
Japanese Journal of Gastroenterology Research
Case Report - Open Access, Volume 2
A snared loop on top of malrotation in association with situs inversus, a report of rare presentation
Ahmed Elrouby1*; Ahmed Maher2
1 Associate Professor of Pediatric Surgery, Faculty of Medicine, Alexandria University, Egypt.
2 Assistant lecturer of Pediatric Surgery, Faculty of Medicine, Alexandria University, Egypt.
*Corresponding Author : Ahmed Elrouby
Faculty of Medicine, Alexandria University, Egypt.
Email: elroubypaedo@yahoo.co
Received : Dec 06, 2021
Accepted : Jan 21, 2022
Published : Jan 28, 2022
Archived : www.jjgastro.com
Copyright : © Elrouby A (2021).
Abstract
Introduction: The association of intestinal malrotation with situs inversus is found in 40-90% of such patients.
Case report: We report a case with this association who was presented to our institute with bilious vomiting, constipation and abdominal distension. Plain x-ray abdomen standing showed multiple air fluid levels with laboratory investigations showing evidence of profound sepsis. Surgical exploration revealed situs inversus with malrotation and snared loop of the terminal ileum. Ladd’s procedure with resection of the ileal loop and ileo-colic anastomosis.
Conclusion: The outcome in such cases is favorable except in case of profound sepsis or co-morbid fatal associations.
Keywords: situs inversus; malrotation; snared loop.
Citation: Elrouby A, Maher A. A snared loop on top of malrotation in association with situs inversus, a report of rare presentation. Japanese J Gastroenterol Res. 2022; 2(2): 1055.
Introduction
The right to left internal body organs arrangement is known as situs. Situs inversus is defined as the reverse of this right to left arrangement [1]. Those patients may pass all of their lives unnoticed until they were evaluated medically for other medical evaluation of un related conditions [2]. It may be either isolated or associated with other congenital anomalies; mostly intestinal malrotation which associates this anomaly in 40-90 % of patients [1]. The report of snared loop in the literature is not frequently found although the association with duodenal and jejunoileal atresia is more commonly reported. We introduce a case of snared loop in a patient with situs inversus.
Case report
A twenty days old male neonate was referred to our pediatric surgery department at Elshatby University Hospital presented with constipation, abdominal distension and persistent vomiting. Vomiting started three days before admission; it was non-bilious in nature in the beginning then it progressed rapidly to be bilious then feculent with increasing amount. On examination the patient was hypoactive, dehydrated, tachycardiac, hypothermic, hypotensive with profound mottling. Local abdominal examination showed massive abdominal distension with visible loops without showing any signs of peritoneal irritation. The patient was immediately admitted to the neonatal intensive care unit when resuscitation was started with intravenous fluid administration, correction of electrolyte imbalance and anti-sepsis regimen.
Plain X-ray abdomen standing showed severe gaseous distension, multiple sharp air fluid levels, and absence of gas distribution in the lower abdomen. The cardiac shadow was obscured (Figure 1).

The patient was transferred to the operating theatre after full resuscitation and stabilization. Under general anesthesia with endotracheal intubation, abdominal exploration was done through right transverse supra-umbilical incision. Massive bowel distension was noticed and after full bowel evisceration; situs inversus was found in addition to bowel malrotation. An abnormal congenital band was found extending from the root of the mesentery to the anterior abdominal wall just beside the umbilicus around which a loop of the terminal ileum was looping (snared) with an area of fibrosis just before the ileo-cecal valve (Figure 2).

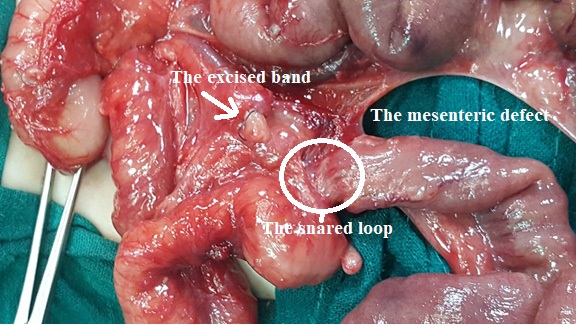
Excision of the congenital band was done after which a large mesenteric defect was found with a white avascular unhealthy ring of the terminal ileum just beside the ileo-cecal valve as shown in (Figures 3,4,5). The liver was found on the left side of the abdomen and stomach the right side with an abnormally located spleen just behind the stomach (stomach bed). Ladd’s procedure was done for malrotation considering the situs inversus. The avascular snared loop of the terminal ileum was resected together with the ileo-cecal region and ileocolic anastomosis was done. The mesenteric defect was closed in Mercedes sign to keep the mesentery broad, considering the vascular blood supply of intestine (Figure 6).



The patient was then transferred to the neonatal intensive care unit where he was mechanically ventilated with profound irreversible septic shock. The stormy post-operative period was resistant to all supportive measures and the patient died six hours later.
Discussion
Situs inversus is a rare congenital anomaly in which the body organs are mirrored from their normal position. Common anomalies associated with situs inversus are cardiac and intestinal anomalies that requiring surgical correction [3]. Situs inversus may not be discovered along life span as it may not be associated with any complaint, Fonkalsrud et al. [4] in their study which included 37 patients having situs inversus, reported that 15 patients (40%) have major correctable abdominal anomalies requiring surgical intervention. Situs abdominus is rarely associated with neonatal intestinal obstruction (midgut volvulus or multiple intestinal atresia), [2] however a more common association is present with situs inversus totalis (all of the normal human anatomy is mirrored or inversed [5]. The presentation of situs inversus with gastrointestinal complaints is considered an emergency. Intestinal obstruction in such conditions issuggested by radiological investigations as abdominal radiographs and contrast study. Abdominal sonography and CT may show the inverse relationship of the mesenteric vessels in case of malrotation and whirlpool sign in superadded volvulus [2].
Other congenital anomalies may be found in case of situs inversus as congenital heart malformations and splenic anomalies [6]. Volvulus on top of malrotation in case of situs inversus may develop in an anti-clockwise direction so a great attention of the direction of rotation should be made in such cases as the intra-operative derotation should be done in a clock wise manner as in our reported case [2]. Pre-operative diagnosis of situs inversus in case of surgical intervention is very important in planning the surgical incision and the intra-operative management plane [3]. The lines of surgical treatment in case of situs inversus totalis in association with intestinal obstruction are the same as in classical cases. After am appropriate laparotomy incision, Ladd’s procedure is performed taking into consideration a clockwise derotation to avoid volvulus if the usual anticlockwise derotation was performed due to the situs inversus. [7, 8].
The mortality associated with patients having situs inversus in combination with malrotation and volvulus without intestinal necrosis is usually attributed to the associated cardiac anomalies. Surgical intervention of malrotation associated with situs inversus in selected patients who have cardiac stability has an acceptable outcome with prevention of midgut volvulus [9].
The patient presented in our report was suffering from profound sepsis on admission which was resistant to all supportive measures and died about six hours post-operative. Ruben et al. reported in his study three deaths from the studied seven neonates who underwent Ladd’s procedure for malrotation associated with situs inversus who were presented with abdominal surgical emergency [9].
Conclusion
The association of malrotation with situs inversus is very common however the presence of snared loop is not usually found. The outcome in such cases is favorable except in case of profound sepsis or co-morbid fatal associations.
Declarations
Conflict of interest statement: We declare that there is no conflict of interest regarding this manuscript to declare.
Funding source: The study had not receive any fund.
Ethical approval: We read and complied with the policy of the journal regarding the ethical consent. A written consent with clear explanation of the procedure was signed by the parents. The ethical committee of our institute had approved the study
Informed consent: An informed consent was signed by the parents accepting publication of this case report.
Agree to conditions: All authors of the manuscript have read and agreed to its content and are accounted for all aspects of the accuracy and integrity of it.
References
- Choi KS, Choi YH, Cheon JE, Kim WS, Kim IO. Intestinal malrotation in patients with situs anomaly: Implication of the relative positions of the superior mesenteric artery and vein. Eur J Radiol. 2016; 85: 1695-700.
- Gupta R, Soni V, Valse PD, Goyal RB, Gupta AK, Mathur P. Neonatal intestinal obstruction associated with situs inversus totalis: two case reports and a review of the literature. J Med Case Rep [Internet]. 2017; 11: 264.
- Chinya A, Naranje K, Mandelia A. Situs inversus abdominalis, polysplenia, complex jejunal atresia and malrotation in a neonate: A rare association. Int J Surg Case Rep [Internet]. 2019; 56: 93-5.
- FONKALSRUD EW. Abdominal Manifestations of Situs Inversus in Infants and Children. Arch Surg [Internet]. 1966; 92: 791.
- Devera J, Licandro F, Ramos J, Taymoorian HT, Yap LG. Situs Inversus Totalis in the Neonatal Setting. Cureus [Internet]. 2021.
- Nawaz A, Matta H, Hamchou M, Jacobez A, Trad O, Salem AH Al. Situs inversus abdominus in association with congenital duodenal obstruction: a report of two cases and review of the literature. Pediatr Surg Int [Internet]. 2005; 21: 589-92.
- Menon P, Mahalik S, Khanna S. Malrotation and volvulus associated with heterotaxy syndrome. J Indian Assoc Pediatr Surg [Internet]. 2012; 17: 138.
- Budhiraja S, Singh G, Miglani HPS, Mitra SK. Neonatal intestinal obstruction with isolated levocardia. J Pediatr Surg [Internet]. 2000; 35: 1115-6.
- Tashjian DB, Weeks B, Brueckner M, Touloukian RJ. Outcomes after a Ladd procedure for intestinal malrotation with heterotaxia. J Pediatr Surg [Internet]. 2007; 42: 528-31.