
Japanese Journal of Gastroenterology Research
Case Report - Open Access, Volume 1
A rare case of cholecystoduodenal fistula and gallstone impaction causing gallstone ileus: A case report
Chiew Junloong1,*; Maizatul Aliaa AM1; Ismazizi Z2; Zainal AA2
1Department of General Surgery, Hospital Sultanah Aminah, Johor Bahru, Johor, Malaysia.
2Department of General Surgery, Hospital Kuala Lumpur, Kuala Lumpur, Malaysia.*Corresponding Author: Chiew Junloong
Medical Officer Surgical Department, Hospital Sultanah Aminah, Johor Bahru, Johor, Malaysia.
Email: chiewjunloong@gmail.com
Received : Sep 25, 2021
Accepted : Nov 09, 2021
Published : Nov 12, 2021
Archived : www.jjgastro.com
Copyright : © Junloong C (2021).
Abstract
Gallstone ileus is a rare cause of gastrointestinal (GI) complication of gallstone that causes mechanical intestinal obstruction due to gallstone impaction in the gastrointestinal tract. About less than 1% of intestinal obstruction is caused by this. Patients may present with non-specific signs and symptoms. Surgical relief of gastrointestinal obstruction remains the mainstay of operative treatment. Classical findings on plain abdominal radiography include (1) pneumobilia; (2) intestinal obstruction; (3) an aberrantly located gallstone; and (4) change of location of a previously observed stone. The current surgical procedures are: (1) simple enterolithotomy; (2) enterolithotomy, cholecystectomy, and fistula closure (one-stage procedure); and (3) enterolithotomy with cholecystectomy performed later (two-stage procedure). We describe a case of gallstone ileus.
Abbreviations: GI: Gastrointestinal; CT: Computerised Tomography.
Citation: Junloong C, Maizatul AAM, Ismazizi Z, Zainal AA. A rare case of cholecystoduodenal fistula and gallstone impaction causing gallstone ileus: A case report. Japanese J Gastroenterol Res. 2021; 1(7): 1034.
Introduction
Gallstone Ileus (GI) is characterized by obstruction of the intestinal lumen as a result of one or more gallstones [1]. According to reports from the 1990s, GI is a rare complication of gallstones that occurs in 1%-4% of all cases of bowel obstruction. The mortality associated with GI ranges between 12% and 27% [2].
In 1941 L.G. Rigler described his famous triad of roentgen manifestations indicating Gallstone Ileus (GSI), that is, the association of an ectopic gallstone, bowel distension, and pneumobilia [10]. The pathogenesis is due to episodes of cholecystitis causing a fistula to develops between the gallbladder and the bowel, most commonly the duodenum. A large gallstone is then able to migrate to the gastrointestinal tract causing a mechanical obstruction. The most common locations of impaction are the terminal ileum and the ileocecal valve due to the small diameter and less active peristalsis.
Case report
A 53 years old female patient, no past medical history, was admitted to our surgical ward for epigastric pain, vomiting, and no bowel opening for the past 3 days. She did not give any history of fever or chills.
On arrival to the Emergency Department, she was not in acute distress with normal vital signs and body temperature. Upon examination, her abdomen was distended, tympanic on percussion, and high-pitched bowel sounds were audible. Digital rectal examination was collapsed rectum with no bogginess or mass.
Laboratory tests demonstrated a normal white blood cell count. Her renal profile and liver function test were within the normal range. Her chest X-ray was normal and did not show any air under diaphragm.
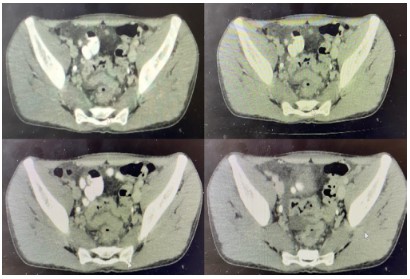
Abdominal X-ray showed a well-defined radiopaque focus seen at the right hypochondriac region in keeping with gallstone. There are loops of dilated small bowel with stacked coin appearance seen at the lower abdomen. There is another radiopaque focus seen projected over the right sacral alar suggestive of gall stone ileus (Figure 1).
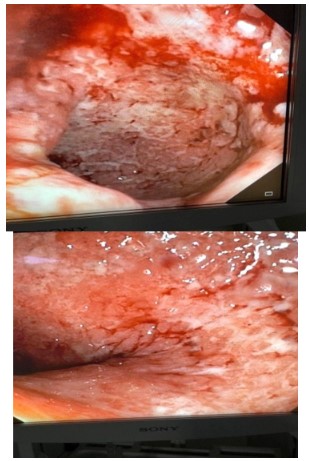
Due to her persistent vomiting and distended abdomen, an orogastric tube was inserted and feculent material drained about 500 cc. Decision made for an urgent exploratory laparotomy. Exploration revealed massively dilated loops of small bowel proximal to the distal ileum. An obstruction was seen at 180 cm from the duodenojejunal junction with a 1 cm size of small bowel perforation at the mesenteric site. Enterotomy was made to reveal a large gallstone 2 X 3 cm. The gallstone was removed, and 10 cm of the small bowel was resected, and an end-to-end anastomosis was done. The gallbladder wall was thickened with multiple small gallstones, and one large gallstone about 2 cm impacted at the Hartmans pouch (Figure 2). There was also a fistula communicating between the Hartmans pouch and the first part of the duodenum, which was repaired primarily with absorbable poly filament suture and omental patch. Cholecystectomy was also performed.
The patient had an uneventful post-operative course and was discharged home on post-operative day 10.
Discussion
Gallstone ileus is more common in women, and the ratio of females to males is 3.5 to 1 [4]. The gallstone may enter the intestine through a fistula, and it can impact anywhere in the gastrointestinal tract. The gallstone must be ≥ 2-2.5 cm in diameter to cause obstruction [5]. As shown by Reisner and Cohen, impaction of the stone can occur in any part of the bowel, i.e., the ileum (60.5% of cases), jejunum (16.1%), stomach (14.2%), colon (4.1%), and duodenum (3.5%). It can also be passed spontaneously (1.3%) [4]. Most frequently is the terminal ileum and the ileocaecal calve because of the narrow lumen and less active peristalsis [7]
Gallstone ileus is more common in elderly patients with comorbidities. The often vague, intermittent symptoms may delay the diagnosis and worsens morbidity and mortality. The patient may have intermittent symptoms of nausea, vomiting, abdominal distention, and pain. More attention should be made to those patients who have a history of cholecystolithiasis and with symptoms of nausea, vomiting, abdominal pain, and distention. However, our patient had an acute intestinal obstruction and led us to a quick decision for surgical intervention.
Classical findings on plain abdominal radiography include (1) pneumobilia; (2) intestinal obstruction; (3) an aberrantly located gallstone; and (4) a change in location of a previously observed stone[9]. Gallstones are radiopaque only in 15-20% of cases [1]. In our patient, we did not proceed with a diagnostic CT abdomen as she had feculent material on her ryles tube free flow; thus, a decision was made for an urgent laparotomy.
GI is a mechanical intestinal obstruction caused by the impaction of gallstones within the lumen of the bowel. Most reports indicate that stones smaller than 2.5 cm usually pass through spontaneously, so conservative treatment (decompression by nasogastric drainage) is conducted before a decision is made to remove the impacted stone by surgical means [8].
Wound infections and dehiscence is known to being the most common complications after surgery in 25% to 50% of GI cases. Other complications such as acute renal failure are also seen in post-operative patients. Gastrointestinal complications related to anastomotic leaks and intra-abdominal abscesses are highest in patients undergoing enterotomy with fistula closure [11].
Laparotomy should involve a systematic and meticulous search for the presence of additional ectopic enteric stones. Enterolithotomy remains the mainstay of operative treatment. A one-stage cholecystectomy and repair of the fistula is justified only in selected patients in good general condition and adequately stabilized preoperatively. Specific criteria for a one-stage procedure remain to be established. Two-stage surgery is an option for patients with persistent symptomatology after enterolithotomy surgery.
Conclusion
Gallstone ileus or gallstone gastrointestinal obstruction represents less than 1% of gastrointestinal obstruction cases, with a higher frequency among the elderly. The patient may present with vague symptoms, which may delay the diagnosis and treatment. Surgical intervention to relieve the obstruction is the mainstay of the treatment. A good judgment in selecting the surgical procedure will help in reducing mortality and morbidity.
Declarations
Ethics approval and consent to participate: This work adheres to the guidelines and principles of the Declaration of Helsinki and is in accordance with the Malaysian Good Clinical Practice (MGCP) 4th edition 2018. This research is also registered with the National Medical Research Register (NMRR), and ethics approval was obtained from the Medical Research and Ethics Committee (MREC) prior to the initiation of the study
Consent for publication: Verbal consent was obtained from the patient.
Availability of data and materials: Not applicable.
Competing interests: The authors declare that they have no competing interests.
Funding: This study was conducted without any funding from any parties.
Authors' contributions: CJ collected the patient's clinic information, searched relevant works of literature, and wrote the manuscript. MAAM was the attending doctor of the patient. IZ & ZAA carried out critical revision and correction of the manuscript. All authors read and approved the final manuscript for submission and publication.
Acknowledgements: We would like to thank the Director-General of Health Malaysia for his permission to publish this article. We also would like to express our gratitude to the Surgical Department of Hospital Sultanah Aminah Johor Bahru, and those who had extended their help in contributing to this manuscript.
References
- Gallstone ileus: An atypical presentation and unusual location. Chatterjee S, Chaudhuri T, Ghosh G, Ganguly A Int J Surg. 2008; 6:e55-6.
- Gallstone ileus: a review of 1001 reported cases. Reisner RM, Cohen JR Am Surg. 1994; 60: 441-6.
- Bortoff GA, Chen MY, Ott DJ et-al. Gallbladder stones: imaging and intervention. Radiographics. 2000; 20: 751-66.
- Surgery for gallstone ileus: a nationwide comparison of trends and outcomes. Halabi WJ, Kang CY, Ketana N, Lafaro KJ, Nguyen VQ, Stamos MJ, Imagawa DK, Demirjian AN Ann Surg. 2014; 259: 329-35.
- Gallstone ileus. Review of 112 patients in the Japanese literature. Kasahara Y, Umemura H, Shiraha S, Kuyama T, Sakata K, Kubota H Am J Surg. 1980; 140: 437-40.
- Gallstone ileus: A review of 1001 reported cases. Reisner RM, Cohen JR Am Surg. 1994; 60: 441.-6.
- Gallstone ileus and jejunal perforation along with gangrenous bowel in a young patient: A case report. Gupta M, Goyal S, Singal R, Goyal R, Goyal SL, Mittal A N Am J Med Sci. 2010; 2: 442-3.
- A case of gallstone ileus with a spontaneous evacuation. Ihara E, Ochiai T, Yamamoto K, Kabemura T, Harada N Am J Gastroenterol. 2002; 97: 1259-60.
- Gallstone ileus: increased diagnostic sensitivity by combining plain film and ultrasound. Ripollés T, Miguel-Dasit A, Errando J, Morote V, Gómez-Abril SA, Richart J Abdom Imaging. 2001; 26: 401-5.
- L. Rigler, C. Borman, and J. Noble, "Gallstone obstruction: pathogenesis and roentgen manifestations," The Journal of the American Medical Association. 1941; 117: 1753–1759.
- Surgery for gallstone ileus: a nationwide comparison of trends and outcomes. Halabi WJ, Kang CY, Ketana N, Lafaro KJ, Nguyen VQ, Stamos MJ, Imagawa DK, Demirjian AN Ann Surg. 2014; 259(2): 329-35.