
Journal of Gastroenterology Research and Practice
Review Article - Open Access, Volume 3
Non-invasive biomarkers in chronic inflammatory bowel disease: State of the art
Sawsan Feki1*; Lassaad Chtourou2; Ameni Jerbi1; Dorra Bouzid1; Hend Hachicha1; Nabil Tahri2; Hatem Masmoudi1
1Laboratory of Immunology, Habib Bourguiba UH, Sfax, Tunisia.
2Gastroenterology Department, Hedi Chaker UH, Sfax, Tunisia.
*Corresponding Author : Sawsan Feki
Laboratory of Immunology, Habib Bourguiba Hospital,
University of Sfax, 3029, Sfax, Tunisia.
Tel: +216-58-127-972 & +216-92-796-659;
Email: sawsanfeki@yahoo.fr
Received : Aug 28, 2023
Accepted : Sep 26, 2023
Published : Oct 03, 2023
Archived : www.jjgastro.com
Copyright : © Feki S (2023).
Abstract
The need to improve the diagnosis and classification of chronic Inflammatory Bowel Disease (IBD) on the one hand, the monitoring and prognostic prediction on the other hand, have prompted scientific efforts to improve the characterization of the already-known markers and to search for other potential effective parameters. Consequently, the predominant target of polynuclear neutrophil Anti-Cytoplasma (ANCA) in ulcerative colitis (DNA-bound lactoferrin) and exocrine anti-pancreatic antibodies (Ab) in Crohn’s Disease (CD)) (GP2 and CUZD1) have recently been identified. Moreover, new markers have shown their potential clinical utility during IBD. Most of them have been associated with CD, such as anti-glycans which include in addition to classic ASCA, other recently described markers (Anti-Laminaribioside (ALCA), Anti-Chitobioside (ACCA), antimannobioside (AMCA), anti-laminarin (anti-L) and anti-chitin (anti-C)). Other anti-microbial antigens Ab (anti-OmpC, anti-Cbir1 and anti-I2 sequence Ab) have been also reported and associated with certain clinical phenotypes of CD. Regarding inflammatory markers, serum C-reactive protein, calprotectin and faecal lactoferrin, which are considered to be simple and very well studied markers, have shown their reliability in the differentiation between IBD and irritable bowel syndrome, the classification of the degree of intestinal inflammation and the follow-up under treatment. Finally, non-coding RNAs, the more recently described biomarkers, seem to be detectable in blood and useful in enhancing diagnosis, classification and monitoring disease activity.
Keywords: Crohn's disease; Ulcerative colitis; Biomarkers; Serum, Stool; Intestinal inflammation.
Citation: Feki S, Chtourou L, Jerbi A, Bouzid D, Hachicha H, et al. Non-invasive biomarkers in chronic inflammatory bowel disease: State of the art. J Gastroenterol Res Pract. 2023; 3(7): 1161.
Introduction
Chronic Inflammatory Bowel Disease (IBD) is considered as a heterogeneous group of chronic inflammatory conditions affecting the gastrointestinal tract [1]. Their diagnosis is conventionally based on a set of clinical, radiological, endoscopic and histological arguments. Currently, biomarkers could be useful as helpful clinical tools for diagnosis and for prediction of disease course and therapeutic response [2-5]. The reliability of a biomarker depends on its effectiveness in differentiating IBD from other non-IBD diseases, having a similar clinical presentation and in discriminating between Crohn’s Disease (CD) and Ulcerative Colitis (UC), the 2 main forms of IBD. The biomarker usefulness also depends on its prognostic prediction and its role in monitoring disease activity, including under treatment [6].
Among the various known serological markers, only antineutrophil cytoplasmic antibodies (Ab) (ANCA) and anti-Saccharomyces cerevisiae Ab (ASCA) have demonstrated diagnostic utility. Their simultaneous research improves the specificity in the distinction between MC and UC. However, the interest of ASCA and ANCA is limited, in particular because of their moderate sensitivities. Moreover, these auto-Abs are not predictive of disease activity, and are of no interest in monitoring treatment [1,4,6-8]. More recently, non-coding RNAs (ncRNAs) have attracted a lot of interest in the context of IBD. Preliminary data reported emerging roles of some of these markers in the diagnosis, treatment and prognosis of IBD and its associated-colorectal cancer. The need to improve the diagnostic and classification tools, on the one hand, and the monitoring and prognostic prediction (activity, course, response to treatment) of IBD on the other hand, has led efforts to better characterize the already-known markers and to look for new promising parameters [5,6,9].
Classic IBD markers
Currently, the conventionnel markers for IBD diagnosis in routine practice remains ASCA and ANCA. Other previouslydescribed markers are less frequently associated with IBD: they are mainly exocrine anti-pancreatic antibodies (APE) (in CD); but also anti-goblet cells of the intestine (ACCI) (in UC) which is less described and studied.
ANCA (Anti-Neutrophil Cytoplasmic Antibodies)
During IBD, ANCA seem to target a nuclear and non-cytoplasmic component of PNNs. In this context, these Ab are called atypical p-ANCAs of the “Nuclear Associated Neutrophil Antibodies” (NANA) or x-ANCA type. They are specific markers of UC with a specificity greater than 88% [1]. Thus, serum levels of ANCA could be a helpful tool for the diagnosis of UC [10]. Furthermore, monitoring of ANCA-IgG levels could predict disease course and may guide treatment of UC [11]. In particular, in patients with severe UC, pANCA may be useful in determining the clinical response to infliximab [12].
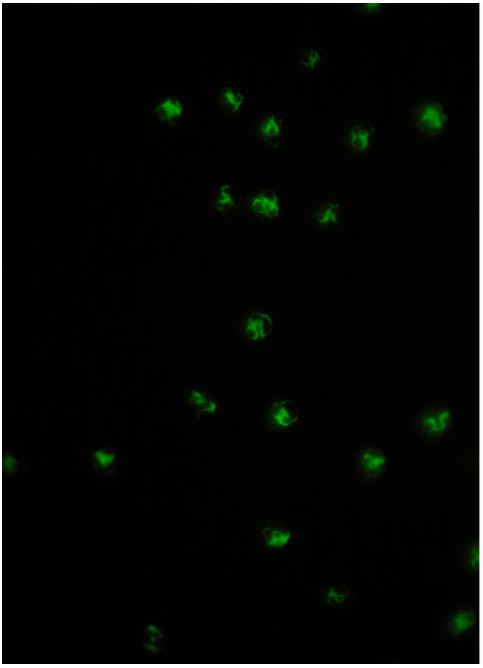
The screening for NANA (IgG) is carried out first by Indirect Immunofluorescence (IIF) on human PNNs fixed with ethanol and then by IIF on human PNNs fixed with formalin and methanol. The initial p-ANCA pattern, lost on the formalin slide, could be found on the methanol slide. Moreover, this p-ANCA aspect is atypical compared to ANCA directed against myeloperoxidase (MPO-ANCA), with a thinner and less regular border surrounding the nucleus of PNNs (Figure 1) [1].
For a long period of time, the exact antigenic target of NANA has remained unknown. Several studies proposing nuclear components of PNNs as potential or possible targets for these autoAbs have been ruled out. Lactoferrin has been suggested as a target of NANA during UC. However, the detection of this molecule was impossible using Western Blot or monospecific ELISA (purified lactoferrin bound to the solid phase) techniques. Recently, some authors have shown that it is exactly the lactoferrin bound to DNA, detected by IIF performed on granulocytes treated with saline solution and reconstituted with human lactoferrin “LFR granulocytes”, which is the major target of NANA during of UC (72% of cases) [13].
A pathophysiological role has been suggested for these DNAbound anti-lactoferrin Ab. They seem to be able to bind to components of chromatin and to PNN proteins, involved in the composition of extracellular traps “Neutrophil Extracellular Traps” (NETs). Granulocytes, in general, and NETs in particular, are considered as cornerstones of the innate defense against microbes (GRAM positive and negative bacteria), especially in barriers such as the intestinal mucosa. Therefore, the auto-Abs directed against the components of nets could affect this antimicrobial defense at this barrier, which suggests the link between microbial infection and the onset of autoimmunity during IBD [13].
ASCA (anti-Saccharomyces cerevisiae Ab)
Described in the late 1980s, these Ab react with brewer’s and bread yeast, Saccharomyces cerevisiae. Since then, they have been known as a specific marker for CD within adults as well as children with a specificity above 90%. In clinical practice, serum ASCA levels was found to be the most accurate serological marker for the differential diagnosis of CD [14]. In addition, combined tests of serum ANCA-IgG, ASCA-IgG, and ASCA-IgA levels may help to distinguish UC from CD [11,15].
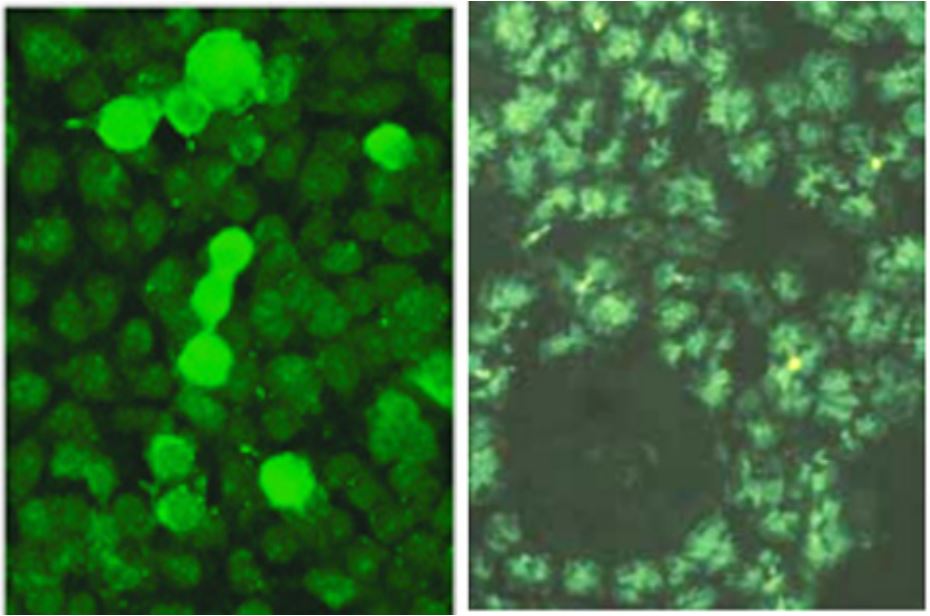
The antigenic target recognized by these Abs is found in the soluble extract of the yeast wall. This is phosphopeptidomannan, commonly referred to as “Mannan” (GP of 200 kDa). The antigenic determinants are more precisely trimannoside epitopes. ASCA are detected by IIF on a culture of S. cerevisiae, with a fluorescent pattern of the wall of yeasts (Figure 2).
Besides, ASCA can be detected by Elisa or by immunodot. These two techniques use antigens extracted from boiled or disrupted yeast or phosphopeptidomannans purified from the wall of yeasts [1]. Recently, “gASCA”, an improved ASCA test, has been described, which is based on the covalent immobilization of purified “mannan” polysaccharides, and has proved to be efficient in comparison with the conventional ASCA test [16].
On the other hand, recent researches have revealed promising new markers of the anti-glycans family, to which ASCA belongs. Most of these recent parameters are associated with CD (see below “Abs directed against microbial antigens”) [6].
Anti- Exocrine Pancreas antibodies (AEP)
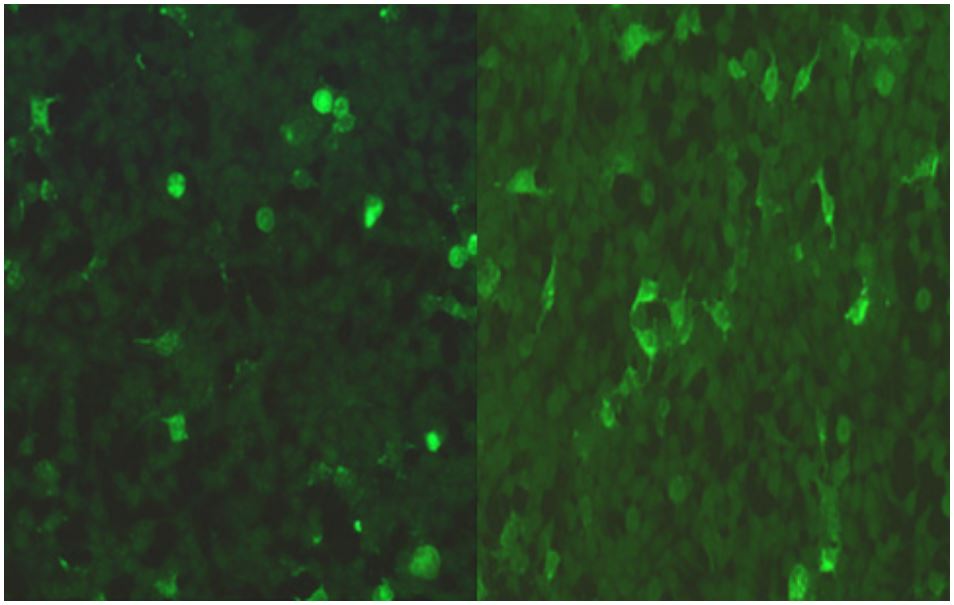
Described for the first time in 1987 in patients with CD, AEP (IgG) are detected by IIF on sections of primate or human pancreas. Two types of fluorescence patterns can be distinguished: the first is an extracellular pattern in drops located in the lumen of the pancreatic acinis, while the 2nd is an intracellular reticulogranular pattern detected within the acinis (Figure 3).
It has been shown that AEP have an excellent positive predictive value for IBD (99%). Their excellent specificity for CD was re-discussed after the study conducted by Joossens et al., where authors showed a prevalence of 32% of AEP in CD but also a positivity of 23% in UC and 22% in healthy relatives of patients [1]. Recently, molecular targets for APEs have been identified [17-19]:
* Fluorescence pattern in drops in the lumen of acini is related to the major target of APE during IBD: “the zymogen granule glycoprotein 2 (GP2)”.This target is also present on the surface of the “Microfold” M cells of Peyer’s patches and appears to play an immunomodulatory role in the intestine.
* The intracellular reticulo-granular fluorescence pattern within acinis is mainly due to Ab directed against the target “CUB and zona pellucida-like domains containing protein 1 (CUZD1)”. GP2 and CUZD1 belong to the family of innate immunity proteins. It seems that these two molecules are involved in maintaining the balance between tolerance to commensal bacteria and defense against pathogens in the intestine [17].
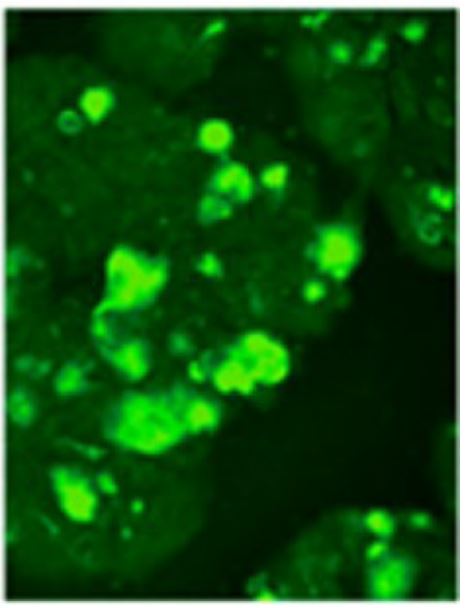
The characterization of these targets is carried out by IIF on transfected HEK 293 cells (Figure 4) or by ELISA.
The anti-GP2 and anti-CUZD1 Ab have been described mainly during CD (Table 1). Most studies focused on determining the clinical relevance of anti-GP2. Serum level of this Ab is more detected in patients with CD than in UC [6]. The detection of anti-GP2, in combination or not with ASCA, allows a phenotypic classification of CD patients. In fact, anti-GP2 can be used to evaluate the clinical severity, especially with early onset, pouchitis and pouch surgery [20].
Studies related to Anti-CUZD1 remain very limited. However, IgA isotype of this marker appears to be associated with complications in CD.
Anti- Caliciform Cells of the Intestine (ACCI)
More than 50 years ago, these Ab were described as pathognomonic markers of UC but with a low prevalence of 28%. They are detected by IIF. The substrate of choice is fetal primate intestinal tissue. The presence of these Ab is responsible for an indistinct borderline “woolly” fluorescence (Figure 5).

Markers directed against microbial antigens
The spectrum of antibodies directed against different microbial antigens which are described as associated with IBD continues to expand rapidly. Most of these Abs are associated with CD, such as the family of anti-glycans, which in addition to the classic ASCA, include other recently described markers: anti-laminaribioside Ab (ALCA), anti-chitobioside (ACCA), antimannobioside (AMCA), anti-laminarin (anti-L) and anti-chitin (anti-C) (Table 1). Despite of the lack of sensitivity of these biomarkers for the diagnosis of IBD, they are capable of identifying a small group of patients with CD seronegative for the conventional markers (such as ASCA). AMCAs, ALCAs and ACCAs can be used for the differentiation between CD and UC [17]. The specificity of anti-L and anti-C for CD diagnosis is relatively high with a low sensitivity. Therefore, the combination of these Abs with ANCA and ASCA detection may be more helpful in the differentiation of CD from UC [18-22]. Moreover, the new anti-glycans seem to be correlated with the complicated forms of CD and are associated with a severe course and the need for surgical treatment [6].
Other anti-microbial antigens Ab have been reported during IBD: anti-OmpC "anti-Escherichia coli Outer membrane porin C", anti-Cbir1 flagellin and Ab "anti-I2 Pseudomonas fluorescens sequence" were particularly associated with certain clinical phenotypes of CD (stenosing and penetrating forms) [6,23]. More recently, Ab against 2 other flagellins (A4-Fla2, Fla-X) have been identified and appear to be associated with complications [24,25]. However, given their low sensitivity, the role of these Abs in the diagnosis and prognostic evaluation during IBD remains a controversial issue.
Table 1: Characteristics and prevalence of the new serological markers (anti-exocrine pancreas and anti-microbial antigen antibodies) of inflammatory bowel disease [6,20,24,25].
| Biomarker | Antigenic target | Isotype | Technique of detection |
Prevalence (%) | Ref | |||
|---|---|---|---|---|---|---|---|---|
| CD | UC | Other GI disorders | Unaffected controls |
|||||
| Anti-pancreas exocrin | ||||||||
| anti-GP2 |
Pancreatic major glycoprotein GP2 of the zymogen granule membrane |
IgA | IIF ELISA | 1-25 | 0-13 | 4 29-38 celiac disease |
0-4 | 26-33 |
| anti-GP2 | IgG | IIF ELISA | 10-44 | 1-22 | 0–1 0-19 celiac disease |
0-8 | 26-34. | |
| anti-GP2 | IgA and/or IgG |
IIF ELISA |
21-45 | 2-19 | 4 | 1-8 | 26-30, 32, 33. | |
| anti-CUZD1 |
CUB and zona pellucida-like domains containing protein 1 |
IgA | IIF | 12.1- 16.1 |
2.9-6.2 | --------- | 0 | 15, 35-37. |
| anti-CUZD1 | IgA | IIF | 16.3- 17.9 |
4.4-6.7 | --------- | 0 | ||
| anti-CUZD1 | IgA and/or IgG |
IIF | 21-26 | 5.9-9 | --------- | 0 | ||
| Antibodies anti-microbial antigen | ||||||||
| gASCA | Purified carbohydrate PPM epitopes from S. cerevisiae wall | IgA and/or IgG |
ELISA | 0-69 | 0-14 | 1-23 11-22 celiac disease |
0-15 | 21, 22, 38-45. |
| ACCA | Chitobioside (GlcNAc (β1, 4) GlcNAc (β)) | IgA | ELISA | 8-52 | 0-45 | 3-35 22 celiac disease |
2-33 | 21, 22, 38-40, 42-46. |
| ALCA | Laminaribioside (Glc (β1, 3) Glc (β)) | IgA | ELISA | 8–76 | 0-22 | 1-21 0-7 celiac disease |
0-23 | 21, 22, 38-47. |
| AMCA | Mannobioside (Man (α, 3) Manα | IgA | ELISA | 12-67 | 0-36 | 3-27 | 0-33 | 22, 38-40, 42-46. |
| Anti-C | Chitin (GlcNAc (β1, 4)) n | IgA | ELISA | 10-25 | 2-15 | 7-23 | 2 | 22, 39, 42. |
| Ani-L | Laminarin (Glc (β1, 3)) 3n (Glc (β1, 6)) n) | IgA | ELISA | 11-26 | 3-15 | 4-11 | 2 | 22, 39, 42. |
| ≥1 anti-glycan | 59-78 | 28-48 | 21-50 | 21-23 | 22, 24, 39, 40, 42. | |||
| Anti-OmpC | Escherichia coli outer mem-outer mem- brane porin C | IgA | ELISA | 24-55 | 2-24 | 5-11 | 5-20 | 37,48-62. |
| Anti-I2 | I2 Pseudomonas fluorescens sequence | IgA | ELISA | 38-60 | 2-10 | 19 | 5–15 | 48-51, 54, 55, 60, 63, 64. |
| Anti-Cbir1 | Cbir1 bacteria flagellin | IgA | ELISA | 50-56 | 6-36 | 14 | 8 | 50, 53, 55, 57, 65, 66. |
CD: Crohn’s disease; UC: ulcerative colitis; GI: gastro-intestinal, IIF : Indirect Immunofluorescence; ELISA: Enzyme-Linked Immunosorbent Assay.
Benefits of inflammation markers during IBD
Subjective assessment of disease activity during IBD is often described as unreliable. The objective criteria for measuring inflammation correlate much more with long-term outcome, but depend generally on invasive and expensive procedures such as ileocoloscopy and imaging. Non-invasive, accurate and inexpensive indicators of intestinal inflammation would allow the clinician to better adjust therapies and thus, to improve the control of inflammation [2,7]. Several non-invasive inflammatory markers were tested in blood, stool and other biological fluids (urine). While no marker has been universally adopted, some have been well characterized, and others appear to be very promising.
Serum C-reactive protein "C Reactive Protein (CRP)" and fecal calprotectin (cytosolic protein of neutrophils binding zinc and calcium, easily detected in the stool) are among the best studied, simple and non-invasive biomarkers of inflammation in IBD [2,7,8], their reliability has been described in the differentiation between IBD and irritable bowel syndrome, in the classification of the degree of intestinal inflammation, in the evaluation of the response to treatment, and eventually, in the detection of recurrent inflammation after remission.
Thus, CRP and fecal calprotectin are currently useful in clinical practice for the management of IBD patients [10,67] In addition to these two markers, the detection of lactoferrin in the stool (thermostable protein derived from PNNs that have migrated into the intestinal mucosa), appears to be a promising indicator for monitoring intestinal inflammation [68].
Non-coding RNAs in IBD
NcRNAs, including microRNA (miRNA), long ncRNA (lncRNA) and circular RNAs (circRNAs), have gained a lot of interest last years. Although they account for ~90% of RNAs, these molecules have no protein coding potential and are important regulatory mediators transcribed from the genome. They control gene expression at the RNA level [8,69]. NcRNAs abnormal expression in blood or tissues has been associated with several autoimmune and malignant disorders [8]. Regarding IBD, it seems that the expression level of circulating and tissue ncRNA is different in patients compared to healthy controls. In particular, miRNAs, a short and stable ncRNAs (18-24 nucleotides) involved in the negative regulation of gene expression at the post-transcriptional level by binding the 3′- untranslated region of mRNA (inhibition of translation or degradation of mRNA), seems to be a promising non-invasive biomarker of disease activity in blood [5,8]. Several studies showed that miRNAs may be involved in the mediation of inflammatory responses, intestinal barrier dysfunction and gut microbiota interactions [5,8,70,71]. Most of the recent research in IBD has measured levels of circulating miRNAs in body fluids such as blood or feces, and in homogenized tissue biopsies using techniques like microarray profiling, RT-qPCR, and NGS [72]. Serum concentrations of some miRNAs (such as miR-16, miR-21, and miR-223) are reported to be higher in IBD patients than in healthy controls and levels may differ between CD and UC patients. MiRNAs have been therefore identified as promising diagnostic biomarkers (to differentiate IBD from other non-IBD diseases and UC from CD) and potential therapeutic targets [2,4,5,73,74]. It could potentially be used for disease management in IBD.
Furthermore, LncRNAs, a non-coding RNAs involved in the regulation of various intracellular processes and have a length of more than 200 nucleotides, is also reported to be a potential relatively stable and simply detectable biomarker for IBD diagnosis [75]. LncRNAs have been proven to play important role in IBD pathogenesis, including regulation of the intestinal epithelial barrier, cell apoptosis, and various immune system processes [8]. Preliminary studies have shown that LncRNAs’ expression may be different between IBD patients and healthy controls as well as between CD and UC patients [8,76]. The profile of this biomarker in blood needs to be more investigated, to identify new lncRNAs, and to assess their diagnostic value as a non-invasive biomarker in IBD.
Regarding CircRNAs which are considered as microRNA sponges regulating gene expression at the transcriptional or post-transcriptional level, the alteration of their expression in IBD results in intestinal epithelial barrier and immune homeostasis dysregulation [69,77]. Available reports suggest that CircRNAs (ex: circRNA_004662) might be a novel candidate for differentiating CD from UC as well as a promising prognosis marker [69]. On the other hand, circRNA_103516 level in PBMCs was found to be a potential biomarker for diagnosing IBD [78]. Additionally, it seems that some circRNAs may serve as a promising target for the disease therapy [8].
Oncostatin M
Oncostatin M (OSM) is a member of IL-6 cytokine family. A high and consistent expression of this marker in affected mucosa and in blood has been reported in IBD patients [4,8,79]. Serum level is particularly elevated in active IBD patients as well as in unaffected first-degree relatives of IBD patients [8,79]. It has been reported that serum level of OSM could be a diagnostic biomarker of IBD [4,8,79]. However, it seems that this circulating level could not predict the disease outcome and treatment responsiveness, in contrary with colonic OSM level [80].
Conclusion
So far, no national, European or international recommendation exists concerning the routine detection of Ab (including ANCA and ASCA) for the diagnosis and prognostic prediction of IBD. However, several recent studies have suggested the potential clinical utility of some new markers in IBD, which can be detected in serum, (anti-GP2, new anti-glycans...) as well as in the stool (fecal calprotectin and lactoferrin) at different times in the natural history of the disease. Due to the variation in the results from one study to another (sample size, inclusion criteria, techniques and methodology used, etc.), more prospective data are required to better evaluate the behavior of these markers in relation to the disease course, in particular during the treatment. Non-coding RNAs offer a promising window of opportunity to identify potential non invasive diagnostic blood markers and treatment targets for IBD and its associated-colorectal cancer.
References
- Benkhadra F, Humbel RL. Les marqueurs sérologiques des maladies inflammatoires chroniques intestinales (MICI). Immunoanalyse et biologie spécialisée. 2008; 23, 202-211.
- Alghoul Z, Yang C, Merlin D. The Current Status of Molecular Biomarkers for Inflammatory Bowel Disease. Biomedicines. 2022; 10: 1492.
- Salla M, Guo J, Joshi H, Gordon M, Dooky H, et al. Novel Biomarkers for Inflammatory Bowel Disease and Colorectal Cancer: An Interplay between Metabolic Dysregulation and Excessive Inflammation. Int J Mol Sci. 2023; 24: 5967.
- Sakurai T, Saruta M. Positioning and Usefulness of Biomarkers in Inflammatory Bowel Disease. Digestion. 2023; 104: 30-41.
- Liu D, Saikam V, Skrada KA, Merlin D, Iyer SS. Inflammatory bowel disease biomarkers. Med Res Rev. 2022; 42: 1856-1887.
- Bonneau J, Dumestre-Perard C, Rinaudo-Gaujous M, Genin C, Sparrow M, et al. Systematic review: New serological markers (anti-glycan, anti-GP2, anti-GM-CSF Ab) in the prediction of IBD patient outcomes. Autoimmun Rev. 2015; 14: 231-45.
- Roblin X, Cavaille A, Clavel L, Paul S. Intérêt des biomarqueurs dans la prise en charge des MICI.; Presse Med. 2014; 43: 66-73.
- Chen P, Zhou G, Lin J, Li L, Zeng Z, et al. Serum Biomarkers for Inflammatory Bowel Disease. Front Med (Lausanne). 2020; 7: 123.
- Sands BE. Biomarkers of Inflammation in Inflammatory Bowel Disease. Gastroenterology. 2015; 149: 1275-1285.e2.
- Høie O, Aamodt G, Vermeire S, Bernklev T, Odes S, et al. Serological markers are associated with disease course in ulcerative colitis. A study in an unselected population-based cohort followed for 10 years. Journal of Crohn’s and Colitis. 2008; 2: 114-22.
- Pang Y, Ruan H, Wu D, Lang Y, Sun K, et al. Assessment of clinical activity and severity using serum ANCA and ASCA antibodies in patients with ulcerative colitis. Allergy Asthma Clin Immunol. 2020; 16: 37.
- Nguyen DL, Nguyen ET, Bechtold ML. pANCA positivity predicts lower clinical response to infliximab therapy among patients with IBD. South Med J. 2015; 108: 139-43.
- Teegen B, Niemann S, Probst C, Schlumberger W, Stöcker W, et al. DNA-bound lactoferrin is the major target for antineutrophil perinuclear cytoplasmic antibodies in ulcerative colitis. Contemporary Challenges in Autoimmunity: Ann N Y Acad Sci. 2009; 1173: 161-5.
- Gao X, Zhang Y. Serological markers facilitate the diagnosis of Crohn’s disease. Postgrad Med. 2021; 133: 286-290.
- Reese GE, Constantinides VA, Simillis C, Darzi AW, Orchard TR, et al. Diagnostic precision of anti-Saccharomyces cerevisiae antibodies and perinuclear antineutrophil cytoplasmic antibodies in inflammatory bowel disease. Am J Gastroenterol. 2006; 101: 2410-22.
- Papp M, Altorjay I, Dotan N, Palatka K, Foldi I, et al. New serological markers for inflammatory bowel disease are associated with earlier age at onset, complicated disease behavior, risk for surgery, and NOD2/CARD15 genotype in a Hungarian IBD cohort. Am J Gastroenterol. 2008; 103: 665-81.
- Pavlidis P, Komorowski L, Teegen B, Liaskos C, Koutsoumpas AL, et al. Diagnostic and clinical significance of Crohn’s disease-specific pancreatic anti-GP2 and anti-CUZD1 antibodies. Clin Chem Lab Med. 2016; 54: 249-56.
- Papp M, Sipeki N, Tornai T, Altorjay I, Norman GL, et al. Rediscovery of the Anti-Pancreatic Antibodies and Evaluation of their Prognostic Value in a Prospective Clinical Cohort of Crohn’s Patients: The Importance of Specific Target Antigens [GP2 and CUZD1]. J Crohns Colitis. 2015; 9: 659-68.
- Michaels MA, Jendrek ST, Korf T, Nitzsche T, Teegen B, et al. Pancreatic Autoantibodies Against CUZD1 and GP2 Are Associated with Distinct Clinical Phenotypes of Crohn’s Disease. Inflamm Bowel Dis. 2015; 21: 2864-72.
- Werner L, Sturm A, Roggenbuck D, Yahav L, Zion T, et al. Antibodies against glycoprotein 2 are novel markers of intestinal inflammation in patients with an ileal pouch. J Crohns Colitis. 2013; 7: e522-32.
- Dotan I, Fishman S, Dgani Y, Schwartz M, Karban A, et al. Antibodies against laminaribioside and chitobioside are novel serologic markers in Crohn’s disease. Gastroenterology. 2006; 131: 366-78.
- Rieder F, Schleder S, Wolf A, Dirmeier A, Strauch U, et al. Association of the novel serologic anti-glycan antibodies anti-laminarin and anti-chitin with complicated Crohn’s disease behavior. Inflamm Bowel Dis. 2010; 16: 263-74.
- Kohoutova D, Drahosova M, Moravkova P, Rejchrt S, Bures J. Anti-Outer membrane protein C and anti-glycoprotein 2 antibodies in inflammatory bowel disease and their association with complicated forms of Crohn’s disease. BMC Gastroenterol. 2014; 14: 190.
- Kuna AT. Serological markers of inflammatory bowel disease. Biochem Med (Zagreb). 2013; 23: 28-42.
- Liaskos C, Rigopoulou EI, Orfanidou T, Bogdanos DP, Papandreou CN. CUZD1 and anti-CUZD1 antibodies as markers of cancer and inflammatory bowel diseases. Clin Dev Immunol. 2013; 2013: 968041.
- Roggenbuck D, Hausdorf G, Martinez-Gamboa L, Reinhold D, Büttner T, et al. Identification of GP2, the major zymogen granule membrane glycoprotein, as the autoantigen of pancreatic antibodies in Crohn’s disease. Gut. 2009; 58: 1620-8.
- Roggenbuck D, Reinhold D, Wex T, Goihl A, von Arnim U, et al. Autoantibodies to GP2, the major zymogen granule membrane glycoprotein, are new markers in Crohn’s disease. Clin Chim Acta. 2011; 412: 718-24.
- Op De Beéck K, Vermeire S, Rutgeerts P, Bossuyt X. Antibodies to GP2, the major zymogen granule membrane glycoprotein, in inflammatory bowel diseases. Gut. 2012; 61: 162-4.
- Bogdanos DP, Roggenbuck D, Reinhold D, Wex T, Pavlidis P, et al. Pancreatic-specific autoantibodies to glycoprotein 2 mirror disease location and behaviour in younger patients with Crohn’s disease. BMC Gastroenterol. 2012; 12: 102.
- Pavlidis P, Forbes A, Bogdanos DP. Antibodies to glycoprotein 2 (GP2) in patients with inflammatory bowel diseases from UK. Clin Chim Acta. 2011; 412: 1163-4.
- Gross S, Bakker SF, van Bodegraven AA, van Hoogstraten IM, Gelderman KA, et al. Increased IgA glycoprotein-2 specific antibody titres in refractory celiac disease. J Gastrointestin Liver Dis. 2014; 23: 127-33.
- Bonaci-Nikolic B, Spuran M, Andrejevic S, Nikolic M. Autoantibodies to GP2, the major zymogen granule membrane glycoprotein, in patients with gluten-sensitive enteropathy: a possible serological trap. Clin Chim Acta. 2012; 413: 822-3.
- Roggenbuck D, Bogdanos D, Conrad K. Loss of tolerance to one or two major targets in Crohn’s disease or just cross-reactivity?, J Crohns Colitis. 2013; 7: e273-4.
- Pavlidis P, Romanidou O, Roggenbuck D, Mytilinaiou MG, Al-Sulttan F, et al. Ileal inflammation may trigger the development of GP2-specific pancreatic autoantibodies in patients with Crohn’s disease. Clin Dev Immunol. 2012; 2012: 640835.
- Desir B, Amre DK, Lu SE, Ohman-Strickland P, Dubinsky M, et al. Utility of serum antibodies in determining clinical course in pediatric Crohn’s disease. Clin Gastroenterol Hepatol. 2004; 2: 139-46.
- Esters N, Vermeire S, Joossens S, Noman M, Louis E, et al. Belgian Group of Infliximab Expanded Access Program in Crohn’s Disease. Serological markers for prediction of response to antitumor necrosis factor treatment in Crohn’s disease. Am J Gastroenterol. 2002; 97: 1458-62.
- Cohavy O, Bruckner D, Gordon LK, Misra R, Wei B, et al. Colonic bacteria express an ulcerative colitis pANCA-related protein epitope. Infect Immun. 2000; 68: 1542-8.
- Prideaux L, Kamm MA, De Cruz P, van Langenberg DR, Ng SC, et al. Inflammatory bowel disease serology in Asia and the West. World J Gastroenterol. 2013; 19: 6207-13.
- Rieder F, Hahn P, Finsterhoelzl L, Schleder S, Wolf A, et al. Clinical utility of anti-glycan antibodies in pediatric Crohn’s disease in comparison with an adult cohort. Inflamm Bowel Dis. 2012; 18: 1221-31.
- Koutroubakis IE, Drygiannakis D, Tsirogianni A, Oustamanolakis P, Karmiris K, et al. Antiglycan antibodies in Greek patients with inflammatory bowel disease. Dig Dis Sci. 2010; 56: 845-52.
- Simondi D, Mengozzi G, Betteto S, Bonardi R, Ghignone RP, et al. Antiglycan antibodies as serological markers in the differential diagnosis of inflammatory bowel disease. Inflamm Bowel Dis. 2008; 14: 645-51.
- Seow CH, Stempak JM, Xu W, Lan H, Griffiths AM, et al. Novel anti-glycan antibodies related to inflammatory bowel disease diagnosis and phenotype. Am J Gastroenterol. 2009; 104: 1426-34.
- Malickova K, Lakatos PL, Bortlik M, Komarek V, Janatkova I, et al. Anticarbohydrate antibodies as markers of inflammatory bowel disease in a Central European cohort. Eur J Gastroenterol Hepatol. 2010; 22: 144-50.
- Henckaerts L, Pierik M, Joossens M, Ferrante M, Rutgeerts P, et al. Mutations in pattern recognition receptor genes modulate seroreactivity to microbial antigens in patients with inflammatory bowel disease. Gut. 2007; 56: 1536-42.
- Lakatos PL, Altorjay I, Mándi Y, Lakatos L, Tumpek J, et al. Hungarian IBD Study Group, Papp M. Interaction between seroreactivity to microbial antigens and genetics in Crohn’s disease: Is there a role for defensins? Tissue Antigens. 2008; 71: 552-9.
- Michielan A, Basso D, Martinato M, Pathak S, Banerjee A, et al. Increased antibody response to microbial antigens in patients with Crohn’s disease and their unaffected first-degree relatives.Dig Liver Dis. 2013; 45: 894-8.
- Rejchrt S, Drahosová M, Kopácová M, Cyrany J, Douda T, et al. Antilaminaribioside and antichitobioside antibodies in inflammatory bowel disease. Folia Microbiol (Praha). 2008; 53: 373-6.
- Mow WS, Vasiliauskas EA, Lin YC, Fleshner PR, Papadakis KA, et al. Association of antibody responses to microbial antigens and complications of small bowel Crohn’s disease. Gastroenterology. 2004; 126: 414-24.
- Spivak J, Landers CJ, Vasiliauskas EA, Abreu MT, Dubinsky MC, et al. Antibodies to I2 predict clinical response to fecal diversion in Crohn’s disease. Inflamm Bowel Dis. 2006; 12: 1122-30.
- Dubinsky MC, Lin YC, Dutridge D, Picornell Y, Landers CJ, et al. Western Regional Pediatric IBD Research Alliance. Serum immune responses predict rapid disease progression among children with Crohn’s disease: immune responses predict disease progression. Am J Gastroenterol. 2006; 101: 360-7.
- Landers CJ, Cohavy O, Misra R, Yang H, Lin YC, et al. Selected loss of tolerance evidenced by Crohn’s disease-associated immune responses to auto- and microbial antigens. Gastroenterology. 2002; 123: 689-99.
- Zholudev A, Zurakowski D, Young W, Leichtner A, Bousvaros A. Serologic testing with ANCA, ASCA, and anti-OmpC in children and young adults with Crohn’s disease and ulcerative colitis: Diagnostic value and correlation with disease phenotype. Am J Gastroenterol. 2004; 99: 2235-41.
- Dubinsky MC, Kugathasan S, Mei L, Picornell Y, Nebel J, et al. Western Regional Pediatric IBD Research Alliance; Pediatric IBD Collaborative Research Group; Wisconsin Pediatric IBD Alliance. Increased immune reactivity predicts aggressive complicating Crohn’s disease in children. Clin Gastroenterol Hepatol. 2008; 6: 1105-11.
- Arnott IDR, Landers CJ, Nimmo EJ, Drummond HE, Smith BKR, et al. Seroreactivity to microbial components in Crohn’s disease is associated with disease severity and progression, but not NOD2/CARD15 genotype. Am J Gastroenterol. 2004; 99: 2376-84.
- Devlin SM, Yang H, Ippoliti A, Taylor KD, Landers CJ, et al. NOD2 variants and antibody response to microbial antigens in Crohn’s disease patients and their unaffected relatives. Gastroenterology. 2007; 132: 576-86.
- Elkadri AA, Stempak JM, Walters TD, Lal S, Griffiths AM, et al. Serum antibodies associated with complex inflammatory bowel disease. Inflamm Bowel Dis. 2013; 19: 1499-505.
- Markowitz J, Kugathasan S, Dubinsky M, Mei L, Crandall W, et al. Age of diagnosis influences serologic responses in children with Crohn’s disease: a possible clue to etiology? Inflamm Bowel Dis. 2009; 15: 714-9.
- Mei L, Targan SR, Landers CJ, Dutridge D, Ippoliti A, et al. Familial expression of anti-Escherichia coli outer membrane porin C in relatives of patients with Crohn’s disease. Gastroenterology. 2006; 130: 1078-85.
- O’Donnell S, O’Sullivan M, O’Morain CA, Ryan BM. The clinical significance of antimicrobial serologic responses within an Irish Crohn’s disease population. Eur J Gastroenterol Hepatol. 2013; 25: 1464-9.
- Papadakis KA, Yang H, Ippoliti A, Mei L, Elson CO, et al. Antiflagellin (CBir1) phenotypic and genetic Crohn’s disease associations. Inflamm Bowel Dis. 2007; 13: 524-30.
- Davis MK, Andres JM, Jolley CD, Novak DA, Haafiz AB, et al. Antibodies to Escherichia coli outer membrane porin C in the absence of anti-Saccharomyces cerevisiae antiboies and antineutrophil cytoplasmic antibodies are an unreliable marker of Crohn disease and ulcerative colitis. J Pediatr Gastroenterol Nutr. 2007; 45: 409-13.
- Coukos JA, Howard LA, Weinberg JM, Becker JM, Stucchi AF, et al. ASCA IgG and CBir antibodies are associated with the development of Crohn’s disease and fistulae following ileal pouchanal anastomosis. Dig Dis Sci. 2012; 57: 1544-53.
- Sutton CL, Kim J, Yamane A, Dalwadi H, Wei B, et al. Identification of a novel bacterial sequence associated with Crohn’s disease. Gastroenterology. 2000; 119: 23-31.
- Iltanen S, Tervo L, Halttunen T, Wei B, Braun J, et al. Elevated serum anti-I2 and anti-OmpW antibody levels in children with IBD. Inflamm Bowel Dis. 2006; 12: 389-94.
- Lodes MJ, Cong Y, Elson CO, Mohamath R, Landers CJ, et al. Bacterial flagellin is a dominant antigen in Crohn disease. J Clin Invest. 2004; 113: 1296-306.
- Targan SR, Landers CJ, Yang H, Lodes MJ, Cong Y, et al. Antibodies to CBir1 flagellin define a unique response that is associated independently with complicated Crohn’s disease. Gastroenterology. 2005; 128: 2020-8.
- Sipponen T, Kolho KL. Fecal calprotectin in diagnosis and clinical assessment of inflammatory bowel disease. Scand J Gastroenterol. 2015; 50: 74-80.
- Mosli MH, Zou G, Garg SK, Feagan SG, MacDonald JK, et al. CReactive Protein, Fecal Calprotectin, and Stool Lactoferrin for Detection of Endoscopic Activity in Symptomatic Inflammatory Bowel Disease Patients: A Systematic Review and Meta-Analysis. Am J Gastroenterol. 2015; 110: 802-19.
- Xu Y, Xu X, Ocansey DKW, Cao H, Qiu W, et al. CircRNAs as promising biomarkers of inflammatory bowel disease and its associated-colorectal cancer. Am J Transl Res. 2021; 13: 1580-1593.
- Williams MR, Stedtfeld RD, Tiedje JM, Hashsham SA. MicroRNAs-Based Inter-Domain Communication between the Host and Members of the Gut Microbiome. Front Microbiol. 2017; 8: 1896.
- Nguyen HT, Dalmasso G, Müller S, Carrière J, Seibold F, et al. Crohn’s disease-associated adherent invasive Escherichia coli modulate levels of microRNAs in intestinal epithelial cells to reduce autophagy. Gastroenterology. 2014; 146: 508-19.
- James JP, Riis LB, Malham M, Høgdall E, Langholz E, et al. MicroRNA Biomarkers in IBD-Differential Diagnosis and Prediction of Colitis-Associated Cancer. Int J Mol Sci. 2020; 21: 7893.
- Feng Y, Zhang Y, Zhou D, Chen G, Li N. MicroRNAs, intestinal inflammatory and tumor. Bioorg Med Chem Lett. 2019; 29: 2051-2058.
- Quaglio AEV, Santaella FJ, Rodrigues MAM, Sassaki LY, Di Stasi LC. MicroRNAs expression influence in ulcerative colitis and Crohn’s disease: A pilot study for the identification of diagnostic biomarkers. World J Gastroenterol. 2021; 27: 7801-7812.
- Zacharopoulou E, Gazouli M, Tzouvala M, Vezakis A, Karamanolis G. The contribution of long non-coding RNAs in Inflammatory Bowel Diseases. Dig Liver Dis. 2017; 49: 1067-1072.
- Chen D, Liu J, Zhao HY, Chen YP, Xiang Z, et al. Plasma long noncoding RNA expression profile identified by microarray in patients with Crohn’s disease. World J Gastroenterol. 2016; 22: 4716-31.
- Kristensen LS, Andersen MS, Stagsted LVW, Ebbesen KK, Hansen TB, et al. The biogenesis, biology and characterization of circular RNAs. Nat Rev Genet. 2019; 20: 675-691.
- Ye YL, Yin J, Hu T, Zhang LP, Wu LY, et al. Increased circulating circular RNA_103516 is a novel biomarker for inflammatory bowel disease in adult patients. World J Gastroenterol. 2019; 25: 6273-6288.
- Verstockt S, Verstockt B, Vermeire S. Oncostatin M as a new diagnostic, prognostic and therapeutic target in inflammatory bowel disease (IBD). Expert Opin Ther Targets. 2019; 23: 943-954.
- West NR, Hegazy AN, Owens BMJ, Bullers SJ, Linggi B, et al. Oxford IBD Cohort Investigators, Keshav S, Travis SPL, Powrie F. Oncostatin M drives intestinal inflammation and predicts response to tumor necrosis factor-neutralizing therapy in patients with inflammatory bowel disease. Nat Med. 2017; 23: 579-589.