
Journal of Gastroenterology Research and Practice
Case Report - Open Access, Volume 3
Ulcerative colitis and autoimmune hemolytic anemia in adult male patient: A rare case report
Mahmoud Ahmad Abdallah1; Taha Mahmoud AlBaik1; Ahmed Tayseer Ibrahim1; Abdulrahaman Al-Toos1; Ezat Mohammed Anini1; Asala Mohammad Awaysa2*; Layth Al- Karaja2; Mosab Samamra1; Laith Alamlih3
1Palestine Polytechnic University, Hebron, Palestine.
2Al-Quds University, Jerusalem, Palestine.
3Hebron University, Hebron, Palestine.
*Corresponding Author : Asala Mohammad Awaysa
Palestine Polytechnic University, Hebron, Palestine.
Email: asalaawaysa98@gmail.com
Received : Feb 13, 2023
Accepted : Mar 20, 2023
Published : Mar 27, 2023
Archived : www.jjgastro.com
Copyright : © Awaysa AM (2023).
Abstract
Autoimmune Haemolytic Anemia (AIHA) as a manifestation of Ulcerative Colitis (UC) is a rare occurrence. This case report describes a 21-year-old male patient diagnosed with UC who was treated with medication, but 11 months later developed Coombs-positive AIHA. Although AIHA in UC patients is more commonly observed in females with pancolitis, the exact mechanism behind this phenomenon remains unclear. This case report presents a theory that sheds light on the potential underlying mechanisms.
Keywords: Inflammatory bowel disease; Ulcerative colitis; Autoimmune hemolytic anemia; Extraintestinal manifestations; Rare case report
Citation: Abdallah MA, AlBaik TM, Ibrahim AT, Al-Toos A, Awaysa AM, et al. Ulcerative colitis and autoimmune hemolytic anemia in adult male patient: A rare case report. J Gastroenterol Res Pract. 2023; 3(2): 1134.
Introduction
Inflammatory Bowel Disease (IBD), which includes Crohn’s disease and ulcerative colitis, is a long-term inflammatory condition of the intestinal mucosa. IBD comprises a complicated interaction between genetic, environmental, or microbial factors and immune responses, despite the fact that the etiology is still largely unclear [1]. Although ulcerative colitis and Crohn’s disease have many similar clinical characteristics, they are treated substantially differently. Endoscopy and cross-sectional imaging that reveals intestinal inflammation are the primary diagnostic tools. Ideally, a sample is taken, and either CD or UC is confirmed by histology and the disease pattern [2]. Patients with Inflammatory Bowel Disease (IBD), which can affect any organ in the human body, may have a wide range of Extraintestinal Manifestations (EIMs).
One of the most typical extraintestinal symptoms of Inflammatory Bowel Disease (IBD) is anemia. It can be asymptomatic or accompanied by vague symptoms including anorexia, agitation, headaches, fatigue, and dizziness, and due to their subtle onset, lack of standardized screening procedures, and potential underappreciation that treating anemia is equally necessary while treating IBD, anemia and iron deficiency in these patients may be underestimated. The pathogenesis of anemia in IBD patients is frequently multifaceted and includes iron deficiency, anemia from chronic inflammation and illness, vitamin deficiencies, hemolysis, and drug-induced myelosuppression [3].
The reported prevalence of anemia in IBD patients ranges from 6% to 74% [4], and the two primary IBD-related kinds of anemia, Iron Deficiency Anemia (IDA) and Anemia of Chronic Disease (ACD), are experienced by the majority of patients. Autoimmune Hemolytic Anemia (AIHA) is an EIM since it involves an organ other than the GI tract and does not originate from IBD inflammation. IBD patients seldom develop AIHA, and most cases that have been recorded have been found in UC patients [4].
Case presentation
A 21-year-old male patient with no prior medical history presented with progressive rectal bleeding (6 times per day), abdominal discomfort, and face pallor for the past month. On admission, the patient had fatigue, dizziness, tachycardia, tachypnea, and shortness of breath.
Laboratory findings on admission showed low hemoglobin levels (Hgb 6.2 g/dL), MCV (71 fL), MCH (21 pg), and low iron levels (16.15 mcg/dL) with normal WBC, platelet count, and TIBC. After blood transfusion of two units, repeat laboratory tests revealed a slightly increased hemoglobin level (Hgb 9.6 g/ dL), MCV (77.3 fL), and MCH (23.5 pg) with normal WBC and platelet count.
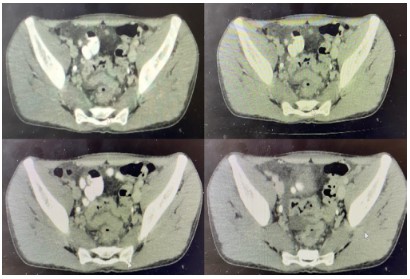
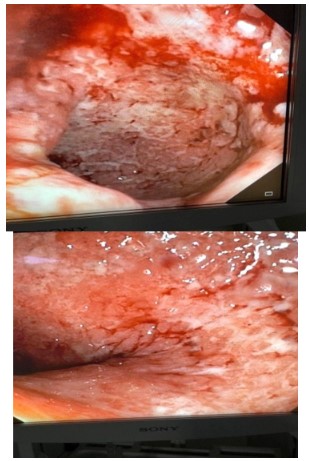
A CT scan showed chronic inflammatory changes in the sigmoid and rectum, perirectal lymph node enlargement, and a small amount of free fluid in the pelvis. A colonoscopy revealed severe left-sided recto-segmoiditis, as classified by Mayo type 3 (as shown in figure 1). Biopsy confirmed the presence of active chronic ulcerative colitis.
The patient was treated with a combination of prednisolone, mesalazine, azathioprine, rafassal, iron, and folic acid for 8 weeks. 11 months later, the patient returned with generalized weakness and jaundice. Laboratory findings showed low hemoglobin levels (Hgb 6.4 g/dL), low MCV (122 fL), high MCH (43.9 pg), elevated CRP (14.28 g/L), ESR (95 mm/hr), total and direct bilirubin levels, reticulocytes and lactate dehydrogenase, leading to a diagnosis of autoimmune hemolytic anemia. The patient was treated with folic acid, Imuran, prednisolone, Nexium, and calcium with vitamin D for 2 months.
Discussion
The present study reports a rare case of Ulcerative Colitis (UC) associated with Autoimmune Hemolytic Anemia (AIHA). Extraintestinal manifestations (EIMs) are commonly seen in UC patients, occurring in 15% of all UC patients, regardless of age [5]. EIMs typically involve the musculoskeletal and dermatologic systems, but can also affect the hepatopancreatobiliary, ocular, renal, and pulmonary systems. Anemia is a frequent occurrence in UC and can result from anemia of chronic disease, iron deficiency anemia, or, rarely, AIHA.
According to previous studies, the prevalence of AIHA in UC patients ranges from 0.2-1.7% [1]. There are gender differences in the incidence of AIHA in UC patients, with females being the predominant gender affected [6,7]. The majority of UC patients with AIHA have pancolitis, while isolated left-sided colonic involvement is less common [8,9].
In the current case, we report a male patient with isolated sigmoido-proctitis and AIHA. The patient was treated with a combination of oral and topical medications, including prednisolone, calcium, iron and folic acid, mesalazine enema, azathioprine, and oral mesalazine. The patient was prescribed a prednisolone dose of 60 mg once daily for 8 weeks, with a gradual tapering to discontinuation over a period of 8 weeks. Additionally, the patient received calcium at a dose of 600 mg once daily, iron and folic acid once daily for 8 weeks, mesalazine enema twice daily for 2 weeks, followed by once daily at night, azathioprine at a dose of 50 mg twice daily, and oral mesalazine at a dose of 500 mg four times daily for 8 weeks.
In conclusion, this case highlights the rare but possible occurrence of AIHA in UC patients, according to one of the most popular theories, the UC-affected colon wall absorbs non-specific, non-red-cell antigens that later trigger an immune reaction and additional cross-reactivity of antibodies made against those antigens and circulated red blood cells [8-10] and the importance of considering this diagnosis in patients with UC presenting with anemia. Furthermore, the treatment approach used in this case may provide valuable information for managing similar cases in the future.
Conclusion
It is unclear exactly how ulcerative colitis and AIHA are related. According to one of the most popular theories, the UC-affected colon wall absorbs non-specific, non-red-cell antigens that later trigger an immune reaction and additional cross-reactivity of antibodies made against those antigens and circulated red blood cells [8-10].
However, further investigation is required to fully comprehend the precise cause of AIHA in UC. Whether the cause is UC itself or the drug that use to treat it.
References
- Zhang YZ, Li YY. Inflammatory bowel disease: pathogenesis. World J Gastroenterol. 2014; 20: 91-99.
- Flynn S, Eisenstein S. Inflammatory Bowel Disease Presentation and Diagnosis. Surg Clin North Am. 2019; 99: 1051-1062.
- Goyal A, Zheng Y, Albenberg LG, Stoner NL, Hart L, et al. Anemia in Children with Inflammatory Bowel Disease: A Position Paper by the IBD Committee of the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr. 2020; 71: 563-582.
- Toplicanin A, Toncev L, Matovic Zaric V, Sokic Milutinovic A. Autoimmune Hemolytic Anemia in Inflammatory Bowel Disease-Report of a Case and Review of the Literature. Life (Basel). 2022; 12: 1784.
- Lakatos L, Pandur T, David G. Balogh Z, Kuronya P, et al. Association of extraintestinal manifestations of inflammatory bowel disease in a province of western Hungary with disease pheno-type: Results of a 25-year follow-up study. World J. Gastroenterol. 2003; 9: 2300-2307.
- Lorber M, Schwartz LI, Wassermann LR. Association of antibody-coated red blood cells with ulcerative colitis; report of four cases. Am J Med. 1955; 19: 887-894.
- Gumaste V, Greenstein AJ, Meyers R, Sachar DB. Coombs-positive autoimmune hemolytic anemia in ulcerative colitis. Dig Dis Sci. 1989; 34: 1457-1461.
- Ramakrishna R, Manoharan A. Auto-immune haemolytic anaemia in ulcerative colitis. Acta Haematol. 1994; 91: 99-102.
- Veloso FT, Carvalho J, Magro F. Immune-related systemic manifestations of inflammatory bowel disease. A prospective study of 792 patients. J Clin Gastroenterol. 1996; 23: 29-34.
- Shashaty GG, Rath CE, Britt EJ. Autoimmune hemolytic anemia associated with ulcerative colitis. Am J Hematol. 1977; 3: 199-208.