
Journal of Gastroenterology Research and Practice
Short Report - Open Access, Volume 3
Donut-like esophageal leiomyoma enucleation in very critical patient
Duranti Leonardo*; Tavecchio Luca
Thoracic Surgery, Fondazione IRCCS Istituto Nazionale Tumori, Milan, Italy.
*Corresponding Author : Leonardo Durant
Thoracic Surgery, Fondazione IRCCS Istituto Nazionale
Tumori, Milan, Italy.
Email: leonardo.duranti@istitutotumori.mi.it
Received : Jul 19, 2023
Accepted : Aug 17, 2023
Published : Aug 24, 2023
Archived : www.jjgastro.com
Copyright : © Duranti L (2023).
Abstract
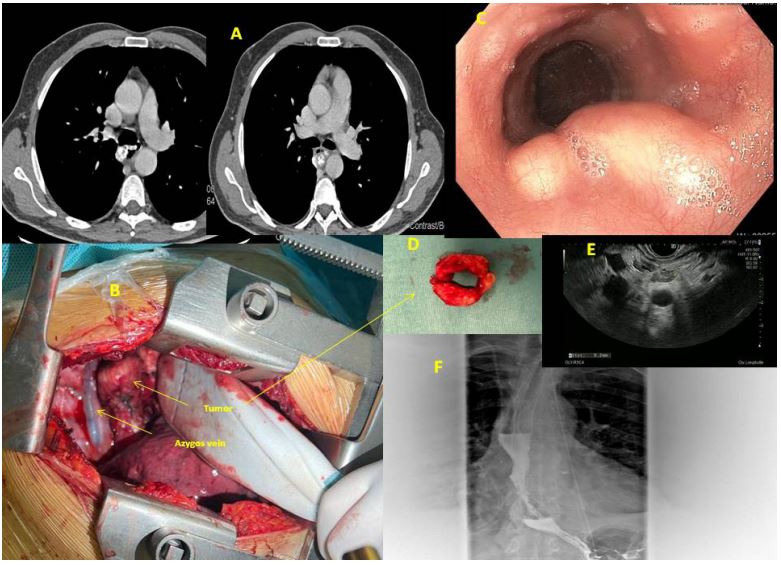
We present here a case of 61 year old man, heavy smoker with hepatic cirrhosis Child-Pugh A alcohol associated. Patient underwent endoscopy and chest CT scan beacause of severe dysphagia and cough. The diagnosis was mid-esopahgeal leiomyoma. We performed a complete enucleoresection of leiomyoma of the midesophagus with direct reconstruction of the muscular wall of the esophagus. This leiomyoma was shaped such as Donut-like (Figure 1). The patient was discharged after 9 days and he was very good with free diet.
Citation: Leonardo D, Luca T. Donut-like esophageal leiomyoma enucleation in very critical patient. J Gastroenterol Res Pract. 2023; 3(6): 1154.
Introduction
Esophageal leiomyomas are benign mesenchymal esophageal tumors, typically involving the distal two-thirds of the esophagus. They are uncommon, and they represent less than 10% of esophageal tumors [1].
Case presentation
A 61-year-old man, heavy smoker with cirrhosis Child-Pugh a alcohol associated, was admitted for surgery. The lesion had a donut-like shape and arised from the muscular layer of the midesophagus. The patient was studied with CT scan, Endoscopy and EBUS with biopsy and with PET scan showing a SUVmax = 1,9 [2]. Because of the poor functional value of spirometry and DLCO, we preferred a fast mono-pulmonary ventilation, so we choosed right lateral muscle-sparing thoracotomy of about 12 cm. The other reason to perform an open surgical access, was the cirrhosis: we were very afraid that a smallest hole in esophageal mucosa could have constituted a high risk of fistula with catastrophic outcome. So we performed a very careful myotomy and enucleoresection of the leomyoma with very great attention to separate the tumor from the mucosa which was very tiny and fragile because of tumoral growth, consistency and weight. The tumor was entirely enulceoresected and the mucosa remained intact [3]. During the hospitalization, we had to control him 3 times every day, with great attention to hepatic function, especially coagulative blood tests and albumin and protein serum levels. Nevertheless, the drainage was removed in eighth post-operative day, when the out-put was <300 ml. We began to reefed the patients after 5 days, previous gastrographin swallow and blu/methylene test. The patient was discharged after 9 days, he was very good with free diet.
Conclusion
Although the esophageal leiomyoma are treated with miniinvasive technique (as we usually do) [4,5], in this very difficult patient we are very happy and proud to have choosed the right lateral thoracotomy. Because of our previous experience of leiomyoma, we knew that is a delicate surgery and that very serious problems such as fistula or esophageal longitudinal laceration could be created. So we treated this esophagus such as crystal glass, dissecting one millemeter for one millimetre, all the contact area between the tumor and mucosa and for 360 degree because of its shape.
Conflict of interest: None.
References
- Punpale A, Rangole A, Bhambhani N, et al. Leiomyoma of esophagus. Ann Thorac Cardiovasc Surg. 2007; 13: 78-81
- Sun LJ, Chen X, Dai YN, et al. Endoscopic ultrasonography in the diagnosis and treatment strategy choice of esophageal leiomyoma. Clinics (Sao Paulo). 2017; 72: 197-201
- Bonavina L, Segalin A, Rosati R, Pavanello M, Peracchia A. Surgical therapy of esophageal leiomyoma. J Am Coll Surg. 1995; 181: 257-62.
- Xu H, Li Y, Wang F, Wang W, Zhang L. Video-Assisted Thoracoscopic Surgery for Esophageal Leiomyoma: A Ten-Year SingleInstitution Experience. J Laparoendosc Adv Surg Tech A. 2018; 28: 1105-8.
- Kemuriyama K, Motoyama S, Sato Y, Wakita A, Nagaki Y, et al. Robot-assisted thoracoscopic enucleation for a large esophageal leiomyoma: a case report. Surg Case Rep. 2021; 7: 129.