
Japanese Journal of Gastroenterology Research
Research Article - Open Access, Volume 2
The changes of Chinese patients’ medical behavior in surgical emergency under the impact of COVID-19 outbreak
Zheng
Department of General Surgery, Beijing Jishuitan Hospital, 31 Xinjiekou East Street, Xicheng District, Beijing, 100035, China.
*Corresponding Author : Zheng
Department of General Surgery, Beijing Jishuitan Hospital, 31 Xinjiekou East Street, Xicheng District, Beijing, 100035, China.
Email: pollitzheng@sina.com
Received : Jul 07, 2022
Accepted : Aug 02, 2022
Published : Aug 09, 2022
Archived : www.jjgastro.com
Copyright : © Zheng (2022).
Abstract
Objective: This research aims to analyze the changes of Chinese patients’ medical behavior in surgical emergency during the COVID-19 outbreak period.
Methods: The retrospective study was designed to observed the impact of patients’ behavior in the department of surgical emergency in Beijing Jishuitan Hospital around the COVID-19 pandemic (2019-2021). We analyzed the numbers of patients in the different periods, and the gender, age, the type of disease, time from onset to consultation, fever and treatment options of patients who came to our emergency surgery around the pandemic.
Results: The number of patients visiting the surgical emergency were 4676 in pre-COVID-19 period (2019), 4275 patients in during-COVID-19 period (2020), and 10832 patients in vaccination-COVID-19 period (2021). The total patients decreased in 2020 compared with that before the pandemic, by about 8.6% (401/4676), and decreased by 20% (472/2363) in the first half of the year, and the number of patients in 2021 was significantly higher than before. There was no significant difference in the gender and the age of the patients (p=0.187, 0.106, 0.530). The number of patients with acute abdomen was significantly higher in the during-COVID-19 period (2020) than that in the pre-COVID-19 period (2019) (p=0.007). The time of patients were much later in 2020 than 2019, and more patients received surgical treatment and more patients with fever between the periods p=0.000, 0.000, 0.000. We also observed the similar results between 2020 and 2021(p=0.001, 0.000, 0.000, 0.000).
Conclusion: Due to the outbreak of COVID-19, patients in surgical emergency department were significantly reduced, but the condition was relatively more serious. The vaccination of new coronavirus vaccine and the corresponding policies adopted after the outbreak, people began to gradually return to normal life and medical behavior.
Keywords: Coronavirus disease 2019 (COVID-19); Surgical emergency; Acute abdomen; Medical behavior.
Citation: Zheng. The changes of Chinese patients’ medical behavior in surgical emergency under the impact of COVID-19 outbreak. Japanese J Gastroenterol Res. 2022; 2(11): 1103.
Introduction
The COVID-19 pandemic has been threatening the public’s health more than two years, since it was diagnosis from the end of 2019 in Wuhan in China. The first official confirmation of novel coronavirus (known as the COVID-19) from the World Health Organization (WHO) on January 9, 2020, which was detective as a new type of infectious coronavirus [1-3]. Then the COVID-19 became widespread worldwide and classified as a pandemic.
The infectious disease has spread globally resulting in over 400 million diagnoses and more than 5 million deaths by December 2021. Since the pandemic outbreak, it has not only affected the health of the population, but also dramatically changed the psychological state, lifestyle and economic status. The public emotion great changes were mainly due to fear of the virus, the loss of relatives, closed isolation, social distancing, fear of vaccine’s safety and economic difficulties [4-6]. The war against COVID-19 has begun in various countries, including strengthen instituted quarantines and personal protections. The preventive behaviors including mask wearing and social distancing have been provided effectively in curbing the spread of the virus, but the preventive vaccine of COVID-19 has shown the advantages of long-term control of the pandemic [7,8]. With strict restrictions on movement helped reduce the transmission of disease, and the social and economic policies had an adverse impact on the healthcare all over the world [9-11]. However, with the vaccination and popularization of the new coronavirus vaccine and the decline of mortality, people’s economic life began to return to normal gradually. Here, we present a perspective on access and barriers to healthcare in surgical emergency in China over the time periods: pre-COVID-19, during-COVID-19 and vaccination-COVID-19 periods. According to the situation, our team observed the patients in our hospital surgical emergency from January 2019 to December 2021, and analyzed the influence of the new coronavirus pandemic on the patients’ behaviors [12-14].
Methods
This is a comparative retrospective study base on the COVID-19 impact on the surgical emergency in China. The data was collected from patients visited surgical emergency in Beijing Jishuitan Hospital between January 2019 to December 2021. The year of 2019 was set as pre-COVID-19 period, and the year of 2020 was set as during-COVID-19 period, while 2021 as vaccination-COVID-19 period. In our study, we compared the number of patients and analyzed the patients’ parameters, including gender, age, the type of disease, time from onset to consultation, fever and treatment options of patients who came to our emergency surgery around before and after the pandemic. The diseases of patients came to our department were divided into two types: acute abdomen (such as acute appendicitis, acute biliary tract infection, acute pancreatitis, acute intestinal obstruction, acute gastrointestinal perforation, abdominal trauma, and acute abdominal pain caused by other causes) and other diseases (including soft tissue infection, acute mastitis and other non-abdominal diseases). The treatment of the patients included surgical treatment and conservative treatment. This study was approved by the Ethics Committee of the Beijing Jishuitan Hospital, and informed consent was obtained from all individuals. All the methods were carried out in accordance with relevant guidelines and regulations. The authors declare that there is no conflict of interest.
Patient and public involvement
This is a comparative retrospective study. All the research questions and outcome measures were informed by telephone and interview. These patients were selected from the patients in the surgical emergency department our hospital. We have already asked the patients to assess the burden of the intervention and time required to participate in the research.
Statistical analysis
The statistical analysis on data was conducted with SPSS 21.0 statistical software. Enumeration data were analyzed by chi-square χ2 test. Measurement data were expressed as mean ± standard deviation and analyzed by t-test. The statistical significance was declared if p < 0.05.
Results
Comparison of the patients attending surgical emergency around the COVID-19 pandemic periods
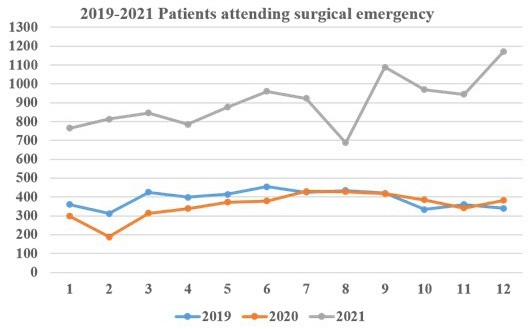
A total of 4676 patients attended surgical emergency department in pre-COVID-19 period (2019), and 4275 patients in during-COVID-19 period (2020), and 10832 patients in vaccination-COVID-19 period (2021). In pre-COVID-19 period (2019), there were 2595 males and 2081 female, 2313 males and 1962 females in during-COVID-19 period (2020), and 6018 males and 4814 females in vaccination-COVID-19 period (2021). The total patients decreased compared with that before the pandemic, by about 8.6% (401/4676), and decreased by 20% (472/2363) in the first half of the year. During the outbreak of COVID-19 in China (2020), the number of patients in the first half of the year (January to June 2020) decreased significantly compared with that in pre-COVID-19 period, and gradually increased to the level before the COVID-19 onset in the second half of the year while the pandemic gradually eased. With the vaccination across the country, the number of patients came to our surgical emergency was significantly higher than before (Figure 1). For the patients with acute abdomen, the similar results were observed in our study. In the first half of 2020, the number of patients with acute abdomen decreased nearly by 16.0% (279/1747), and the number of patients obviously ascended in vaccination-COVID-19 period (2021) (Figure 2).

The diagnosis and treatment of patients around the COVID-19 pandemic periods
There was no significant difference in the gender of the patients visited surgical emergency between pre-COVID-19 period (2019) and during COVID-19 period (2020) (p=0.187). And we didn’t find the significant difference of the mean age between the two groups (57.08±0.95 vs. 55.47±1.00, p=0.058). The similar results were observed in 2020 and 2021 (p=0.106, 0.530). The number of patients with acute abdomen was significantly higher in the during-COVID-19 period than that in the pre-COVID-19 period (p=0.007). The time of the patients who visited surgical emergency was much later in the during-COVID-19 period than that in the pre-COVID-19 period, and more than one in five patients in the during-COVID-19 (p=0.000). And more patients received surgical treatment in the during-COVID-19 period, the difference between the two periods was statistically significant (p=0.000). The patients with fever increased significantly in the during-COVID-19 period than before the pandemic (2019) (p=0.000) (Table 1). We also found that the type of disease, treatment, visit time and fever or not were significantly different between the during-COVID-19 period and the vaccination-COVID-19 period (2021) (p=0.001, 0.000, 0.000, 0.000) (Table 2).
Table 1: The comparison of patients’ parameters in 2019 and 2020.
|
Year |
p |
|
2019 |
2020 |
||
Gender |
|
|
0.187 |
Male |
2595 (55.5%) |
2313 (54.1%) |
|
Female |
2081 (44.5%) |
1962 (45.9%) |
|
Age |
57.08±0.946 |
55.47±0.998 |
0.058 |
Disease Type |
|
|
0.007 |
Acute abdomen |
3443 (73.6%) |
3254 (76.1%) |
|
Other diseases |
1233 (26.4%) |
1021 (23.9%) |
|
Treatment |
|
|
0.000 |
Surgical treatment |
385 (8.2%) |
506 (11.8%) |
|
Conservative treatment |
4291 (91.8%) |
3769 (88.2%) |
|
Fever |
|
|
0.000 |
Yes |
167 (3.6%) |
254 (5.9%) |
|
No |
4509 (96.4%) |
4021 (94.1%) |
|
Visit time |
|
|
0.000 |
<24h |
4064 (86.9%) |
3352 (78.4%) |
|
≥24h |
612 (13.1%) |
923 (21.6%) |
|
Table 2: The comparison of patients’ parameters in 2020 and 2021.
|
Year |
p |
|
2020 |
2021 |
||
Gender |
|
|
0.106 |
Male |
2313 (54.1%) |
6018 (55.6%) |
|
Female |
1962 (45.9%) |
4814 (44.4%) |
|
Age |
55.47±0.998 |
56.38±1.046 |
0.530 |
Disease Type |
|
|
0.001 |
Acute abdomen |
3254 (76.1%) |
7959 (73.5%) |
|
Other diseases |
1021 (23.9%) |
2873 (26.5%) |
|
Treatment |
|
|
0.000 |
Surgical treatment |
506 (11.8%) |
789 (7.3%) |
|
Conservative treatment |
3769 (88.2%) |
10043 (92.7%) |
|
Fever |
|
|
0.000 |
Yes |
254 (5.9%) |
348 (3.2%) |
|
No |
4021 (94.1%) |
10484 (96.8%) |
|
Visit time |
|
|
0.000 |
<24h |
3352 (78.4%) |
9205 (85.0%) |
|
≥24h |
923 (21.6%) |
1627 (15.0%) |
|
Discussion
In pre-COVID-19 period, there was little excessive restrictions of healthcare services for patients in 2019. All this has changed dramatically since the onset of the COVID-19 pandemic in 2020. With the gradual aggravation of the pandemic, people's medical behavior began to be limited. According to the decreasing of confirmed cases and the control of the pandemic, patients began to gradually increase their normal medical behavior. In 2021, the new coronavirus vaccine began to be vaccinated on a global scale. So far, the number of vaccinations in China had exceeded 3 billion, and the number of consulted patients had also begun to increase significantly. Not only the impact of the virus and vaccine, but also the changes of people’s work, life and economic conditions have directly or indirectly changed people’s medical behavior. The cause of healthcare access was complex, and it was affected by individual will, influence of others, and community health service [15,16]. Under the influence of the pandemic, even the distance of the patients from hospitals has become one of the factors affecting the patients going to the hospital. Lack of effective treatment of pandemic and easy transmission had a great impact on the psychology and behavior of patients [17,18]. Since the outbreak of COVID-19 pandemic, patients began to hesitate and feel uneasy before coming to the hospital. Therefore, compared with before the pandemic, they went to the hospital for treatment later and the number of patients also decreased [19].
During the pandemic period, due to the isolation and closure policy, the total number of patients going to the outpatient clinic reduced, and when people have acute symptoms, they will go to the hospital emergency. In our study, we observed the impact of pandemic on patients visiting surgical emergency. In the during-COVID-19 period (2020), the number of patients in surgical emergency decreased by nearly 10% compared with that in pre-COVID-19 period, while the number in the first six months decreased by 20%. With the improvement of the pandemic situation in China, people's medical behavior began to change, and more and more patients with surgical symptoms began to go to emergency surgery. Therefore, the number of patients began to increase in the second half of the year, which was gradually flat with that before the pandemic. By 2021, with the nationwide popularization and vaccination of the new coronavirus vaccine, people began to gradually return to normal work and life, and the number of people seeking medical treatment began to increase rapidly, which is also consistent with our observation. We also found the similar results for the most common patients with acute abdomen in surgical emergency department during the periods. Moreover, more patients with fever or later visiting to the surgical emergency during the pandemic than in the pre-COVID-19 period and vaccination-COVID-19 period. For the most common acute abdomen patients, the proportion of patients during the pandemic is also higher, and more patients had received surgical treatment. The reason for this is that people's fear of new coronavirus pneumonia, isolation and close management of the areas diagnosed or suspected, and even the distance from the patient's home to the hospital and so on may affect the patient's surgical emergency treatment during the COVID-19 outbreak in 2020. Until the patient has a serious condition and fever, the patient has to go to the hospital for treatment, and the time from onset to surgical emergency will be significantly prolonged. Because of more patients with serious diseases, although the total number is small, the proportion of patients undergoing surgical treatment had increased, which was an effective means to quickly alleviate the condition. With the effective control of China's COVID-19, although there are intermittent outbreaks and repeated outbreaks, it has not affected the medical behavior of patients, especially after vaccination.
However, there is no a targeted therapy for COVID-19, the early detection through nucleic acid detection and low dose lung CT, and the vaccination became to be an effective prevention method for COVID-19. After its clinical development, a COVID-19 vaccine will also face the challenge of acceptance by the general population in a post-crisis context [20]. But more and more evidence showed that the risk of COVID-19 infection has been reduced, and the symptoms after infection are also lighter. Therefore, more and more people have been vaccinated, and people are also confident that they will begin to enter normal life with decreased fear of virus. At the same time, people also began to try internet medical consultation and telemedicine, more patients began to pay attention to their health status, and will take the initiative to visit the doctor in hospital emergency when the disease appears in the early stage [21-23]. One limitation of our study is the relatively modest number of surgical emergency patients during the initial pandemic at our center, which likely reflects a combination of variables. The most prominent contributing factor is likely the geographic heterogeneity of the pandemic, even in Beijing, because of the incidence of COVID-19 cases and regional segregation policies in different areas.
Conclusion
Due to the outbreak of novel coronavirus pneumonia, patients in surgical emergency department were significantly reduced, but the condition was relatively serious. With doctors' in-depth understanding of the disease, the vaccination of new coronavirus vaccine and the corresponding policies adopted after the outbreak, people began to gradually return to normal life and medical behavior.
Ethics statement: This study was approved by the Ethics Committee of the Beijing Jishuitan Hospital, and informed consent was obtained from all individuals.
References
- WHO. Novel Coronavirus (2019-nCoV) Situation ReportJ.. World Health Organization, 2020.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumoniaJ. N Engl J Med. 2020; 382: 1199-1207.
- World Health Organization. Who coronavirus disease (COVID-19) Dashboard: World Health organization. 2020.
- Nicola M, Alsafi Z, Sohrabi C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): A reviewJ.. International Journal of Surgery. 2020; 78: 185-193.
- Lwin M, Lu J, Sheldenkar A, et al. Global sentiments surrounding the COVID-19 pandemic on twitter: Analysis of twitter trends J.. JMIR Public Health and Surveillance. 2020; 6: e19447.
- Otu A, Ebenso B, Labonte R, et al. Tackling COVID-19: can the African continent play the long game?J.. J Glob Health. 2020; 10: 010339.
- World Health Organization. Coronavirus disease (COVID-19) advice for the publicJ.. World Health Organization. 2020.
- Zaheer Allam. The Rise of Machine Intelligence in the COVID-19 Pandemic and Its Impact on Health PolicyB.. Urban Health, Data Technology and Political Economy. 2020; 89-96.
- Yang G, Zhang H, Yang Y. Challenges and Countermeasures of Integrative Cancer Therapy in the Epidemic of COVID-19J.. Integr Cancer Ther. 2020; 19: 1534735420912811.
- Omigbodun A, Lilford R. COVID-19: locking down urban settlements in sub-Saharan AfricaJ.. NIHR ARC West Midlands News Blog. 2020; 2: 3–4.
- Wilkinson A, Ali H, Bedford J, et al. Local response in health emergencies: key considerations for addressing the COVID-19 pandemic in informal urban settlementsJ.. Environ Urban. 2020: 095624782092284.
- A Al-Jabir, A Kerwan, M Nicola, et al. Impact of the Coronavirus (COVID-19) pandemic on surgical practiceJ.. Int J. Surg. 2020: S1743-9191(20)30405-2.
- Royal College of Surgeons of England, Guidance for Surgeons Working During the COVID-19 Pandemic. 2020.
- COVID-19: elective case triage guidelines for surgical care, https://www.facs.org/covid-19/clinical-guidance/ elective-case.
- Levesque J-F, Harris MF, Russell G. Patient-Centered access to health care: conceptualizing access at the interface of health systems and populationsJ.. Int J Equity Health 2013; 12: 18.
- Fuhrman S, Kalyanpur A, Friedman S, et al. Gendered implications of the COVID-19 pandemic for policies and programs in humanitarian settings. BMJ Glob Health 2020; 5: e002624.
- Dong RQ, Zhou X, Jiao XN, et al. Psychological Status in Medical Isolation Persons during Outbreak of COVID-19J.. Rehabilitation Medicine. 2020; 30: 7-10.
- Liu B, Sun HY, Wang WJ. Cognition, Attitude and Behavior for COVID-19 among Medical StudentsJ.. Medical Education Research and Practice 2020; 28: 214-217.
- Liu Y, Wang Z, Shen H, et al. Assessment of the global status of COVID-19 pandemicsJ.. J Pub Health Prev Med. 2021; 32: 319-326.
- Detoc M, Launay O, Dualé C, et al. Barriers and motivations for participation in preventive vaccine clinical trials: experience of 5 clinical research sites. Vaccine. 2019; 37: 6633-6639.
- K. Nandra, G. Koenig, A. DelMastro, E. Mishler, J.E. Hollander, C.J. Yeo, Telehealth provides a comprehensive approach to the surgical patient, Am. J. Surg. 2019; 218: 476-479.
- R.L. Gunter S. Chouinard, S. Fernandes-Taylor, Current use of telemedicine for post discharge surgical care: a systematic review, J. Am. Coll. Surg. 2016; 222: 915-927.
- Zhang Yunqiu, Zhang Huifang. Research on People’s Medical-seeking Behavior Under COVID-19 EpidemicJ.. Medicine and Society. 2021; 34: 7-11.