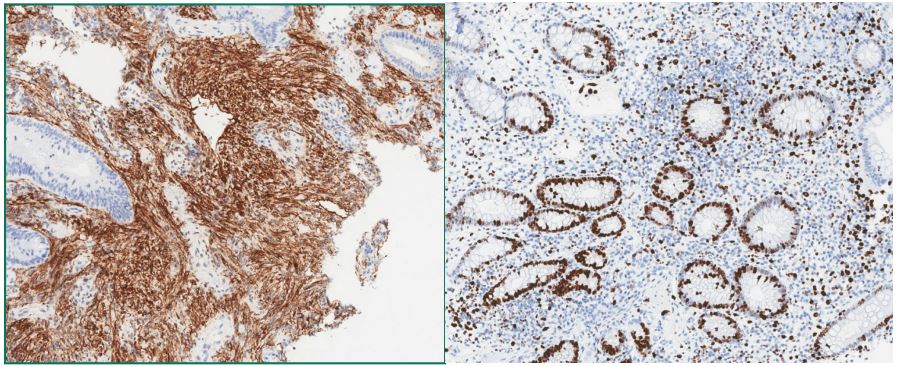
A 36-year-old male patient presented to our outpatient clinic in September 2022 with weakness, fatigue, bloody diarrhea, abdominal pain and weight loss. In June 2022, the patient was evaluated at another hospital with similar complaints, was diagnosed with UC by colonoscopic examination; and methylprednisolone was started. But his complaints did not regress and he lost approximately 10 kg, and HIV infection was diagnosed in July 2022. CD4 T lymphocyte count was detected 29%; biktegravir/emtricitabine/tenofovir alafenamide was initiated. He only mentioned that he was homosexual. Physical examination revealed abdominal tenderness. The patient complained of bloody and mucous stools more than 10 times a day and weight loss continued. Fecal calprotectin was 993 ug/g (0-50 ug/g); Cryptosporidia, Giardia and Entamoeba antigens were negative; Salmonella spp., Shigella spp., Plesiomonas spp. and Aeromonas spp. were negative. Clostridium difficile toxin A-B were negative. Stool analysis showed leukocytes and erythrocytes. In laboratory tests; leucocytes: 4620/µL, lymphocyte: 1220/ µL, hemoglobin: 9.5 g/dL, C-Reactive Protein (CRP): 53.9 mg/L were detected. The patient was started on methylprednisolone 1 mg/kg and mesalazine granule 3 g and mesalazine enema 1x4 g. Two weeks later, the patient’s number of bloody and mucous stools decreased and his abdominal pain regressed; but since a proximal myopathy developed, the dose of methylprednisolone was reduced and Azathioprine (AZA) 1 x 50 mg was added to treatment. The patient admitted a few weeks later and stated that he did not take his medication regularly, so the number of stools increased again and he continued to lose weight. In a new colonoscopic examination, active colitis was observed throughout all colon segments; and multiple and ulcerated mass-like reddish nodules which merged with each other and small pseudopolyps were observed on the mucosa (Figure 1). Histopathologically, the lesions consisted of spindle cells and irregularly distributed vascular proliferations was found; active chronic colitis was also determined in the surrounding mucosa of the lesions. On immunohistochemistry, the lesional cells were positive for CD34 and HHV-8. And with these findings, the diagnosis of KS was confirmed (Figure 2).
In addition, serum CMV DNA load: 2461 IU/mL, tissue CMV DNA from the colon mucosa was determined 31,779,821 IU/ mL; AZA was discontinued; low dose methylprednisolone and mesalazine were continued. Valganciclovir treatment was started for CMV colitis. In December 2022, the patient was consulted to the medical oncology clinic due to KS. The patient was evaluated for sarcoma metastasis with Positron Emission Tomography/Computed Tomography (PET/CT); and no metastasis was observed, there was diffuse sarcoma infiltration throughout the colonic mucosa. In multidisciplinary oncology meeting; liposomal doxorubicin treatment was planned for the patient. Although it was emphasized that it was important to comply the treatment, the patient left the follow-up.
Discussion
KS is a rare, slowly progressive vascular malignancy, originating from lymphatic endothelial cells. The presence of primary intestinal KS without cutaneous involvement is quite uncommon, so recognizing KS can be challenging. Nearly all subtypes of KS are associated with HHV-8 infection [3].
Several case reports have demonstrated the relationship between KS and UC; and all of these cases presented with similar symptoms [4,5]. KS usually involves the submucosa of the intestines, then progresses deeper, involving all intestinal layers. If the lesion is not a prominent reddish nodule or plaque as in KS, or if the lesions are obscured by IBD such as UC; the diagnosis may not be confirmed histopathologically. Therefore, to make definitive diagnosis, the biopsy should be taken deeply to include the submucosa [6].
In the first colonoscopy of our patient, endoscopic findings were more suggestive of UC. The biopsies probably only involved the mucosa and the diagnosis of KS could not be made histopathologically, or sarcoma lesions were hidden in the severe inflammation of UC. But, the lesions of KS became obvious endoscopically and microscopically as a result of immunosuppression by methylprednisolone for UC.
The host immune response is critical in controlling CMV infections. The most severe manifestations of a CMV infection are observed in immunocompromised patients; CMV colitis is also associated with acute, severe UC exacerbations, requiring treatment with high-dose corticosteroids [7]. Corticosteroids are a predisposing factor for CMV reactivation, suppressing anti-CMV T-cell function and directly activating viral replication [8,9]. High dose steroids and other immunomodulators such as thiopurines are associated with CMV colitis in patients with active UC [10]. In our case with bloody diarrhea, CMV colitis and KS were diagnosed at the same time, but the patient's clinical findings initially appeared as an UC exacerbation. His immunosuppression progressed due to both HIV infection and high-dose steroids and thiopurines therapies. This progressive immunosuppression caused an increased susceptibility to CMV and HHV-8 infections, leading to simultaneous detection of KS and CMV colitis. Because of that, the differential diagnosis should be extended in homosexual individuals presenting with prolonged bloody diarrhea.
According to the guidelines of the European Crohn’s and Colitis Organization (ECCO) in 2014, the management of CMV infection in UC patients is as follows: “In patients with severe steroid-resistant colitis with CMV detected in the colon mucosa under immunomodulator therapy, antiviral therapy should be started and immunomodulators should be discontinued until colitis symptoms improve” [7]. As a result of deterioration of clinical findings in our case, oral steroid treatment was reduced, and AZA was discontinued; valganciclovir for CMV colitis and antiretroviral treatments for HIV were started as mentioned in the ECCO guideline. In addition, liposomal doxycycline, which has a very high effectivity on KS, was recommended, unfortunately our patient was lost to follow-up.
Conclusion
In UC patients, KS may present only gastrointestinal tract involvement. Therefore, HIV positive patients with persistent UC symptoms, KS should be included in the differential diagnosis. It should be kept in mind that due to immunosuppression, CMV colitis can also be seen together with these diseases and rapid modifications in treatment can be life-saving.
Conflict of interest: The authors have no conflict of interest to declare.
References
- C Hoffmann, M Sabranski, S Esser. HIV- associated Kaposi’s Sarcoma. Oncol res treat. 2017; 40: 94-98.
- Bower M, Dalla Pria A, Coyle C, Andrews E, Tittle V, et al. Prospective stage-stratified approach to AIDS-related Kaposi’s sarcoma. J Clin Oncol. 2014; 32: 409-414.
- S Esser, H Schöfer, C Hoffmann, J Claßen, A Kreuter, et al. S1 guidelines for Kaposi Sarcoma. J Dtsch Dermatol Ges. 2022; 20: 892-904.
- Adlersberg R. Kaposi’s sarcoma complicating ulcerative colitis: report of a case. Am J Clin Pathol. 1970; 54: 143-146.
- Cetin B, Büyükberber S, Yılmaz IB, Yıldız R, Coşkun U, et al. Kaposi’s sarcoma in patients with ulcerative colitis receiving immunosuppressive drugs: Report of a case. Turk J Gastroenterol. 2011; 22: 621-625.
- Biggs BA, Crowe SM, Lucas CR, Ralston M, Thompson IL, et al. AIDS related Kaposi’s sarcoma presenting as ulcerative colitis and complicated by toxic megacolon. Gut. 1987; 28: 1302-1306.
- Sylvie Pillet, Bruno Pozzetto, Xavier Roblin. Cytomegalovirus and ulcerative colitis: Place of antiviral therapy. World J Gastroenterol. 2016; 22: 2030-2045.
- Van Damme E, Sauviller S, Lau B, Kesteleyn B, Griffiths P, et al. Glucocorticosteroids trigger reactivation of human cytomegalovirus from latently infected myeloid cells and increase the risk for HCMV infection in D+R+ liver transplant patients. J Gen Virol. 2015; 96: 131-143.
- Inoue-Toyoda M, Kato K, Nagata K, Yoshikawa H. Glucocorticoids facilitate the transcription from the human cytomegalovirus major immediate early promoter in glucocorticoid receptor- and nuclear factor-I-like protein-dependent manner. Biochem Biophys Res Commun. 2015; 458: 180-185.
- Shukla T, Singh S, Tandon P, McCurdy JD. Corticosteroids and Thiopurines, But Not Tumor Necrosis Factor Antagonists, are Associated with Cytomegalovirus Reactivation in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. J Clin Gastroenterol. 2017; 51: 394-401.