
Journal of Gastroenterology Research and Practice
Case Series - Open Access, Volume 4
Endoscopic decontamination of massive, modified release venlafaxine overdose
Ho Tuan Tiong*; Jan Kubovy
Department of Gastroenterology, Christchurch Hospital, Waitaha, New Zealand.
*Corresponding Author : Ho Tuan Tiong
Department of Gastroenterology, Christchurch Hospital,
Waitaha, New Zealand.
Tel: +643-364 0920 & +643-364 0419;
Email: Tioho105@gmail.com
Received : Feb 11, 2024
Accepted : Mar 05, 2024
Published : Mar 12, 2024
Archived : www.jjgastro.com
Copyright : © Tuan Tiong H (2024).
Abstract
Pharmacobezoars, which are bezoars comprised of medications, are considered a rare phenomenon encountered in overdose patients. There are no clear recommendations for its diagnosis and management. Altered pharmacokinetics can lead to atypical clinical course. Traditional gastrointestinal decontamination methods have questionable efficacy in these cases and endoscopic decontamination is poised to become the method of choice. We present two cases of massive overdose of modified release venlafaxine associated with gastric pharmacobezoar formation. Diagnosis with computed tomography was convincing in only one case, however, subsequent endoscopy confirmed pharmacobezoar in both patients. The pharmacobezoar was associated with significantly delayed gastric emptying. Subsequent endoscopic decontamination was difficult, but overall feasible and possibly lifesaving. The timing of diagnosis and endoscopic intervention is crucial and the only modifiable factor. Multidisciplinary approach with establishment of local protocol could improve clinical outcomes.
Keywords: Pharmacobezoar; Modified release venlafaxine; Overdose; Endoscopic decontamination.
Citation: Tuan Tiong H, Kubovy J. Endoscopic decontamination of massive, modified release venlafaxine overdose. J Gastroenterol Res Pract. 2024; 4(3): 1189.
Introduction
Bezoar refers to the formation of masses of undigested material within the Gastrointestinal (GI) tract. Medication bezoar, termed pharmacobezoar, can form after ingested drug overdose, particularly of modified release or enteric-coated preparations [1]. Pharmacobezoars can gradually release medication into the GI tract leading to delayed absorption associated with persistently elevated drug levels and prolonged toxicity [2]. Pharmacobezoar can also break down suddenly, leading to a rapidly increasing drug level [2]. In addition, there is a risk of mechanical luminal obstruction. These cases can present with an atypical clinical course and challenging management, especially when the ingested dose of medication is associated with a life threatening toxidrome. Venlafaxine is an antidepressant belonging to the class of Serotonin-Norepinephrine Reuptake Inhibitors (SNRI). It can lead to serotonin syndrome [3] and recalcitrant cardiac arrhythmia [4]. Gastrointestinal decontamination techniques such as activated charcoal or whole bowel irrigation, are important management strategy in patients presenting with venlafaxine overdose [5]. However, pharmacobezoars can challenge this standard of care. Endoscopic decontamination has recently emerged as potential method dealing with these scenarios. Only a handful of case reports are published to date, describing variable techniques and outcomes [6]. We report endoscopic management of two cases of massive overdose of modified release venlafaxine associated with gastric pharmacobezoar formation.
Case 1
A 50-year-old female was found unresponsive at home with suspected intentional multiple drug overdose of modified release (XR) venlafaxine and lamotrigine. The calculated dose amounted to 32.1 g of venlafaxine (209 tablets of 150 mg XR Venlafaxine and 10 tablets of 75 mg SR Venlafaxine [ENLAFAX®XR, manufactured by VIATRIS]) and 23.3 g of lamotrigine (233 tablets of 100 mg Lamotrigine [LOGEM®, manufactured by VIATRIS]). On arrival to Emergency Department (ED), she had reduced level of consciousness with a Glasgow Coma Scale (GCS) of 10 and suffered recurrent seizures. She was hypoxic on room air with 90% oxygen saturation, tachycardic with 146 beats per minute (bpm), but normotensive at 138/71 mmHg. Venous Blood Gas (VBG) showed a pH of 7.27, PCO2 of 52 mmHg, HCO3 of 23.6 mmol/L and an anion gap of 16.3 mmol/L. Initial ECG showed sinus tachycardia without toxic changes.
The patient was intubated and placed on mechanical ventilation in Intensive Care Unit (ICU). A Nasogastric Tube (NGT) was inserted and aspirated pink-coloured fluid. She deteriorated with recurrent broad complex tachycardia, progressive haemodynamic compromise, and incremental seizures.
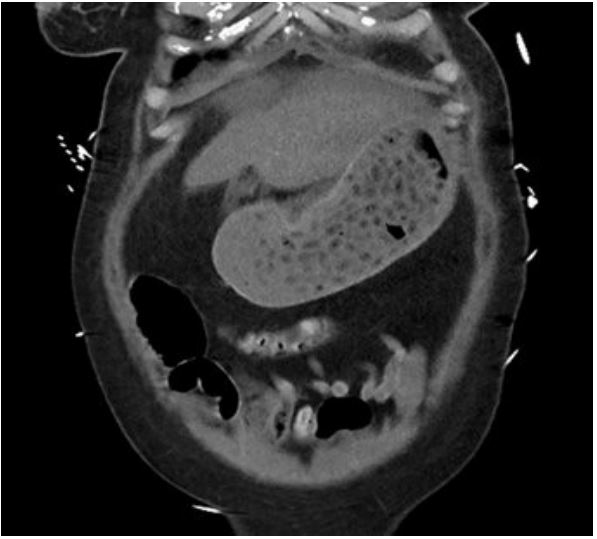
New Zealand National Poison Centre was consulted 30 hours after her initial presentation. The ingested dose of 309 mg/kg of venlafaxine and 224 mg/kg of lamotrigine significantly exceeded the intervention threshold, (12.5 mg/kg and 30 mg/kg for venlafaxine and lamotrigine, respectively) [7,8]. Abdominal cross-sectional imaging and/or urgent gastroscopy was recommended to assess/remove any remaining pill burden. Abdominal Computed Tomography (CT) 36 hours after the initial presentation revealed large pill concretion within gastric lumen (Figure 1). Urgent gastroscopy using therapeutic endoscope (GIF-2TH180, dual channel 3.7 mm and 2.8 mm diameter, Olympus Medical, Japan), found a large conglomerate of tablets in the stomach (Figure 2). Pill retrieval was attempted with a retrieval basket (Meditalia® 30x60 mm Loop Net, Italy) and a polypectomy snare (SnareMaster Plus, 10 mm, Olympus Medical, Japan). The procedure was technically challenging due to the large, compact nature of the concreted pharmacobezoar. The pharmacobezoar could not be easily broken down or removed and significant amount of pill burden remained. A last resort laparotomy was then contemplated to aid gastric decontamination, but the patient was deemed hemodynamically too unstable. She continued to deteriorate despite all available supportive measures and died a few hours later


Case 2
A 27-year-old female with known depression and previous intentional drug overdose presented to ED with a reduced level of consciousness after taking total of 6.75 g (66.2 mg/kg) of XR Venlafaxine (45 tablets of 150 mg XR Venlafaxine [ENLAFAX® XR, manufactured by VIATRIS])) 2 hours earlier. Initial examination revealed an oxygen saturation of 98% on room air, a heart rate of 120 bpm, blood pressure of 160/90 mmHg, and reduced GCS of 12. She had sustained clonus in both her ankles. VBG showed a pH of 7.40, pCO2 of 45 mmHg, HCO3 of 27.7 mmol/L and an anion gap of 14.3 mmol/L. ECG showed sinus tachycardia without toxic changes.
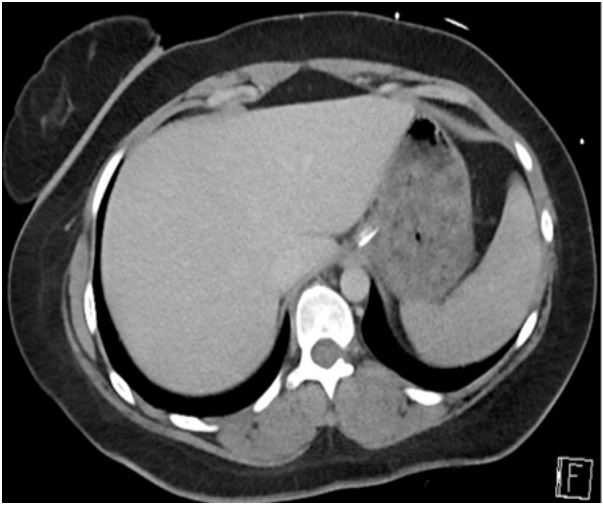
NGT was inserted, aspirating red-colored fluid with pill fragments. Activated charcoal was then administered and urgent abdominal CT scan organized. This revealed a moderate volume of variable attenuation gastric content in the stomach without further characterization (Figure 3).
She was then intubated and placed on mechanical ventilation to facilitate urgent gastroscopy. This was performed 6 hours after the ingestion and revealed a conglomerate of tablets in the stomach with copious adherent activated charcoal (Figure 4). Removal of tablets was challenging due to the presence of charcoal leading to a 2-hour long procedure. The stomach was eventually completely cleared, successfully retrieving large number of pills using a retrieval basket (Meditalia® 30x60 mm Loop Net, Italy). She then received whole-bowel irrigation with around 10 liters of Polyethylene Glycol solution (PEG) over 48 hours. She remained hemodynamically stable and was extubated the following day. She was discharged four days after the initial presentation with psychiatric follow-up.
Discussion
Pharmacobezoar is rare, or at least not commonly encountered due to general lack of abdominal imaging in patients with drug overdose. Consequent to this lack of experience, there are no clear recommendations for its diagnosis and management. While the efficacy of established GI decontamination methods such as activated charcoal and whole-bowel irrigation could be described as uncertain, the role of decontamination endoscopy is uncharted. We found only three case reports of venlafaxine overdose associated with pharmacobezoar involving endoscopic management. Different methods of diagnosis and decontamination were employed with variable outcomes [6]. Our two cases have contrasting clinical outcomes, providing useful insights into the diagnosis, management, and appropriate timing.
Massive venlafaxine overdose is associated with delayed gastric emptying. This, along with the adhesive gelatine capsule of the sustained release drug preparation could lead to the pharmacobezoar formation and its solid, concrete-like nature (concretion) [9]. In case 1, this was seen in stomach 36 hours after ingestion, significantly longer than a standard solid gastric emptying time of around 4 hours. Resultant prolonged absorption can cause delayed or prolonged toxicity [6]. We are uncertain of the effect of co-ingested lamotrigine.
Delayed gastric emptying and pharmacobezoar formation set the stage for endoscopic intervention as possibly the most appropriate method of decontamination. Timely imaging such as CT scan can be invaluable in confirming pharmacobezoar. However, case 2 shows that the presence of pills versus food may not be radiologically distinguishable. Gastroscopy may still be indicated in such cases and indeed be a lifesaving intervention. Nevertheless, we believe that timely cross-sectional imaging (i.e., upon arrival to ED) should guide the indication to urgent gastroscopy, as absence of significant gastric content may render gastroscopy unnecessary.
Our cases also highlight that endoscopic decontamination can be technically challenging. Local expertise and patient’s clinical status should be taken into consideration when contemplating endoscopic decontamination. Our tertiary center had no prior experience with this method. However, given the strong potential for such lifesaving intervention, a local protocol has been put in place in cases of potentially life-threatening overdose. A CT scan on arrival to ED demonstrating potential pharmacobezoar triggers immediate referral for urgent gastroscopy. Case 2 illustrates that administering activated charcoal prior to UGI endoscopy can render endoscopic decontamination difficult if not impossible. As such, activated charcoal should only be considered after endoscopy or when this is unavailable or not indicated. We have no experience with prior administration of PEG solution, but assume that its clarity shouldn’t interfere with subsequent gastroscopy.
The contrasting outcomes of our cases are likely due to multiple factors, including the patient’s age, the dose taken and the timing of presentation relative to ingestion. The only modifiable factor is timing of pharmacobezoar diagnosis and timing of its subsequent management. In case 1, imaging wasn’t performed until 30 hours after the initial presentation. This delay in pharmacobezoar identification and gastroscopy was highly likely detrimental [6].
Conclusion
Potentially lethal overdose requires multidisciplinary approach with involvement of local poison center. If indicated, endoscopic decontamination is feasible and possibly lifesaving method. Pharmacobezoar needs to be considered early during presentation of modified release venlafaxine overdose (and likely other modified release drugs). Timing of pharmacobezoar diagnosis and endoscopic management is crucial, and the right sequence should be protocolized amongst all main stakeholders (including first responders, ED, ICU and endoscopy service).
Conflict of interests: The authors declare that they have no conflict of interest.
Funding: This work received no funding.
References
- Nelson L. As If, There Weren’t Enough Controversies in Gastrointestinal Decontamination. Journal of Toxicology: Clinical Toxicology. 2000. Available from: https://www.tandfonline.com/doi/full/10.1081/CLT-100102007
- Gussow L. Toxicology Rounds: Facts and Fiction about Pharmacobezoars. Emergency Medicine News. 2020; 42: 22.
- Daniels RJ. Serotonin syndrome due to venlafaxine overdose. J Accid Emerg Med. 1998; 15: 333-4.
- Howell C, Wilson AD, Waring WS. Cardiovascular toxicity due to venlafaxine poisoning in adults: a review of 235 consecutive cases. British Journal of Clinical Pharmacology. 2007; 64: 192-7.
- Emergency Management of Poisoning. Haddad and Winchester’s Clinical Management of Poisoning and Drug Overdose. 2007; 13-61.
- Simpson SE. Pharmacobezoars described and demystified. Clin Toxicol (Phila). 2011; 49: 72-89.
- New Zealand National Poisons Centre. Enlafax-XR. 2024. Available from: https://www.toxinz.com/specifications/snris/venlafaxine/enlafax-xr/?&name=Enlafax-XR
- New Zealand National Poisons Centre. Logem. 2024. Available from: https://www.toxinz.com/specifications/lamotrigine/logem/?&name=Logem
- Djogovic D, Hudson D, Jacka M. Gastric bezoar following venlafaxine overdose. Clinical Toxicology. 2007; 45: 735-735.